
Translate this page into:
Unilateral Nevoid/primary Hyperkeratosis of Nipple and Areola Successfully Treated with Radiofrequency Ablation
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 20-year-old unmarried woman presented with a warty growth over the left nipple and areola for the past 2 years. The lesions progressed with respect to the number and size during the initial 6 months. Ever since, the lesions have been stable. It was not associated with any history of pruritus, alteration of the lesion with menstrual cycle, and complications such as ulceration, discharge, pain, and retraction of the nipple. There was no history of any lesion over the other breast or any other body site. Neither she took any hormonal treatment nor did she get pregnant.
On examination, the left breast showed hyperpigmented, warty papules with a growth of the size of 6 cm across, involving the nipple and areola [Figure 1]. There was no tenderness or discharge. There was no lymphadenopathy. No associated anomaly of the nipple or breast was seen. The skin biopsy of the representative lesion showed orthokeratotic hyperkeratosis, slight acanthosis, and papillomatosis changes on routine haematoxylin and eosin-stained specimens [Figure 2]. A breast ultrasound revealed no abnormality of its architecture. Based on the clinical and histopathological features, we reached the diagnosis of nevoid hyperkeratosis of the nipple and areola (NHNA). The patient was subsequently started on topical 0.05% tretinoin cream. No improvement was seen after 3 months of therapy. Therefore, it was decided to undertake radiofrequency ablation because the equipment was available with us and it did not cost anything to the poor patient. After obtaining an informed written consent from the patient, the lesions of the nipple and areola were excised tangentially with a diamond-shaped electrode of a radiofrequency surgical unit under local anaesthesia. Some of the smallest lesions were left behind. She was prescribed antibiotics and analgesics after surgery. The patient has been on follow-up for 7 months post-surgery without any recurrence. The patient is highly satisfied with the cosmetic results. The lesions have healed very well with only some hypopigmentation and scarring [Figure 3].

- Left breast depicting hyperpigmented, warty papules, and growth involving the nipple and areola
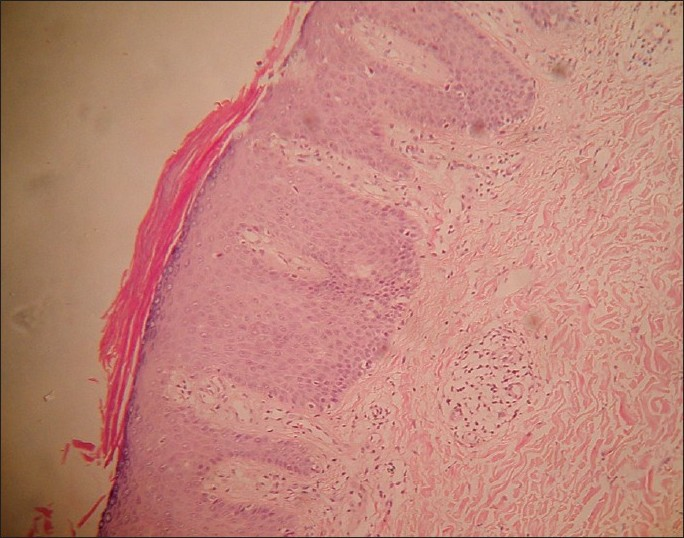
- Section from the representative lesion illustrating orthokeratotic hyperkeratosis, acanthosis, and papillomatosis (H and E, ×40)

- Postradiofrequency surgery follow-up illustrating healed lesions with some residual hypopigmentation and scarring with some smaller residual (left out) lesions in the vicinity
NHNA is a rare, idiopathic disorder, usually seen in females.[12] It presents as hyperkeratotic, verrucous, hyperpigmented papules and plaques of the nipple and areola. They may involve the nipple, areola or both. The lesions are often bilateral but there are reports of unilateral lesions also.[3–6] Unilateral primary hyperkeratosis of the nipple and/or areola must be distinguished from an underlying breast carcinoma.[7] They are generally asymptomatic but may be itchy. Lesions over nipple may cause difficulty in breastfeeding females. The classical Levy-Franckel classification[2] includes three categories, I) As an extension of an epidermal naevus (in which involvement tends to be unilateral and both sexes may be equally affected); II) In association with ichthyosis (in which involvement is bilateral and both sexes may be affected); III) A nevoid type, usually bilateral, and occurring predominantly in women in the second or third decade of life. Considering the above classification, our patient has type III. Alternative classification schemes have been suggested.[8–10] A recommended classification[8] is into (1) primary hyperkeratosis of the nipple and/or areola, which is idiopathic, and (2) secondary hyperkeratosis of the nipple and/or areola, which is associated with epidermal nevus, organoid nevus leiomyomas, verruca, congenital, acquired, or erythrodermic ichthyosis, malignant acanthosis nigricans, Darier disease, chronic eczema such as atopic dermatitis, cutaneous T-cell lymphoma, chronic mucocutaneous candidiasis, pregnant females, males receiving hormonal therapy for prostate cancer, and estrogen therapy for androgen insensitivity syndrome. The etiology of NHNA is still unknown. A change in estrogen milieu has been proposed as a possible mechanism.[10] Histopathologically, it shows hyperkeratosis, filiform acanthosis and papillomatosis, and keratin plugging. NHNA needs to be differentiated from epidermal naevus, acanthosis nigricans, chronic eczema, atopic eczema, seborrhoic keratosis, Darier's disease, Paget's disease, basal cell carcinoma, dermatophytosis and Bowen's disease. The main cause for concern in patients of NHNA is cosmetic appearance of nipple and areola. There is no definitive treatment, yet various treatment modalities have been advocated including topical retinoic acid, topical calcipotriol, low dose acitretin, cryotherapy, carbon dioxide laser, shave excision, and removal of the areola and reconstruction with a skin graft.[11] A case of NHNA was successfully treated with radiofrequency surgery and no recurrence was seen.[12] The current case too was effectively treated with radiofrequency surgery excision with a good cosmetic outcome. No recurrence has occurred so far, 7 months post-surgery.
REFERENCES
- Nevoid hyperkeratosis of the nipple and areola: A distinct entity. J Am Acad Dermatol. 2002;46:414-8.
- [Google Scholar]
- Unilateral nevoid hyperkeratosis of the nipple and areola. Int J Dermatol. 1996;35:602-3.
- [Google Scholar]
- Hyperkeratosis of the nipple and areola as a sign of malignant acanthosis nigricans. Clin Exp Dermatol. 2005;30:721-2.
- [Google Scholar]
- Unilateral hyperkeratosis of the nipple: The response to cryotherapy. Arch Dermatol. 1986;122:1360-1.
- [Google Scholar]
- Unilateral nevoid hyperkeratosis of the nipple: A report of two cases. Indian J Dermatol Venereol Leprol. 2006;72:303-5.
- [Google Scholar]
- Naevoid hyperkeratosis of the nipple and areola. J Eur Acad Dermatol Venereol. 2003;17:232-3.
- [Google Scholar]
- Hyperkeratosis of the nipple and areola: Report of 3 cases. Arch Dermatol. 2001;137:1327-8.
- [Google Scholar]
- Nevoid hyperkeratosis of nipple: Nevoid or hormonal? Indian J Dermatol Venereol Leprol. 2006;72:384-6.
- [Google Scholar]
- Hyperkeratosis of the nipple and areola: 2 years of remission with low-dose acitretin and topical calcipotriol therapy. J Dermatolog Treat. 2008;19:337-40.
- [Google Scholar]
- Treatment of nevoid hyperkeratosis of the nipple and areola using a radiofrequency surgical unit. Dermatol Surg. 2005;31:703-5.
- [Google Scholar]




