
Translate this page into:
Giant Earlobe Epidermoid Cyst
Address for correspondence: Mr. Joaquín Pérez-Guisado, Service of Plastic, Aesthetic and Reconstructive Surgery, Reina Sofía University Hospital, Av. Menéndez Pidal s/n 14004, Córdoba, Spain. E-mail: pv1peguj@uco.es
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Epidermoid cysts represent the most common cutaneous cysts. They are usually small and benign; however, sometimes they can grow to giant epidermoid cists, and occasionally malignancies develop. Giant epidermoid cysts at the earlobe have never been described but in other locations. We describe a case of a giant epidermoid cyst at the earlobe, a location where such a large cyst has never been reported before. The mass was completely resected and the wound of the pedunculated base was sutured with four stitches of nylon 5/0. Histopathology confirmed the presumptive diagnosis of an epidermoid cyst. Six months after the resection, the patient did not have any relapse of the epidermoid cyst. The earlobe is a potential location for giant epidermoid cysts. Although the clinical diagnosis could be enough, due to the possibility of malignancy and to ensure appropriate diagnosis, we consider that all cysts should be sent to the anatomic pathology laboratory for histological evaluation.
Keywords
Epidermal cysts
epidermal inclusion cysts
follicular infundibular cysts
sebaceous cyst

INTRODUCTION
Epidermoid cysts represent the most common cutaneous cysts. Their histogenesis is still unclear although they are probably formed by several mechanisms, including remnant ectodermal tissue that migrates incorrectly during embryogenesis, occlusion of the pilosebaceous unit or traumatic or surgical implantation of epithelial elements.[1] While they may occur anywhere on the body, the most frequently affected areas are the face, scalp, neck and trunk.[2] Giant epidermoid cysts have been described before; nevertheless, our literature search through the most important online databases in English and Spanish language (Google Scholar, OpenJGate, Tripdatabase, PubMed, Clinical Evidence, Cochrane, Scopus, Embase, Biomed Central, Science Direct, Ovid, Willey–Blackwell, Doaj, Doyma, Imbiomed, Scielo and Medigraphic) did not find any report of a giant epidermoid cyst on the earlobe. We describe a case of a male patient with a pedunculated giant epidermoid cyst at the back of the right earlobe. The histology confirmed the diagnosis.
CASE REPORT
The patient was a 76-year-old man who visited our clinic with a tumour at the back of the right earlobe that had appeared 30 years ago as a small lesion of the size of a rice grain and started enlarging slowly.
Two weeks before visiting our clinic, the patient consulted his general practitioner who established a presumptive diagnosis of a giant epidermoid cyst and referred him to our plastic surgery clinic for presurgical evaluation. Physical examination revealed a pedunculated mass 7.5 × 6 cm size with a 2-cm pedunculated base hanging from the posterior side of the right earlobe [Figure 1a]. On inspection, it did not seem to be inflamed or infected. It was not painful and the patient had never received any treatment for it. Fine-needle aspiration was used and the material was sent to the anatomic pathological laboratory. Smears of the aspirated material stained with the Wright–Giemsa stain demonstrated nucleated keratinocytes and a wavy keratin material.
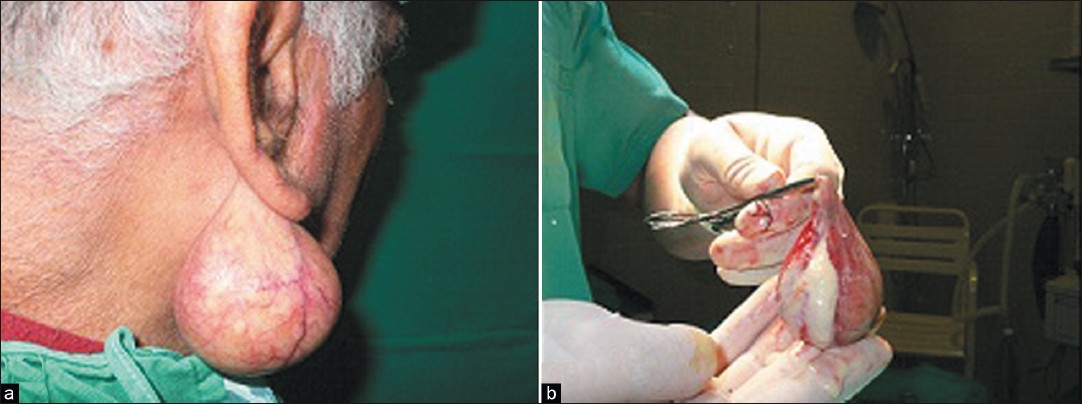
- (a) Giant earlobe epidermoid cyst. (b) Giant epidermoid cyst resection and content
The medical history of the patient included active smoking for 60 years and hypertension for 25 years treated actually with two pills daily of enalapril–hydrochlorothiazide (20/12.5 mg per pill). He was widowed for 19 years; he had been depressed since the death of his wife with partial social isolation and without going to the psychiatrist or having any antidepressant medication.
The patient was treated surgically 9 weeks later: A circumferential incision was made around the pedunculated base of the mass. The mass was completely resected and the wound of the pedunculated base was sutured with four stitches of nylon 5/0. The cyst contained a soft cheesy material [Figure 1b] with a characteristic ‘cheesy’ or ‘foot odour’ smell, and was sent to the anatomic pathology laboratory. Histopathology confirmed the presumptive diagnosis of an epidermoid cyst: A cyst filled with keratin, with epidermal lining and granular layer, and no skin adnexa.
DISCUSSION
Epidermoid cysts are not usually symptomatic; nevertheless, they may become inflamed or secondarily infected, resulting in swelling and redness. Occasionally, malignancies, including epidermoid cell carcinoma as the most common, basal cell carcinoma, mycosis fungoides, Bowen's disease and melanoma in situ, have developed in epidermoid cysts.[3] For that reason, although the clinical diagnosis could be enough, due to the rare occurrence of malignancy and to ensure appropriate diagnosis, we consider sending all cysts to the anatomic pathology laboratory for histological evaluation, specially, if the epidermoid cysts have a long evolution period and large size, like the one in our patient.
The most common locations of epidermoid cysts are the face followed by the trunk and the neck, in that order. However, strange cases of epidermoid cysts occurring in bone, breast and various intracranial locations have been reported.[4] Our experience with epidermoid cysts says that the posterior side of the earlobe is a frequent location; nevertheless, a giant epidermoid cyst like this one has never been reported in such location but some other locations like pre-esternal,[56] presacral,[7] gluteal,[8] intertesticular regions[9] and foot.[10] While a normal patient worried about the aesthetic will go to the doctors or the specialist when he feels the mass is increasing in size, this patient due to his depression and social isolation was not worried about the aesthetic at all and allowed the cyst to grow up during 30 years. If we consider the distal location of the mass, the gravity effect on it could explain its huge size.
Six months after the resection, the patient did not have any recurrence.
Source of Support: Nil,
Conflict of Interest: None declared.
REFERENCES
- MRI findings of subcutaneous epidermal cysts: Emphasis on the presence of rupture. Am J Roentgenol. 2006;186:961-6.
- [Google Scholar]
- Aspiration cytology of epidermoid cyst of terminal phalanx. Diagn Cytopathol. 2002;26:266-7.
- [Google Scholar]
- Melanoma in situ involving an epidermal inclusion (infundibular) cyst. Am J Dermatopathol. 2007;29:564-5.
- [Google Scholar]
- Popliteal epidermoid cyst: An unusual location. Plast Reconstr Surg. 2004;114:830-1.
- [Google Scholar]
- Giant epidermoid cyst in the sternum region. Thorac Cardiovasc Surg. 2008;56:243-5.
- [Google Scholar]
- Giant epidermoid presacral and rectrorectal cyst: Case report. Cir Cir. 2009;77:69-72.
- [Google Scholar]
- Giant epidermal cyst extending from sole to dorsum of the foot by penetrating the interosseous muscles. J Dermatol. 2008;35:25-8.
- [Google Scholar]




