
Translate this page into:
Rare Case of Giant Plunging Ranula without Intraoral Component Presenting as a Subcutaneous Swelling in the Neck: A Diagnostic Dilemma
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 21-year-old male presented with an asymptomatic swelling in the left submandibular region of 1 year duration which was gradually increasing in size. The patient gave history of being operated 45 days back for the same swelling; however, the procedure was abandoned without excision. Subsequently, the patient developed pain in the submandibular region and hence visited our center for definitive management. On examination, an irregular, soft, mildly tender swelling was seen in the left submandibular region measuring 6 × 5 × 3 cm [Figure 1a]. Overlying skin which was otherwise unremarkable showed a scar of previous surgical intervention [Figure 1b]. On oral examination, no swelling was found in the sublingual regions bilaterally. Ultrasonography of the lesion showed an anechoic fluid collection in the submandibular region. Contrast-enhanced STIR and T2-weighted MRI images showed a hyperintense (hypointense on T1W images) cystic lesion in the submandibular region in the subcutaneous plane measuring 4.8 × 3.9 × 3.7 cm [Figure 2]. The swelling was abutting left masseter and medial pterygoid muscles and the left submandibular gland was aseptate and showed no communication with sublingual space. With a preoperative diagnosis of lymphangioma, the swelling was excised under general anesthesia after a course of antibiotics. A horizontal incision of about 8 cm was made in the left submandibular region and the swelling was found to be extending inferiorly into the mid-cervical region, laterally up to angle of mandible and superiorly into the floor of mouth [Figure 1c]. Its superior margin was going behind the inferior border of the mandible into the floor of mouth. All the margins were freed and the excised swelling was sent for histopathology examination. We received a specimen of the cyst containing gelatinous material measuring 5 × 3.5 × 2.5 cm. Microscopic examination revealed a typical extravasation mucocele filled with mucin containing numerous macrophages and no lining epithelium [Figure 3]. The wall focally also contained lymphoid follicles and mucus-secreting salivary glands. During the follow-up period of 6 months, the patient had no recurrence.
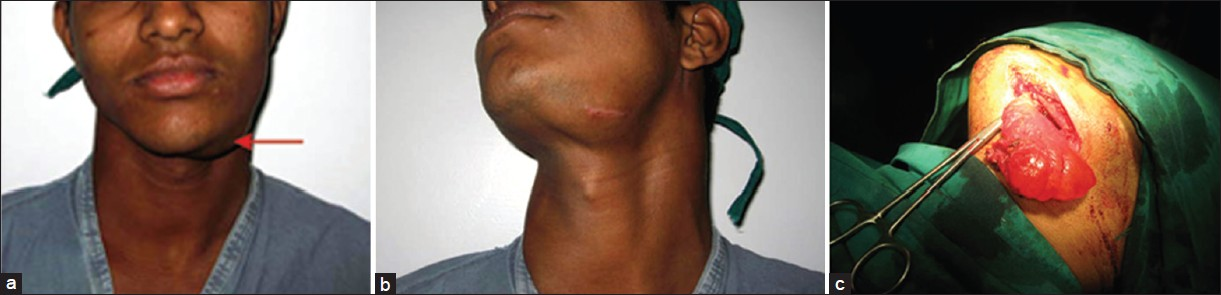
- (a) Photomicrograph showing an irregular subcutaneous swelling in the left submandibular region measuring 6 × 5 × 3 cm with ill-defined margins. (b) Overlying skin was normal in color and temperature; however, a scar of previous surgical intervention was noted over the swelling. (c) Intraoperative photograph of the patient showing swelling with well-defined margins and extending inferiorly into the mid-cervical region, laterally up to angle of mandible and superiorly into the floor of mouth.
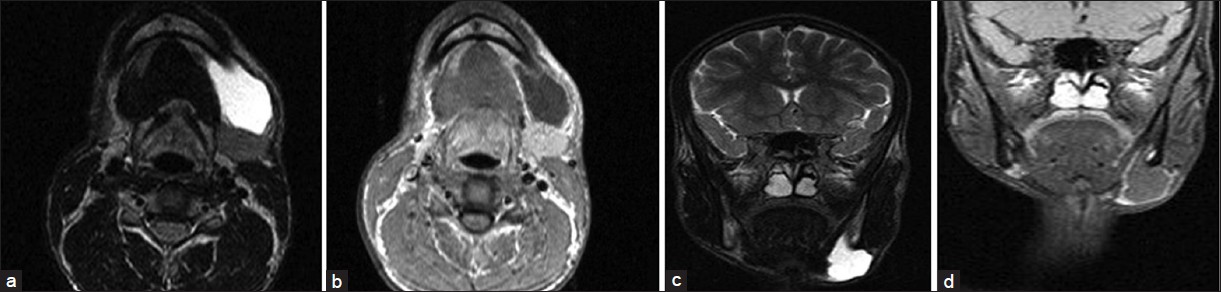
- (A) Contrast enhanced STIR and T-2 weighted MRI axial image showing a hyperintense enhancing cystic lesion in the submandibular region in the subcutaneous plane measuring 4.8 × 3.9 × 3.7 cm. (B) Post-contrast T1W axial image showing hypointense swelling with peripheral rim enhancement suggesting inflammation. (C) Contrast-enhanced STIR and T2-weighted MRI coronal image showing a hyperintense enhancing cystic lesion in the submandibular region. (D) Post-contrast T1W coronal image showing hypointense swelling with peripheral rim enhancement.
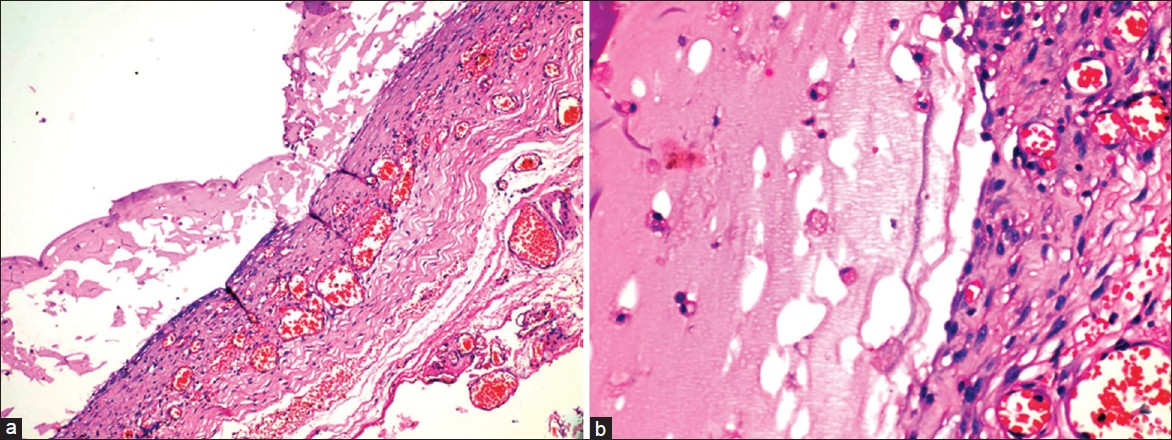
- (A) Photomicrograph showing a low power view of the cyst wall lined by granulation tissue and filled with mucin (Hand E 100×). (B) Higher power of the cyst wall highlighting the absence of lining epithelium and the presence of muciphages (Hand E 400×).
The word “ranula” is derived from a Latin word “rana” meaning “frog” and is a simple, unilocular, extravasation mucocele developing in the floor of the mouth in relation to sublingual glands with a prevalence of 0.2 per 1000 persons.[1] These swellings arise by extravasation of mucus from the sublingual gland secondary to trauma/inflammation although congenital predisposition has been suggested as their prevalence is increased in certain populations like Maori and pacific island polyasians.[1–3] “Plunging” or “diving” ranula is a variant of ranula which is located beyond the mylohyoid muscle and present with painless subcutaneous anterolateral neck masses with most of them having an intraoral component (so-called sublingual-PR).[12] However, rarely these pseudocysts present as subcutaneous cervical masses without any sublingual swelling and hence pose a clinical and radiological dilemma with other cystic swellings of the neck like lymphangioma, epidermoid cyst, dermoid cyst, thyroglossal cyst, branchial cleft cyst, and even mediastinal cysts entering the differential diagnosis depending on the location in the neck.[1] Although the exact prevalence of plunging ranulas without intraoral component is unknown, they are thought to be significantly lower than sublingual/sublingual-plunging ranulas.[34] Ultrasonography is of limited value in evaluation of these swellings but cross-sectional imaging modalities like MRI are helpful.[4] The findings include a unilocular large water density mass with a smooth capsule; lack of internal septations; location extrinsic to the submandibular gland and a characteristic “tail-sign” where sublingual component, if present, communicates with submandibular component of PR through a narrow “tail”.[3] The key differential is a lymphangioma/cystic hygroma which has more infiltrative nature and indistinct margins and has internal lobulation and septations.[3] Enhancement of capsule denotes secondary infection as was observed in our case. Other differentials are rarely a problem clinically and are at best discernible radiologically. Several surgical and non-surgical techniques for treatment of PR have been described with varying success rates including excision of ranula alone or with excision of associated salivary gland; cryosurgery; marsupalization with or without cauterization; incision and drainage; excision of the sublingual gland with drainage of the cyst; CO2 laser; low dose radiation and recently described intracystic injection of streptococcal preparation, OK432.[15] Correct preoperative differentiation from cystic hygroma is essential as the operative approach in both these conditions is different. Whereas cystic hygroma/lymphangioma requires extensive removal of the lesion from the deep spaces of neck, for PR such extensive dissection is not required.[4] However, in the case of PR, removal of sublingual gland is important for prevention of recurrence.[4] In our case, since, intraoperatively, the floor of mouth was adequately explored and on histopathology we found mucinous salivary gland in the wall of the cyst, no further exploration was done. To conclude, PR especially at subcutaneous location without intraoral component can mimic other lesions on clinical and radiological evaluation and hence a preoperative alertness to this lesion is important in evaluation of subcutaneous anterolateral neck masses.
REFERENCES
- Sublingual-plunging ranula as a complication of supraomohyoid neck dissection. Int J Surg Case Rep. 2011;2:90-2.
- [Google Scholar]
- Giant ranula of the neck: Differentiation from cystic hygroma. Am J Neuroradiol. 2003;24:757-61.
- [Google Scholar]
- OK-432 sclerotherapy of plunging ranula in 21 patients: It can be a substitute for surgery. Am J Neuroradiol. 2006;27:1090-5.
- [Google Scholar]




