
Translate this page into:
Dracunculiasis: Two Cases with Rare Presentations
Address for correspondence: Dr. Anirudha Gulanikar, 28, Pannalal Nagar c/o Koppalkar, Aurangabad-431 003, Maharashtra, India. E-mail: agulanikar@hotmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Dracunculiasis (Guinea worm Disease) is a debilitating disease caused by parasite Dracunculus medinensis. The condition is not life threatening, but causes significant morbidity. Patients may be sick for several months. Dracunculiasis has been claimed to be eradicated in India since 1999. We report two patients with calcified guinea worm. Both patient required surgical removal of calcified worm. The cases document that the parasite can cause chronic recurrent nodules and ulcers.
Keywords
Dracunculiasis
gunieworm disease
chronic ulcer

INTRODUCTION
Guinea worm disease (GWD) also known as Dracunculiasis, is a preventable waterborne parasitic disease affecting rural parts of developing nations of South Asia and Africa which do not have access to safe drinking water. It is thought to have existed in India for several thousand years. Banwari Lal, a 25-year-old man from the Jodhpur district in Rajasthan, was India's last reported case of guinea worm disease in July 1996. However, subsequently three more cases were reported from parts of Rajasthan.[1] Today, GWD is seen only in some communities in remote parts of Africa. Annual number of reported cases worldwide has been declined from approximately 900,000 in 1989 to only about 3000 in the year 2009 and about 1000 in the year 2011.[2–4] Asia is considered as free of disease. The disease is not fatal, but causes considerable disability. There is pain and difficulty in moving because of complications of the disease.
CASE REPORTS
Case 1
An 8-year-old girl from rural area came with chief complaints of pain in left leg and ulcer on left shin of 15 days duration. These symptoms were recurrent for last 4 years. The ulcer used to heal with antibiotics and recur after few days. Biopsy done from the ulcer by the treating doctor showed only chronic inflammatory infiltrate. There was no evidence of osteomyelitis on X-ray. She was given anti-tubercular therapy and then multidrug therapy (MDT) for leprosy but the ulcer recurred.
On examination, there was an ulcer of size 3 × 3 cm on shin anterior aspect and a healed ulcer just above the present ulcer. Sensation was normal. There were no thickened nerves or lymphadenopathy. Her general and systemic examination and laboratory investigations were within normal limits. A X-ray of left leg showed no evidence of osteomyelitis however, it revealed a linear calcification ending in the ulcer. Previous X-ray also showed the same linear calcification [Figure 1]. A provisional diagnosis of GWD was made, on the basis or radiological features long linear chain mail type of calcification typical of calcified Gunieworm. As the lesion was chronic and recurrent, we decided to surgically remove the worm. When it was opened, a long linear calcified worm was found which was removed from the subcutaneous plain [Figures 2–4]. Skin was sutured in layers [Figure 5]. Wound healed completely and there was no recurrence thereafter. We followed the case for 3 years and there were no complaints.
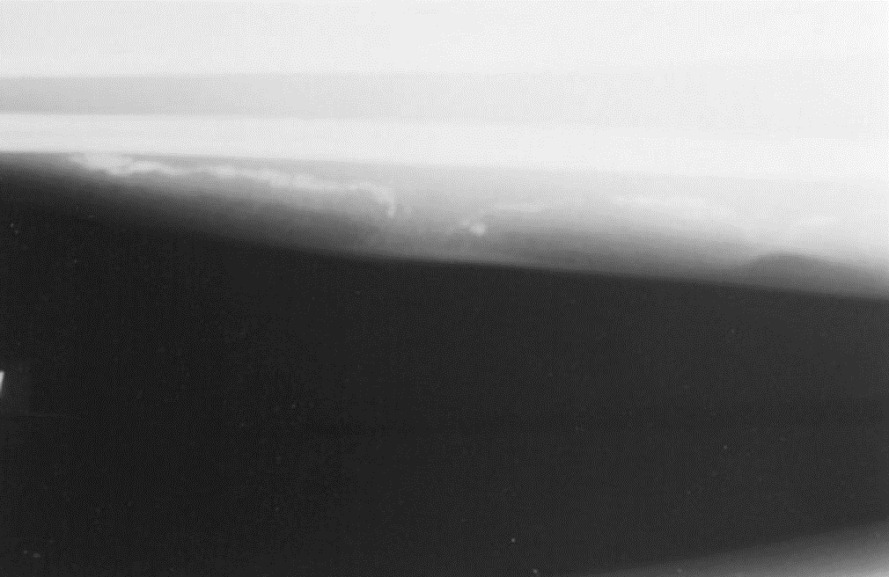
- X-ray showing linear calcification
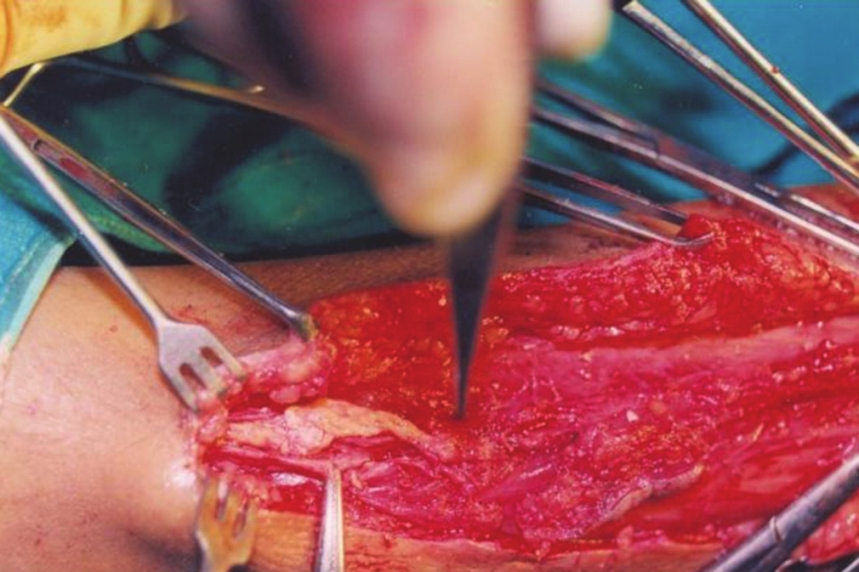
- Intra operative demonstration of worm
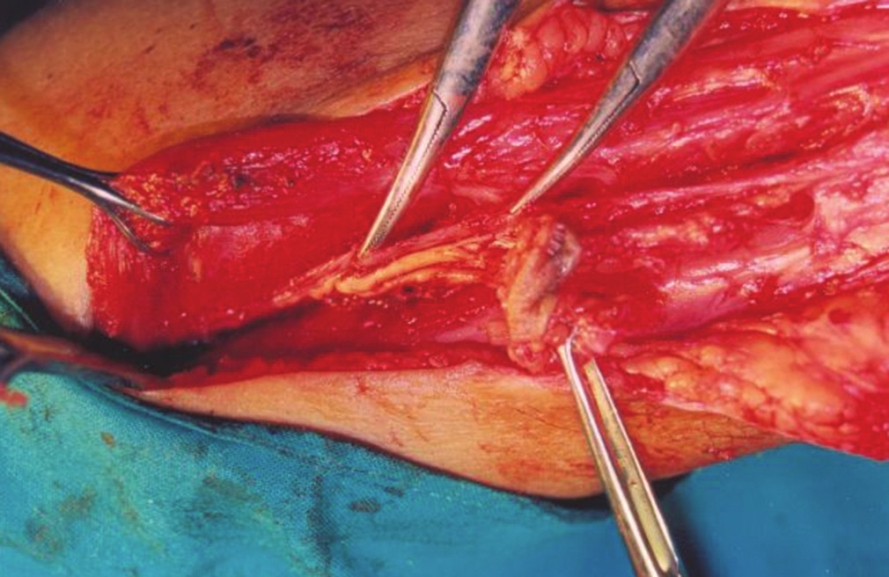
- Intra operative demonstration of worm

- Wound closure

- After suture removal

- Case 2 clinical presentation
Case 2
A 25 year old woman came with complaints of nodular lesion left side abdomen for 5 to 7 years [Figure 6]. It was associated with pain and discharge for 3-4 days.
Lesion was slowly progressive. She had not taken any treatment for this.
Dermatological examination showed large nodular lesion of size 5 cm in diameter left side abdomen, not adherent to the deeper structures. We decided to rule out Squamous cell carcinoma (SCC) and a biopsy was done. It showed calcified lesion with no evidence of malignancy.
Lesion was excised and the whole specimen was again sent for histopathology which showed calcified worm.
DISCUSSION
Dracunculiasis is considered as eradicated from India. The cases presented here are rare and were difficult to diagnose and physcians may not have seen such case for many years.
Dracunculiasis (GWD) is a parasitic disease caused by the parasite worm Dracunculus medinensis commonly known as guinea worm.
The mode of transmission is by drinking stagnant water containing copepods that carry Gunieworm Larvae. Person is infected with Guinea worm by drinking such stagnant water. Guinea worm larvae are eaten by the copepods that live in these stagnant water sources. The larvae mature in 2 weeks in the copepods before they can infest humans.
After ingestion, the copepods die and release the larvae, which penetrate the host stomach and intestinal wall and enter the abdominal cavity and retroperitoneal space. After maturation into adults and copulation, the male worms die and the females migrate in the subcutaneous tissues towards the skin surface. They are 70 to 120 cm long. About a year after infection, the female worm induces a blister on the skin, generally on the distal lower extremity, which ruptures when it comes into contact with water, a contact that the patient seeks to relieve the local discomfort. The female worm emerges and releases larvae into water. The larvae are ingested by a copepod, which completes the life-cycle.
The clinical features include slight fever, itchy rash, nausea, vomiting, diarrhoea, and dizziness. A blister develops most commonly on lower extremity. It enlarges and cause severe pain and burning sensation, which relieves on submerging the part in water. Acute stage complications include cellulitis, abscesses, septic shock, septic arthritis, while in late stage calcification of worm and joint deformities can occur. Acute stage is treated with local care of ulcer, combined with slowly removal of the worm. Systemic antibiotics are given to prevent secondary infection. In chronic stage, rarely the calcified worm may cause recurrent problems as in our case and need surgical removal.
The radiological diagnosis can be made easily when the characteristic long linear, serpiginous or coiled, whorled “chain mail” types of calcification are present in the soft tissues.[4–6] Several filarial worms, particularly Loa loa and Onchocerca volvulus, may calcify but these are much smaller and almost always seen in the hands and feet. Either may cause small, coiled masses of calcification and occasionally may be linear, but neither is as large or extensive as the guinea worm.
In summary, although considered eradicated long ago, occasional cases of calcified guinea worm can occur. Physicians should be aware of this rare diagnosis and should have high index of suspicion for early diagnosis and treatment. The calcified worm, if it causes recurrent problems, should be removed surgically.
Source of Support: Nil.
Conflict of Interest: Nil.
REFERENCES
- Dracunculiasis in tribal region of southern Rajasthan, India: A case report. J Parasit Dis. 2010;34:94-6.
- [Google Scholar]
- Anonymous. Dracunculiasis eradication-Global surveillance summary 2009. Wkly Epidemiol Rec. 2010;85:166-76.
- [Google Scholar]
- Anonymous. Monthly report on dracunculiasis cases, January-November 2011. Wkly Epidemiol Rec. 2012;87:59.
- [Google Scholar]
- Text book of parasitology (13th ed). Kolkotta: CBS Publishers; 2011. p. :254-8.
- Serpentine calcification: A radiological stigma. J Neurosci Rural Pract. 2011;2:203-4.
- [Google Scholar]




