
Translate this page into:
Body Hair Transplantation in Vitiligo
Address for correspondence: Dr. Kavish Chouhan, DERMACLINIX-The Complete Skin and Hair Solution Center, D-9, GF, Green Park Main, Delhi - 110 016, India. E-mail: kavish_chouhan@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Hair transplantation has been used to repigment a stable vitiligo patch. Body hair transplant was done for a 28-year-old male with stable vitiligo with scarring. Peri-folllicular repigmentation was noted at 4 weeks and complete repigmentation of vitiligo patch was achieved at 12 weeks. No recurrence was noted at the end of 3-month follow-up with a good colour match with surrounding skin. To the best of our knowledge, this is the first case report highlighting the effectiveness of body hair transplantation by FUE in focal vitiligo patch with leukotrichia.
Keywords
Body hair transplant
follicular unit extraction
leukotrichia
stable vitiligo

INTRODUCTION
Stable vitiligo has been treated with various surgical modalities including hair transplantation at vitiligo patch with variable success rates. Scarring in vitiligo patch results in loss of hairs and, thereby it is difficult to achieve good repigmentation in these cases. Body hair transplantation (BHT) helps in repigmentation by perifollicular spread of melanocyte and stem cells from the implanted follicles. In addition, the aesthetic appearance is also restored by the new hair. This method is effective in focal vitiligo, vitiligo in non-glabrous areas, and in those patches with leukotrichia.
CASE REPORT
A 28-year-old male presented with multiple focal depigmented macules varying from 1 × 1 to 4 × 6 cm in size on the left shin, calves and both ankles [Figure 1] since past 2 years. Leukotrichia was present. He had applied some Ayurvedic preparation (content not known), which led to phototoxicity resulting in focal scarring on shin. No new lesions were seen elsewhere in the body and the size of the lesions had remained stable for the past 1 years. No history of Koebner’s phenomenon was noted. A diagnosis of vitiligo was made based on the clinical findings. The patient was first started on phototherapy with good improvement, but the areas of scarring [Figure 2a] were not improving despite treatment for 6 months. Body hair transplant was suggested in the areas of scarring. Informed consent was taken. Donor hairs were harvested under aseptic conditions from the right upper thigh by follicular unit extraction (FUE) method [Figure 3] using 0.8-mm punch under local anaesthesia. A total of 52 intact follicular units were extracted. Follicular units were simultaneously transplanted in directions of existing hairs [Figure 2b] using 19-g needle in the depigmented macules with 5-mm gap between the follicles. After implantation, the hair density was roughly 6-8 FU/cm2. Phototherapy was restarted in the recipient area after 1 week of the procedure. Perifollicular repigmentation in the vitiligo patch was seen at the end of weeks by the patient [Figure 2c], and complete pigmentation was achieved at 12 weeks with partial reversal of leukotrichia [Figure 4]. Colour matching was good, but superficial atrophy was still left because of previous scarring. There was no recurrence after 3 months of follow-up.

- Baseline photograph before starting medical treatment
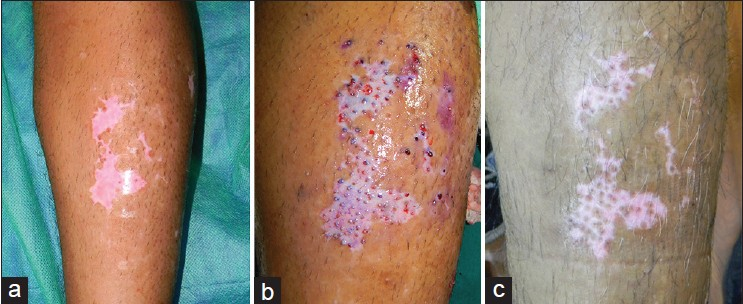
- (a) Vitiligo patch with scarring before surgery (after medical treatment)

- Follicular unit extraction from thigh

- The 3-month result with 100% pigmentation, but with evidence of previous scar and slight hyperpigmentation
DISCUSSION
Follicular unit transplant (FUT) was introduced to repigment vitiligo patches in 1998.[1] Ortonne et al., proposed that repigmentation of vitiligo was derived from the melanocyte reservoir in the hair follicles.[2]
After FUT, the diameter of pigment spread is 5–12 mm per hair grafted.[3] Pigmentation starts appearing at 4–5 week and continues up to 6 months or even longer.[3] Transformation of depigmented hairs into pigmented hairs has been reported following FUT, as seen in our case also.[1] Non-cultured extracted hair follicular outer root sheath (ORS) cell suspension transplantation has also been tried with 65.7% repigmentation.[4] BHT by FUE circumvents the need of tedious melanocyte suspension process.
As hair follicle melanocytes are more resistant to the vitiligo process,[1] hair restoration in a vitiligo patch may be a good modality in non-glabrous area. BHT by FUE in vitiligo is less invasive and leaves almost no visible scarring in donor area. Moreover, the extracted follicular units are directly ready for implantation and give good aesthetic outcome as the hairs matches with the surrounding hairs. In comparison to scalp hair, body hair does not require frequent trimming. However, this method has some limitation; BHT by FUE is a time-consuming and delicate procedure requiring lots of expertise.
BHT by FUE appears to be an effective method for treating localized/segmental vitiligo, especially on hairy parts of the skin, including the eyelids and eyebrows and for small areas of vitiligo. As seen in our case, even density of 6-8 FU/cm2 was sufficient to induce complete pigmentation. The best application of this method will be in vitiligo patches with leukotrichia. In cases of focal vitiligo with scarring/loss of hairs, this procedure could be considered as the procedure of choice.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Single hair grafting for the treatment of vitiligo. J Am Acad Dermatol. 1998;38:580-4.
- [Google Scholar]
- PUVA-induced repigmentation of vitiligo: Scanning electron microscopy of hair follicles. J Invest Dermatol. 1980;74:40-2.
- [Google Scholar]
- Transplantation of hair follicles for vitiligo. In: Gupta S, ed. Surgical Management of Vitiligo (1st ed). New Delhi: Wiley India; 2007. p. :122-7.
- [Google Scholar]
- Noncultured extracted hair follicle outer root sheath cell suspension for transplantation in vitiligo. Br J Dermatol. 2011;164:1241-6.
- [Google Scholar]




