
Translate this page into:
Chemical Reconstruction of Skin Scars Therapy Using 100% Trichloroacetic Acid in the Treatment of Atrophic Facial Post Varicella Scars: A Pilot Study
Address for correspondence: Dr. Asit Mittal, House No. 62, Road No. 2, Ashok Nagar, Udaipur, Rajasthan, India. E-mail: asitmittal62@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Chickenpox (varicella) is a common viral disease caused by Varicella zoster virus. Facial atrophic scars after varicella infection are not uncommon and pose a cosmetic problem. Like atrophic scars of other aetiologies, they are a difficult condition to treat. There are not enough references in the literature regarding efficient treatment of post varicella scars. High strength Trichloroacetic acid (TCA), which is known to cause dermal collagen remodelling, was used to treat varicella scars in the present study.
Aims:
The study was undertaken to assess the efficiency of Chemical Reconstruction of Skin Scars (CROSS) technique using 100% TCA in the treatment of atrophic facial post varicella scars. Settings and Design: Open label, pilot study.
Materials and Methods:
A total of 16 patients with atrophic facial post varicella scars were treated by focal application of 100% TCA solution by pressing down upon the scar surface by a toothpick (CROSS technique). Total 4 sittings were given at 2 weekly intervals and the results evaluated after 3 months of follow-up. Statistical analysis was carried out using Fischer's exact t-test.
Results:
All of the 13 patients who completed the study showed good clinical improvement, with 69% patients grading the response as excellent (>75%) improvement, whereas the rest 31% patients reporting good (51-75%) improvement. No significant complications were seen in any patient.
Conclusions:
CROSS technique using 100% TCA is a safe, cheap and effective therapy for the treatment of post varicella scars.
Keywords
Chemical reconstruction of skin scars
scar
trichloroacetic acid
varicella

INTRODUCTION
Chickenpox (varicella) is a common viral disease caused by Varicella zoster virus. It is a self-limited disease with few complications and sequelae. Post-inflammatory scarring of isolated lesions may occur.[1] These scars are generally atrophic and may be associated with other complications such as hyperpigmentation and hypopigmentation.[23] Patients with facial scars suffer from considerable mental and emotional trauma, impairment of social life and deterioration of life quality. Like atrophic scars of other aetiologies, they are a difficult condition to treat. There are not enough references in the literature regarding efficient treatment of post varicella scars.
Trichloroacetic acid (TCA) is an established peeling agent for skin resurfacing. Lee et al. suggested focal application of higher strengths of TCA on atrophic facial scars[4] and termed it Chemical Reconstruction of Skin Scars (CROSS). It resulted in a rapid healing and lower complication rates, due to sparing of adjacent normal tissue and adnexal structures. This prompted us to evaluate the efficacy of CROSS therapy in the treatment of varicella scars.
MATERIALS AND METHODS
The study was undertaken to assess the efficiency of CROSS therapy using 100% TCA in the treatment of atrophic facial post varicella scars.
Adolescents and adults (10-45 years) attending the dermatology outdoor with complaints of atrophic facial varicella scars of more than 3 months duration, were included in the study after informed consent. All the patients had Fitzpatrick III-V photo type. Patients with a prior history of herpes simplex infection, keloidal tendency, systemic complications of varicella such as encephalitis, pneumonia and hepatitis; and those with scars of less than 3 months duration, were excluded from the study. Methodical recording of the number of scars, duration of scars, associated hypopigmentation or hyperpigmentation and patient's previous and current medications was carried out. Pre-treatment photographs of the patient were taken for record and photographic evaluation.
Before the procedure, the patient's face was washed with soap, and cleaning with alcohol was carried out. They were instructed to keep their eyes closed during the procedure and 10 ml syringes filled with normal saline were kept handy for any accidental TCA spills. 100% TCA (w/v) was used in the study, which was prepared by adding distilled water to 100 g of TCA crystals until the volume of solution became 100 ml. TCA was focally applied by stretching the skin and pressing and moving a toothpick dipped in solution on the entire depressed area of scars, taking care not to spill over on the surrounding normal skin.
All the patients were comfortable during the procedure, and no local anaesthesia was needed. Patients experienced burning sensation for duration of 2-3 min. The area was monitored until it reached a frosted appearance. They were advised not to detach the crusts which developed within 24 h after the procedure, which was allowed to fall off naturally over the next 5-7 days. Avoidance of sunlight and application of a topical sunscreen were advised for the entire duration of the study and follow-up. They were instructed to apply 2% hydroquinone cream to the treated areas, once at night, after shedding of the crusts.
The focal TCA application was performed every fortnight for 4 sittings (or less if the lesions healed earlier). The results were analysed 3 months after the last sitting.
The assessment of response was performed at the end of 3 months of follow-up after the last sitting. The primary outcome measure was subjective improvement in the depth of scars as assessed by the patient himself according to the following grading:
-
Poor: 0-25% improvement
-
Fair: 26-50% improvement
-
Good: 51-75% improvement
-
Excellent: >75% improvement.
Secondary outcome measures were satisfaction of the patient with the treatment given (satisfied/dissatisfied), and photographic assessment. Photographs taken before the start of treatment and at the end of follow-up were compared by two independent dermatologists and assessed for improvement in depth of scars (poor, fair, good and excellent), and improvement in hyperpigmentation [Figures 1–4].

- Varicella scars; pre-treatment

- Varicella scars; 3 months post-treatment
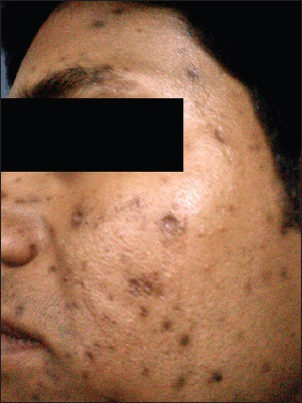
- Varicella scars; pre-treatment

- Varicella scars; 3 months post-treatment
RESULTS
All patients had deep, atrophic, monomorphic, boxcar like scars. A total of 16 patients were included in the study, out of which 3 were lost to follow-up. A total of 13 patients (5 males and 8 females) completed the study. Number of scars ranged from 1 scar in 2 patients to >25 scars in 4 patients. The duration of scars varied from 3 months to 6 years. All the patients had associated hyperpigmentation. None of them was on any other medication.
At the end of study period, 9 patients out of 13 graded the response as excellent (75-100%) improvement while the remaining 4 reported good (50-75%) improvement. Most patients started noticing response after the first sitting itself, which thereafter increased progressively, becoming more apparent after the 3rd and 4th sittings. Two patients reported excellent improvement after 2 sittings; their treatment was discontinued and they were kept under follow-up.
All the patients reported satisfaction with the treatment provided. As per the photographic assessment, 8 patients had an excellent improvement while 5 had good improvement. There was improvement in associated hyperpigmentation in all the cases. None of the patients developed hypopigmentation or keloid. The treated areas had transient erythema in all patients, which faded over 3-8 weeks. The efficacy of therapy was not significantly influenced by the patient's age, skin type, sex or the duration of scar.
DISCUSSION
Atrophic scars are a common complication of varicella infection. They have been reported to occur in up to 18% of patients in various studies.[23] Adults are more prone as they have more and deeper skin lesions.[5] Despite being such a common cosmetic problem, an extensive Medline search for treatment of facial chicken pox scars returned a paucity of studies. Published data of small series of patients treated with Pulsed Erbium YAG laser, high energy short pulsed CO2 laser and continuous wave CO2 laser show variable results.[67]
TCA is an established peeling agent for skin resurfacing. It is usually considered safe when used in low concentrations as a superficial or medium depth chemical peel.[891011] Higher strength TCA (>50%) is not used for peeling, because it causes coagulation necrosis up to reticular dermis, which heals with scarring. However when it is applied focally, only to the already scarred areas, this complication of scarring becomes irrelevant. Subsequently, wound healing by secondary intention leads to deposition of collagen, glycosaminoglycans and elastin fibres in the first few weeks. It results in uplifting the base of scar and recovery of 70-80% tensile strength at the end of 2 months. Thereafter, dermal connective tissue remodelling takes over which may continue for several months.[1213] This process can be considered as creating a less depressed and cosmetically more acceptable scar within the previous scar.
Lee et al. suggested focal application of higher strengths of TCA on atrophic facial scars. This technique of producing focal deep chemical injury by pressing hard on the scar surface was termed as CROSS.[4] It resulted in rapid healing and lower complication rates, due to sparing of adjacent normal tissue and adnexal structures. They reported that 27 of 33 patients (82% of the 65% TCA group) and 30 of 32 patients (94% of the 100% TCA group) experienced a good clinical response. A better and faster response was seen in the 100% TCA group. They also observed that repeated application of high strength TCA is effective in the treatment of deep boxcar scars. In another study, Leheta et al. recommended 100% TCA for use in boxcar scars.[14] The response of scarred tissue to chemical ablation is likely to be governed by scar morphology and the biology of wound healing, irrespective of scar aetiology. The efficacy of TCA CROSS in deep boxcar scars rationalises its use in varicella scars as both are similar in morphology. Two previous studies report the usefulness of this therapy in varicella scars.[1516] Fabbrocini et al. used focal application of 50% TCA application in the treatment of 5 patients with atrophic acne or chicken pox scars.[15] Clinical examination revealed cosmetic improvements in both depth and appearance of skin scars. In a recently published study, Barikbin et al. used 70% TCA at 3 weekly intervals for a maximum of 6 sessions in a series of 100 patients with varicella scars and reported marked improvement in 41%, moderate improvement in 42% and mild improvement in 12% cases at the end of 12 weeks of follow-up.[16] Mild erythema, hyperpigmentation and hypopigmentation were seen in 17%, 15% and 2% patients respectively, which cleared with appropriate symptomatic treatment at 3 months after treatment.
This is probably the first study evaluating CROSS technique using 100% TCA on patients of atrophic facial varicella scars. We believe that higher strength of TCA and more frequent application might be responsible for the better results obtained in our patients. The same was suggested by previous authors including Lee et al. in their original article on CROSS.[417]
The possible adverse effects of this treatment include post inflammatory hyperpigmentation or hypopigmentation, and worsening the scar due to spillage of TCA beyond the scar boundaries accidentally or because of improper technique. Hyperpigmentation may be problematic in the darker skin types, but is usually transient and adequately managed by photo protection, sunscreens and prophylactic/therapeutic use of topical hydroquinone and mild steroids. No significant complications such as persistent erythema or dyspigmentation, hypertrophic scars or keloids have been reported.
There are some obvious drawbacks of our study, such as lack of a control group and small sample size. Larger controlled studies need to be performed to arrive at any conclusion. Furthermore, no objective scoring system was used for evaluation of treatment response. However, we believe that the only indication of treatment of cosmetic complaints such as scars is the demand of the patient. Therefore, the patient's own assessment of improvement, and his/her satisfaction with the treatment given shall be important considerations. These were adequately evaluated in the study.
CONCLUSION
Atrophic varicella scars are a common cosmetic problem, and the therapeutic options have remained unexplored. CROSS therapy using high strength TCA may prove to be an efficient, easy and cheap treatment, with few if any adverse effects. More studies with larger number of patients need to be conducted exploring other treatment options as well as detailing the efficacy of CROSS technique using TCA in various concentrations and frequency of treatment.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Facial scarring after varicella. A comparison with variola major and variola minor. Am J Epidemiol. 1981;114:798-803.
- [Google Scholar]
- Focal treatment of acne scars with trichloroacetic acid: Chemical reconstruction of skin scars method. Dermatol Surg. 2002;28:1017-21.
- [Google Scholar]
- Resurfacing of pitted facial scars with a pulsed Er: YAG laser. Dermatol Surg. 1997;23:880-3.
- [Google Scholar]
- Scar resurfacing with high-energy, short-pulsed and flashscanning carbon dioxide lasers. Dermatol Surg. 1998;24:101-7.
- [Google Scholar]
- Variations and comparisons in medium-depth chemical peeling. J Dermatol Surg Oncol. 1989;15:953-63.
- [Google Scholar]
- A comparative histologic study of the effects of three peeling agents and dermabrasion on normal and sundamaged skin. Aesthetic Plast Surg. 1982;6:123-35.
- [Google Scholar]
- Depths of chemexfoliation induced by various concentrations and application techniques of trichloroacetic acid in a porcine model. J Dermatol Surg Oncol. 1989;15:967-71.
- [Google Scholar]
- Quantitative and qualitative effects of chemical peeling on photo-aged skin: An experimental study. Plast Reconstr Surg. 2001;107:222-8.
- [Google Scholar]
- Tissue renewal, regeneration, and repair. In: Kumar V, Abbas AK, Fausto N, Aster JC, eds. Robbins and Cotran pathologic basis of disease (8th ed). Philadelphia: Elsevier; 2010. p. :79-110.
- [Google Scholar]
- Histologic study of depressed acne scars treated with serial high-concentration (95%) trichloroacetic acid. Dermatol Surg. 2006;32:985-90.
- [Google Scholar]
- Percutaneous collagen induction versus full-concentration trichloroacetic acid in the treatment of atrophic acne scars. Dermatol Surg. 2011;37:207-16.
- [Google Scholar]
- CROSS technique: Chemical reconstruction of skin scars method. Dermatol Ther. 2008;21:S29-32.
- [Google Scholar]
- Focal high-concentration trichloroacetic acid peeling for treatment of atrophic facial chickenpox scar: An open-label study. Dermatol Surg. 2012;38:1662-7.
- [Google Scholar]
- An assessment of the efficacy and safety of CROSS technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3:93-6.
- [Google Scholar]




