
Translate this page into:
Fatal Necrotising Fasciitis After Spinal Anaesthesia
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Necrotising fasciitis (NF), also known as necrotising soft-tissue infections is a progressive, lethal and often polymicrobial bacterial infection of the fascia and surrounding soft-tissue. High index of suspicion is vital in early diagnosis and treatment, as poor prognosis is associated with late diagnosis and treatment. We present a rare case of NF as a result of Escherichia coli complicating spinal anaesthesia.
A 27-year-old female patient was admitted in the emergency department of LLRH, Kanpur with severe pain, swelling, erythema and blackening involving nearly whole of the back of the trunk, part of anterior abdominal wall and the gluteal regions accompanied by fever and chills. Patient had a history of cesarean section delivery 20 days back for which spinal anaesthesia was given. After 2 days, patient developed severe pain, redness and swelling at the injection site in the lumbar region, rapidly progressing to swelling and skin discoloration of the whole of the back, part of gluteal regions and anterior abdomen starting from the spinal injection site. On examination, the patient's general condition was very poor with temperature 40°C, pulse rate 130/min, blood pressure 84/52 mm Hg and respiratory rate 24/min. There was extensive deep NF of the whole of back and part of anterior abdomen and gluteal regions with gangrene and foul smelling exudates [Figure 1]. Early goal directed therapy for septic shock initiated immediately. Fluid resuscitation started with crystalloids and colloids. Blood cultures were sent. Foley's catheterisation done and intravenous ceftriaxone and clindamycin were administered. Central venous pressure was measured and found to be 9 cm H2O. Patient remained hypotensive, tachycardia and oliguric. Injection noradrenaline (2 mg/kg/min) and injection dopamine (16 mg/kg/min) started and the mean arterial pressure slowly raised to above 65 mm Hg. Laboratory findings showed total leucocyte count of 24,000/mm3 with increased polymorphs, haemoglobin of 6.7 g/dl, serum creatinine 3.2 mg/dl, blood urea nitrogen 98 mg/dl with hyponatremia, hypocalcemia and hyperkalemia. Arterial blood gas analysis revealed metabolic acidosis. Other laboratory results were normal. Electrocardiogram showed sinus tachycardia at a rate of 120 beats/min. Chest radiograph was normal. Patient shifted to operation theatre and surgical debridement of the devitalised tissues was done. The operative findings revealed diffuse necrosis of the skin, fascia and the muscles. Wound swab culture and tissue biopsy was sent. After 12h, patient became drowsy, hypotensive, anuric and tachypneic with Glasgow Coma Scale of 7/15. Tracheal intubation done and patient kept on mechanical ventilation in the intensive care unit (ICU). However despite all aggressive medical and surgical interventions, the patient died on the 3rd day of admission in the ICU due to sepsis induced multiorgan failure. Blood and swab culture report revealed luxuriant growth of E. coli. Histopathological examination confirmed the diagnosis of NF with myonecrosis [Figure 2].

- Extensive deep necrotising fasciitis of the whole of back and part of anterior abdomen and gluteal regions with gangrene and foul smelling exudates
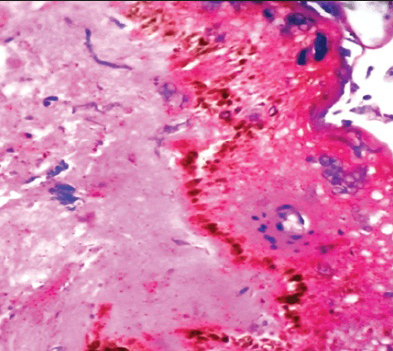
- Histopathological section showing epidermis and dermis with ballooning degeneration of the epidermal cells and mild neutrophilic infiltration in the dermis
NF is a rare, potentially fatal bacterial infection characterized by widespread necrosis of the subcutaneous tissue, superficial fascia and skin[1] and is associated with high mortality and long-term morbidity.[2] The risk of infection during regional anaesthesia is considered to be very low, epidural catheter-related infections are the major cause of this problem after neuroaxial block.[3] Laboratory tests, tissue biopsies along with appropriate imaging studies may facilitate the diagnosis of NF.[4] Broad spectrum antibiotics, aggressive exploration and debridement of suspected deep seated infection and supportive measures for the management of septic shock and multiorgan failure can be life-saving.[5] Maintaining strict asepsis during any surgical procedure and regional anaesthesia techniques is vital in preventing the occurrence of the disease.
REFERENCES
- Necrotizing fasciitis: A dramatic surgical emergency. Eur J Emerg Med. 2004;11:44-8.
- [Google Scholar]
- Prognostic factors in necrotizing fasciitis and myositis: Analysis of 16 consecutive cases at a single institution in Switzerland. Ann Plast Surg. 2007;58:523-30.
- [Google Scholar]
- Clinical and bacteriologic survey of epidural analgesia in patients in the intensive care unit. Anesthesiology. 1996;85:988-98.
- [Google Scholar]
- Value of standard laboratory tests for the early recognition of group A beta-hemolytic streptococcal necrotizing fasciitis. Clin Infect Dis. 2001;32:E9-12.
- [Google Scholar]
- Aggressive surgical management of necrotizing fasciitis serves to decrease mortality: A retrospective study. Am Surg. 1998;64:397-400.
- [Google Scholar]




