
Translate this page into:
Railroading Technique of Dermal Grafting for Linear Atrophic Scarring
Address for correspondence: Dr. Sacchidanand S, Department of Dermatology, Venereology and Leprosy, Bangalore Medical College and Research Institute, Bangalore, Karnataka, India. E-mail: sacchi1260@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Dermal grafting is a valuable technique in the field of dermatosurgery for the treatment of atrophic scars where the source of filler material is the patient's own dermis. However, it is underused for the reasons being difficulties in placing the graft in the tunnel, keratin cysts and complications due to biofilms. Railroading technique used in urology for rupture urethra has been described for dermal grafts to overcome the technical difficulties of graft placement.
Keywords
Atrophic scars
dermal graft
railroading

INTRODUCTION
Dermal grafting is the implantation of appropriately dissected deep dermis into corresponding recipient areas like atrophic scars or other soft tissue defects.[1] Dermal grafts, autologous fat and injectable fillers have been used to correct deeper contour defects.[23] The advantages of dermal graft over other techniques are no allergic reactions as it is autologous, readily available, easily contoured to fit the defect and is firm. However, the technique does not improve skin color or texture.
TECHNIQUE
Patient is ideally taken up after subcision[4] done 2 weeks before the dermal grafting. This facilitates in sliding the graft easily into the tunnel created. This technique is ideally suited for linear atrophic scars.
Step 1: Harvesting dermal graft
Retroauricular area [Figure 1] is the ideal donor site for dermal graft since it relatively lacks appendages. The area is motor or manual dermabraded after local anesthesia till bleeding and whitish tissue is visible. Removal of epidermis decreases the risk of keratin cyst in recipient area. The donor graft should be 3-5 mm more than the recipient area dimensions. Superficial fat also can be excised along with the dermal graft if there is more recipient area atrophy. The wound is closed with 4-0 polyglactin 910 using running horizontal mattress suture [Figure 2].

- Donor site: Retroauricular area

- Continuous horizontal mattress suture at the donor area
Step 2: Preparation of dermal graft
The excised graft [Figure 3] is trimmed to the required dimensions and one end is tied with 3-0 polyglactin 910. For easy graft handling, the dermal graft is trypsinised for 45 min and washed with phosphate buffered saline. Trypsinisation softens the dermal graft and helps it to slide easily into the tunnel.[5]

- Excised dermal graft
Step 3: Forming a tunnel
A 16-G needle with syringe attached for grip is inserted through one edge of the scar (recipient area). The sharp bevel of the needle exits from the other end of the scar. The needle is kept in the same position and moved side to side within the confines of the scar creating only one tunnel [Figure 4].

- Forming a tunnel with a 16-G needle
Step 4: Threading suture into needle
The free end of the suture material tied to one end of the dermal graft is threaded into the bevel of the needle till the suture's free end exits through the hub of the needle. Sutured end of the dermal graft is at the level of bevel of the needle [Figure 5].

- Threading the suture into the needle
Step 5: Railroading dermal graft into tunnel
The dermal graft is now railroaded through the tunnel till the other edge of the linear scar [Figure 6] [Video online]. Suture at one edge of the scar is cut and the graft is left in place. As only one tunnel is created, the possibility of graft losing track is less and pre-trypsinisation facilitates easy sliding of the graft in the tunnel. The edges of the scar can be secured with tapes or sutured with 5-0 polypropylene. [Figure 7]. The lift of the atrophic scar along with decrease in shadow effect can be visualized immediately [Figure 8]. The sutures are removed after 5 days.

- Railroading dermal graft into the tunnel

- Securing the edges with non-absorbable suture
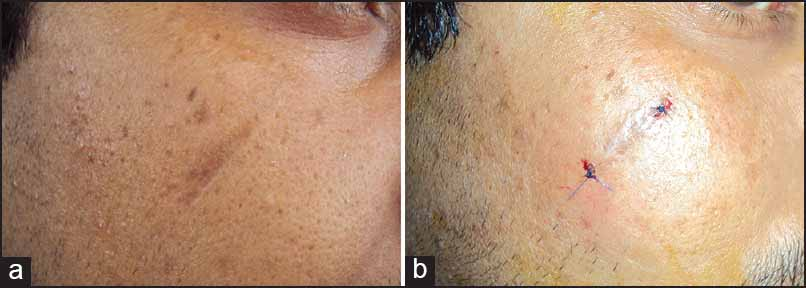
- Appearance of linear atrophic scar before (a) and after (b) treatment
CONCLUSION
Swineheart[1] described a similar technique without railroading which in our experience required more traction pressure and there was always a risk of graft curling and misplacement. The use of snare will produce large entry and exit points in the recipient area. Hence, technical difficulties with handling dermal graft in linear scars are overcome with this railroading technique.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Dermal grafting. In: Klein AW, ed. Tissue Augmentation in Clinical Practice (2nd ed). New York: Taylorand Francis Group; 2006. p. :21-54.
- [Google Scholar]
- Postacne scarring: A review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857-71.
- [Google Scholar]
- Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21:543-9.
- [Google Scholar]
- Surgical management of acne scars. In: Venkatram M, ed. ACS(I) Textbook on Cutaneous and Aesthetic Surgery. New Delhi: Jaypee Brothers Medical Publishers; 2012. p. :392-406.
- [Google Scholar]




