
Translate this page into:
Optimising Laser Tattoo Removal
Address for correspondence: Dr. Kabir Sardana, 466, Sector 28, Noida, UP-201303, India. E-mail: kabirijdvl@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Lasers are the standard modality for tattoo removal. Though there are various factors that determine the results, we have divided them into three logical headings, laser dependant factors such as type of laser and beam modifications, tattoo dependent factors like size and depth, colour of pigment and lastly host dependent factors, which includes primarily the presence of a robust immune response. Modifications in the existing techniques may help in better clinical outcome with minimal risk of complications. This article provides an insight into some of these techniques along with a detailed account of the factors involved in tattoo removal.
Keywords
Laser
tattoo removal
techniques

INTRODUCTION
The practice of tattooing is a rising sociocultural phenomenon that has been seen across various isolated civilisations and countries. Subsequently there is a rising trends of cases demanding laser removal in laser clinics in countries like India, where the armed forces have a stipulation of site-specific removal of tattoos.[1] The initial reports of attempted removal were by salabrasion, use of caustic chemicals, infrared coagulation, electrocautery, and cryotherapy but the significant scarring and residual pigmentation led to their discontinuation. Surgical excision did not always achieve cosmetically pleasing results.[2] In 1963, Goldman documented the first laser application in tattoos, using the normal mode ruby laser which was surprisingly overlooked at the time.[12] Ironically, the scientific-community remained focused on the familiar concept of tissue destruction by ablation which in the continuous mode leads to scarring. Now of course Q-switched lasers form the basis of tattoo removal.[123]
Apart from cosmetic needs, tattoos are also acquired involuntarily by medical need, to demarcate a radiation treatment field or by traumatic embedment of foreign pigmented matter in explosions and other accidents.[12] This results in a wide range of tattoo types but the most relevant classification remains the mode of placement, either professional or amateur.[123] The creation of amateur tattoos with uneven, but superficially placed, monochromatic ink allows excellent laser response with few complications. In contrast, professional tattoos involve a wider variety of pigments that are placed deeply and densely into the dermis.[123] This creates challenges in selecting the appropriate laser and achieving complete clearance.
Amateur tattoos most often employ black Indian ink, but concoctions of organic substances like burnt wood, cotton, and paper, as well as vegetable matter have also been used. Professional tattoos are notorious for their wide range of undocumented chemical compositions and will continue to pose therapeutic challenges, if government regulations are not implemented. Inorganic substances such as metal salts have been used in professional pigments, like chromium green, cobalt blue, or cadmium yellow.[2] These chemicals are known to cause adverse cutaneous reactions.[2] Newer tattoo inks are detailed in the last section of this review.
Laser tattoo removal though an established intervention, is still far from being the easy and perfect method for effective tattoo removal, as is often believed by first-time practitioners.[1] We will attempt to give a succinct overview and then focus on the main aspects that can be varied to enhance the results.
MECHANISMS OF TATTOO REMOVAL
There is a controversy in the literature surrounding the mechanism of tattoo pigment reduction in tissue. The two major mechanisms, which have been proposed for the fragmentation of tattoo ink granules, are thermal and acoustic. Though majority of studies have focused on fragmentation through thermal mechanisms,[4] some have suggested that the acoustic mechanism predominates in short pulsed laser therapy.[56] In contrast, Welch et al.[7] suggested that the laser-induced damage may be caused by a combination of thermal and acoustic effects. Accordingly, a wide range of predicted optimal parameters for laser treatment have been suggested, which make the settings and parameters subject to variation.
The ultimate goal is to minimise sessions and maximise results. Total clearance of a tattoo is not often seen and one study reported that only three of 238 paying patients achieved this goal.[8] Thus, a constant endeavour is to optimise laser parameter selection, increase the efficacy of each treatment session, and minimise the total number of treatment sessions required.[128]
VARIABLES DETERMINING TATTOO REMOVAL
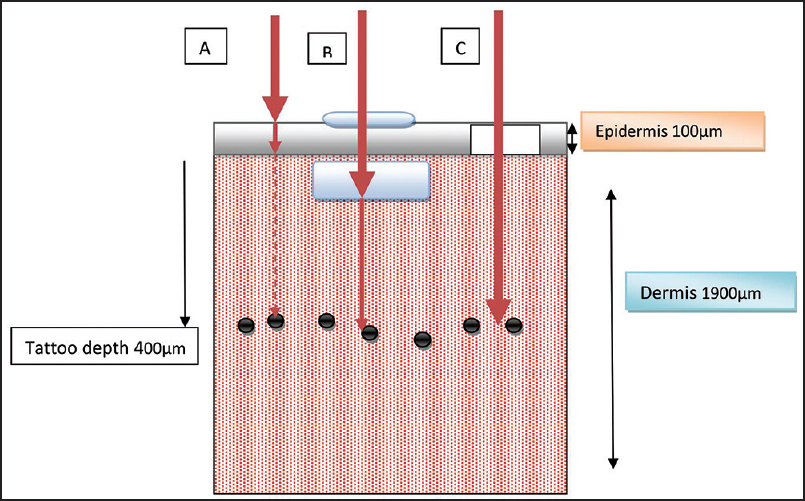
To understand the response rate of lasers, it is imperative to first understand the variables involved in tattoo removal which are depicted in Figure 1 and Table 1. Three broad aspects are involved, the laser(s) used, the skin phenotype and tattoo dependant factors, which includes the type, depth and size of tattoo [Figure 1]. A rarely appreciated aspect of tattoo removal is the role of the host immune response, which ultimately phagocytoses the tattoo particles and drains them away via the lymphatics.[123] Thus it is the inflammation consequent to the laser therapy and the concomitant stimulation of the host response that ultimately results in removal of tattoo ink via the lymphatics.[3]

- Variables that affect tattoo removal. The normal process involves fragmentation followed by phagocytosis and transport via the lymphatics. Each step (a-e) plays a role and thus the variations in results are enormous. The colour and mix of tattoo colour is probably the most important determinant in laser application for tattoo. (Not Drawn to Scale)
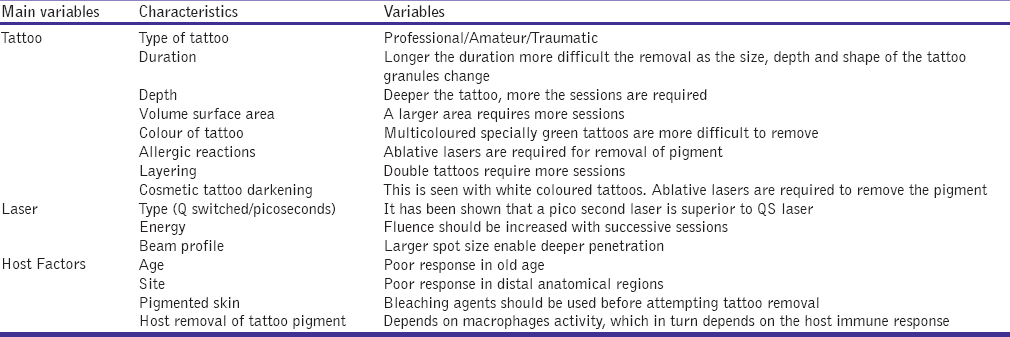
Thus an efficient removal of tattoo requires a modification and enhancement of the laser, the tissue and the host response [Figure 1].[1]
Laser-dependent factors
It is well accepted that the number of sessions depend more on the kind of the tattoo than on the laser used, thus 5-10 sessions are standard for amateur tattoos and 15-20 for professional tattoos, even up to 25 sessions in rare cases.[2] The number of treatment sessions also depends on pigment colour, composition, density, depth, age of the tattoo, body location, and the amount of tattoo ink present.[2] Thus a substantial part of research is directed towards modulating the laser to maximise results. The Q-switched laser systems remain the treatment of choice for tattoo removal, as emphasised by many reviews and studies [Table 2]. While more than one laser type may be required for multicoloured tattoos, appropriate device selection can achieve clearance with a low incidence of scarring or permanent pigmentary alterations. The QSRL was the first of the QS laser systems to be explored in tattoo removal. Studies have found that black and dark blue pigments respond well to the QSRL treatment (Taylor CR et al.).[9] QSRLs can help clear green pigment as well (Kilmer et al.).[10] The frequency-doubled QS Nd:YAG with 532 nm facilitates clearance of red pigments after an average of three treatments (Kilmer et al.)[10]
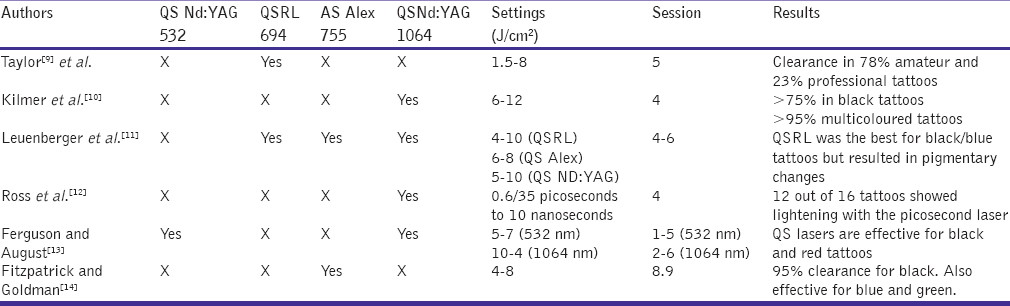
In general, professional tattoos are harder to remove, requiring 6-10 or up to 20 treatment sessions [Table 2]. More recently placed tattoos with deeply located pigment on a distal site are harder to remove due to the reduced lymphatic distribution which helps in removing residual ink particles. Although a comparative study by Leuenberger et al.[11] found that QSRL to be the best laser, it can lead to pigmentary alterations in pigmented skin type. The QS Nd:YAG 1,064-nm device is the “workhorse” laser for removal of blue-black pigments in darker skin types as its longer wavelength is less competitively absorbed by melanin and thus fewer pigmentary alterations result (Kilmner et al.).[10]
We will focus on the novel aspects that can maximise results by tweaking the laser systems commonly employed.
R20 Method and its modifications
This method is based on the observation that the “whitening” that occurs after most Q-switched lasers can prevent successive laser pulses to penetrate into the dermis. To obviate this repeated sessions after an interval of 20 minutes between pulses[1516] can help dissipate this phenomenon and thus multiple passes can be achieved in a single session.
This method has two drawbacks, one it is time consuming and secondly, it has not been adequately studied with other wavelengths, like 1064 nm, which are frequently employed in pigmented skin. There is another issue with this method, as there is a change in the size of the tattoo pigment, which after the first impact will have an altered optical property and size which will change the optical absorption of the pigment. Thus probably the QS mode may not be ideal for the remnant tattoo particles. Moreover, the 1064 nm, used in pigmented skin has a higher photothermal impact and depth than the 755-nm laser used originally and repeated passes may cause more thermal injury while using the 1064-nm device.
A modification of this method has been proposed where application of topical perfluorodecalin (PFD),[16] a highly gas soluble liquid fluorocarbon, that resolves the whitening reaction within seconds, (R0 method) thus obviating the waiting time of 20 minutes.
Spot size of QS laser
Q-switched lasers used for tattoo removal are limited in the amount of total energy they can deliver, as are all lasers. However, with Q-switched lasers, the beam diameters available to deliver clinically meaningful fluences are more limited than other lasers, such as those used for laser hair removal or treatment of vascular lesions. It is a well accepted practice “gem” that in case of a non-responsive tattoo, it is better to increase the spot size than the dose as the former helps in better penetration due to less scattering of the laser beam.[12]
A study comparing the QS laser (1064, 533 nm) with a variable spot size versus the conventional 4-mm-diameter spot size showed significantly more clearance of tattoo pigment in the former group.[17] Because tattoo ink fades with each treatment, increasing fluences are necessary to achieve optimal tattoo removal with each subsequent treatment [Table 1]. If too high fluence is used, especially during the initial treatment sessions when the tattoo is darkest, injury to the skin with scarring can occur. A dynamic spot diameter would,[17] progressively get smaller as the fluence gets higher thus avoiding unnecessary thermal injury. This is contrary to most QS lasers where a 2 to 3-mm diameter spot size is used to achieve fluences as high as 12 J/cm2 at 1064 nm, which can cause more thermal damage. Thus a QS laser with a dynamic diameter can enhance the results with less thermal damage.[17]
Pulse diameter (Picosecond lasers)
Most tattoo pigments have a particle size of 30-300 nm, corresponding to a thermal relaxation time of less than 10 nanoseconds.[18] Thus an ideal laser should have a pulse duration in nanoseconds, which is the logic of using QS lasers (10-9 s). Newer laser technologies shorten that pulse time to picoseconds (10-12 s), promising more effective results in tattoo removal.[1]
This concept was proposed by Ross and colleagues,[12] who had reported that for the same laser energy, tattoo removal becomes more efficient as the laser pulse length is shortened to the picosecond range. In a side-by-side comparison of response of tattoos to picosecond and nanosecond QS (1064-nm) Nd:YAG lasers, they found that 12 out of 16 black tattoos showed greater lightening with a pulse duration of 35 picoseconds than with a pulse duration of 10 nanoseconds. This was replicated by Herd et al.[19] and Izikson et al.[18] using a picosecond titanium: sapphire (795-nm, 500 picoseconds) laser and the QS alexandrite (758-nm, 50 nanoseconds) laser in a porcine model. Both studies found a greater clearance of tattoos treated by picosecond lasers. Brauer et al.[20] further reported the successful and rapid treatment of 12 tattoos containing blue and/or green pigment with the novel, picosecond, 755-nm alexandrite laser. They demonstrated a 75% clearance of blue and green pigment after 1 or 2 treatments, with more than two-thirds of these tattoos more closely approaching 100% clearance.
Inspite of this novel technology, there are certain contrarian views on the picoseconds laser. The first is a practical commercial view, wherein all QS lasers will have to be replaced by picoseconds lasers, adding to the cost of therapy. There are other fundamental arguments against the concept of reduced pulse width in this indication. Humphries et al.[21] had elegantly demonstrated that, variations in the pulse width had little influence on the fragmentation response. Also experimental data on the effect of laser fluences on skin whitening for a wide range of tested pulse durations, has shown that the plasma formation threshold changed only slightly, even though the pulse duration varied by a factor of 25 (from 2 to 50 nanoseconds). It is thus highly unlikely that shortening of the pulse duration by another factor of 2.5 (to obtain sub-nanosecond pulses) would result in any further significant change.[21] The plasma formation in highly absorbing tissues is insensitive to pulse duration and thus reducing the pulse duration into the sub-nanosecond range will not contribute significantly to the thermal mechanisms involved in tattoo removal. The predominant mechanism with sub-nanosecond pulses, is the fracturing of tattoo particles under increased mechanical stress. However, as has been shown, tattoo particle fragmentation does not occur even when 20-times shorter (e.g., 35 ps) pulses are used.[12]
Ross et al.[12] had shown that temperature-induced changes, rather than particle fragmentation, are responsible for tattoo clearing. It is also worth noting that picosecond pulses of a sufficiently high fluence are difficult to generate, and that consequently the picosecond lasers are capable of delivering fluences above plasma formation threshold only at small spot sizes. These small spot sizes result not only in procedures being slow, but also result in unacceptable scattering losses, so that the tissue penetration and treatment efficacy are compromised.[12]
Thus picoseconds lasers may require more data and studies with other wavelengths and in pigmented skin types before they can be widely implemented in clinical practise.
Fluence and progressive escalation
In case of professional tattoos the ink granules are relatively homogeneous in size and depth.[22] This makes the prediction of optimal laser settings a more reliable exercise as compared to amateur tattoos, or tattoos comprising various colours [Table 1]. The purpose of laser treatment is to fragment the ink granules so that the resulting fragments are more likely to be absorbed through macrophagic processes.[23] Successive treatments result in fewer and smaller ink granules. Thus, if laser parameters are not altered to account for the progressive reduction in the size and number of the ink granules, greater number of treatment sessions may be required to reach a satisfactory clinical end point.
An in vitro model,[2122] had predicted that the optimal absolute fluence for the initial session should be in the range of 7 J/cm2, while for the latter session it should be 11 J/cm2 to achieve maximal ink fragmentation while maintaining only a small risk of thermal damage. This can be used as a rough guide for dose settings in clinical practice.
Wavelength of laser in relation to tattoo colour
Though three lasers, the QS ruby laser, QS Nd:YAG and QS alexandrite laser are used commonly, as the tattooed pigment comes in a wide range of colours, multiple wavelengths of laser light are required to successfully remove tattoos.[122425] A depiction of the ideal laser for various coloured tattoos is given in Figure 2 and Table 3.
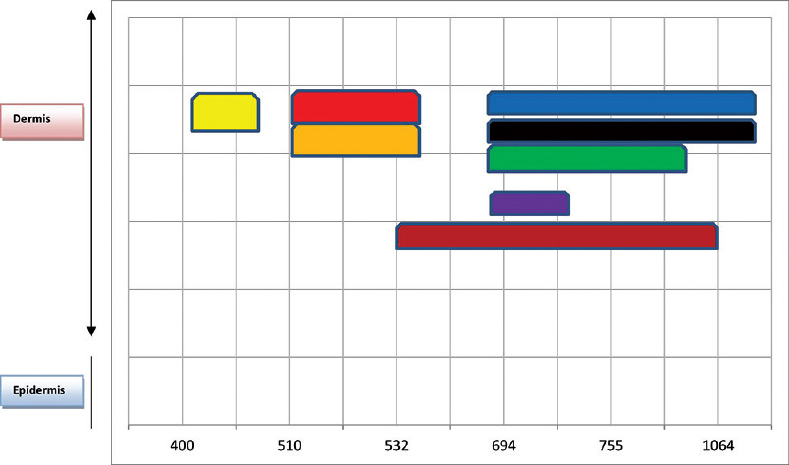
- The various pigment colours are depicted inset and correspond to the absorption spctrum of the wavelengths
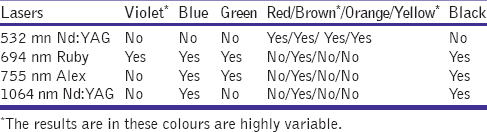
Studies have shown that dark pigmented tattoos can theoretically be treated by any laser, because black absorbs virtually every wavelength of light [Figure 2].[24] Some authors[11] have found the QS 694-nm ruby and QS 755-nm alexandrite laser to be superior for black-blue tattoos as compared to the 1064-nm QS Nd: YAG, but these treatments are frequently associated with transient pigmentary changes, and are not preferred in pigmented skin.[2] Thus the 1064-nm QS Nd:YAG laser is probably the ideal laser for blue-black tattoos. Orange, red and red-brown pigments, in particular, respond well to 532 nm.[2526] The QS 755-nm alexandrite and the QS 694-nm ruby laser are the ideal lasers for the removal of green-coloured tattoos, whereas purple and violet ink respond best to the QS 694-nm ruby laser [Figure 2].[13242526]
Gomez et al.[27] found that for red, orange, and rose inks 532 nm was the ideal wavelength, for brown 1064 nm, yellow and green 448 nm and for blue 600 nm. Some of these wavelengths (448 nm, 600 nm) are not available commercially available laser and highlight the issue of the variable end result that is achieved in multi-coloured tattoos. Though there are studies[227] that have used reflectance spectroscopy to determine the ideal wavelength for the most common colours, for many colours the ideal wavelength is not yet known.
Use of combination of lasers
A novel concept that was first propounded by Goldman MP and Fitzpatrick RE[28] was based on ablation of the epidermis which helped to target the dermal tattoo pigment with less beam scattering and faster results.[2930] This technique fell out of favour as conventional ablative lasers lead to scarring that is consequent to the use of doses and settings that exceed the thermal relaxation time of the skin. But pulsed lasers like Er:YAG and the ultrapulsed CO2 lasers can be used to precisely remove epidermal layers.[2930] This was studied using a combination of ultrapulse CO2 laser followed by QS Nd:YAG,[29] in a split lesion design which lead to a significant reduction in the number of sessions with negligible side effects [Figure 3]. This has been further modified using the Er:YAG followed by the QS Nd:YAG with better results and has been christened the Rapid Tattoo Removal technique (RTR).[30]
- A schematic diagram highlighting techniques to enhance tattoo removal. (a) The laser beam gets attenuated by the epidermis and the dermis due to epidermal and dermal scattering (b) Topically applied clearing agents can help in reducing the dermal scatter and enhance results. They can be placed either on the skin or intradermally (c) Epidermal ablation is another effective tool for enhancing results by eliminating epidermal scatter
Another option is to use a combination of fractional ablative laser and QS laser,[3132] though in our experience this is not as effective as using a pulsed ablative laser this technique creates micro-ablation zones, through which the QS lasers are presumed to penetrate more effectively into the dermis. This needs a spot diameter that corresponds to the micro ablation zones created by the fractional laser. Probably an accurate and complete ablation of the epidermis followed by QS laser is a more appropriate method when emergent tattoo removal is required.[282930]
Tissue-dependent factor
Manipulation of the laser tissue interface
An elegant concept that can be used to improve results is by manipulating the interface between the laser and the tattoo. This will effectively lead to reduced scatter and attenuation of the laser energy, thus resulting in enhanced results [Figure 3]. This can be achieved by various means.
-
Epidermal injury can be reduced by topical application of hyperosmotic solutions prior to laser therapy, such as sucrose, glycerol, and water-soluble gels (e.g., surgilube) that have a refractive index matching closely to that of stratum corneum, i.e, 1.4[33] which will in effect reduce the surface scatter from incident light. The problem being that such solutions are highly hydrophilic and penetrate intact skin very poorly when applied topically.[3435]
Khan et al.[36] used clearing agents such as polypropylene glycol and polyethylene glycol (PPG, PEG) which allowed more photons to reach the target apart from reducing the scattered light. The scattering coefficient of epidermis and superficial papillary dermis (upper 200-300-μm thickness) reduced from 0.4 mm-1 to 0.2-0.1 mm-1 after the application of these clearing agents. The resulting heat source term profiles showed a 40% decrease at the dermoepidermal junction (DEJ) due to reduced epidermal scattering, thus predicting a safer tissue impact profile.
-
Another option is to reduce dermal scatter is by using a transdermal application of a clearing agent (glycerol)[37] which has been shown to improve treatment outcomes in tattoos [Figure 3].
-
A third modification has been described above,[282930] wherein a pulsed laser can be used to remove the epidermis, which eliminates the epidermal diffraction and scatter and this has been shown to reduce the number of sessions markedly.
Tattoo-dependent factors
The role of colour [Table 3, Figure 2] has been extensively dealt with (above) and the effect of the method of insertion (professional/amateur) is well established.
Size of tattoo particle
The characteristics of tattoos and the pigment have been shown to vary with each treatment session.[22] The diameters of tattoo ink granules have been measured, wherein before irradiation the granules within the dermis have a maximum diameter of 6 μm. This mean diameter reduces after successive laser treatment. Since the maximum diameter of granule that can be absorbed by the lymphatic system is approximately 0.4 μm,[22] any laser procedure that tries to fractionate them further is of little clinical use. This scientific concept goes against the concept of the R20R technique, as repeated thermal damage to the tattoo has little effect once the particle size of 0.4 μm is reached.
It has been shown that larger granules, are shown to reach higher temperatures and therefore have a greater chance of fragmentation compared to smaller granules found in later treatment sessions. As smaller granules absorb less energy, larger spot diameters and higher fluence settings are needed to reach the appropriate granule temperatures.[21] Though this concept is generally true, it is also dependent on the colour of the tattoo.
A recent study[38] theorized that black tattoo ink's excellent response to Q-switched lasers was associated with its strong absorption and small particle size. White tattoo ink's poor response was associated with its poor absorption and the large particle size. Thus the results of lasers is dependent both on the size and the colour of the tattoo pigment
Depth of tattoos
The granule depth remains uniform and is located at a depth of about 400 μm, as professional tattoos are generally located in the upper to mid-dermis region [Figure 3].[22] This explains the difficulty in treating these tattoos as compared to amateur tattoos which are superficially placed.
An interest concept was proposed by Ho et al.[5] who demonstrated that laser fluence attenuates rapidly in the dermis, thus a lower-intensity laser may used first for the removal of the top layer of the tattoo pigment. Subsequent sessions, with increasing fluence can help remove the pigment deep inside the dermis. This sequence can minimize the overall laser energy, and consequently reduce the collateral damage.
Composition of tattoo dye
Detailed knowledge with respect to the identity and dye composition of tattoo pigments would be beneficial not only with regard to photoallergic, granulomatous, and anaphylactic reactions but will also be useful in improving treatment planning and response prediction to laser therapy.[22439] Klitzmand[40] designed a permanent and more removable tattoo ink using insoluble and bioresorbable pigments (such as beta-carotene and iron oxide), which are stabilised through microencapsulation in transparent polymethylmethacrylate (PMMA) beads. The microspheres contain discrete pigment that can be targeted by specific laser wavelengths. Laser-based tattoo removal causes the capsule to break, exposing the pigment, which is then reabsorbed by the body. Thus one laser treatment can effectively remove 80% of tattoo pigment, contrary to the 20% removal with conventional ink. Although these results appear promising, the safety and efficacy of microencapsulated tattoo ink in human skin needs to be investigated in further studies as no clinical data have yet been published.
Host-dependent factors
This aspect has not been studied but may be the most important determinant in successful removal of tattoo pigment. This is as the laser merely works by disruption of the tattoo and it is the host tissue response that effects the phagocytosis and expulsion of the tattoo from the skin via the lymphatics.[3426] Patients suffering from short- and long-term immunosuppression (i.e., via chemotherapy, drug-induced, or a medical condition) may experience poor healing, which can further lead to ink retention following laser treatments.[41] This is specially relevant in patients on oral steroids, azathioprine and cyclophosphamide, often prescribed by dermatologists.
Individuals presenting with underlying immunosuppression should be referred to the appropriate specialist for comprehensive care. Once the condition has stabilised or resolved, they should be considered appropriate candidates for laser tattoo removal treatment
CONCLUSIONS
Lasers are the established gold standard for tattoo removal, but employing the appropriate device and technique does not always guarantees a successful outcome. The mechanisms responsible for variable responses of cosmetic tattoos to laser treatment are numerous and often interrelated [Table 1, Figure 1]. Removal of the tattoo depends on various factors including the type of tattoo and the dye used, the depth of the tattoo pigment, the type of lasers and different techniques using combination of lasers. It also is largely dependent on the wavelength, and fluence of the lasers used. Lasers in the picosecond (10-12) domain are currently under development but not as yet commercially viable. Various scenarios that lead to delayed results that may confront the clinician are listed in the table [Table 4][4243444546474849505152] with the possible laser interventions than can help to circumvent these factors.
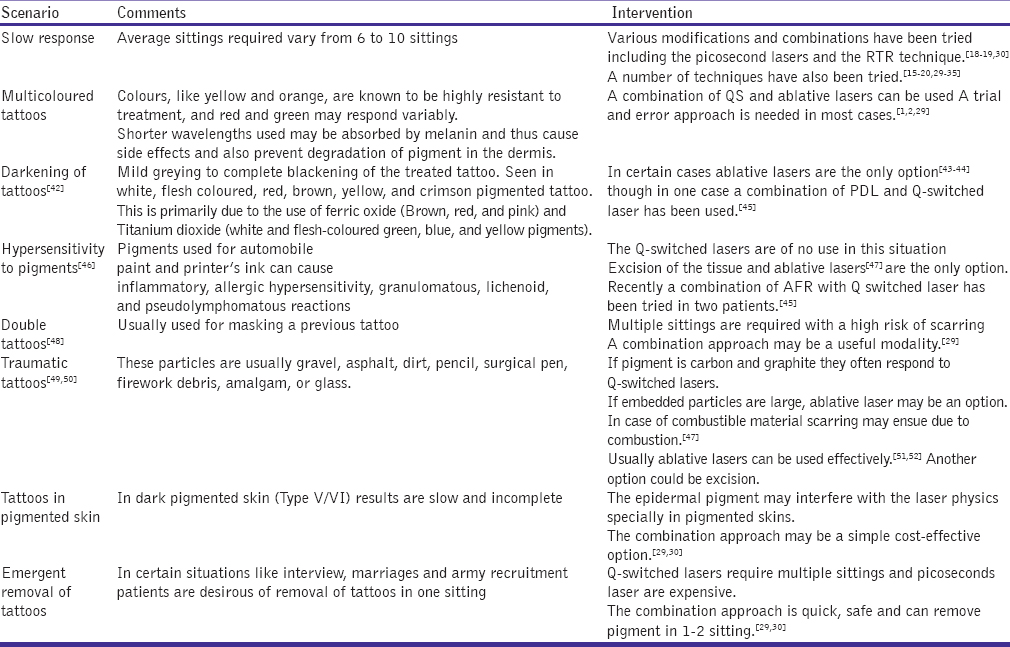
This wide array of variations means that effective and satisfactory response in tattoos is still an exacting science.[4243444546474849505152] Tragically, laser tattoo removal has inevitably lead to more tattooing which is unfortunate as a tattoo is never more beautiful than the skin onto which it is placed.[53] Though a permanent solution would entail making tattoos safer and more removable than ever[229] but as the laser industry and the tattoo practitioner are on different poles, the aim of a faster tattoo removal will remain a difficult goal to achieve for laser physicists and practitioners.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Pigmented lesions and tattoos. In: Sardana K, Garg VK, eds. Lasers in Dermatological Practice (1st ed). New Delhi: Jaypee Brothers; 2014. p. :101-60.
- [Google Scholar]
- Laser treatment of tattoos and other dyschromia. In: Raulin C, Karsai S, eds. Laser and IPL Technology in Dermatology and Aesthetic Medicine. Berlin, Heidelberg: Springer-Verlag; 2011. p. :189-210.
- [Google Scholar]
- The Q-switched neodymium: YAG laser and tattoos: A microscopic analysis of laser-tattoo interactions. Br J Dermatol. 1997;137:405-10.
- [Google Scholar]
- The thermal response of laser irradiated tissue. J Quantum Electron. 1984;20:1471-81.
- [Google Scholar]
- Laser-tattoo removal — A study of the mechanism and the optical treatment strategy via computer simulations. Lasers Surg Med. 2002;30:389-97.
- [Google Scholar]
- Selective photothermolysis: Precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524-7.
- [Google Scholar]
- Optical-thermal response of laser-irradiated tissue. (1st ed). New York: Plenum Press; 1995. p. :561-606.
- [Google Scholar]
- Patient compliance as a major determinant of laser tattoo removal success rates: A 10-year retrospective study. J Cosmet Laser Ther. 2010;12:166-9.
- [Google Scholar]
- Treatment of tattoos by Q-switched ruby laser. A dose-response study. Arch Dermatol. 1990;126:893-9.
- [Google Scholar]
- The Q-switched Nd: YAG laser effectively treats tattoos. A controlled, dose-response study. Arch Dermatol. 1993;129:971-8.
- [Google Scholar]
- Comparison of the Q-switched alexandrite, Nd: YAG, and ruby lasers in treating blue-black tattoos. Dermatol Surg. 1999;25:10-4.
- [Google Scholar]
- Comparison of responses of tattoos to picosecond and nanosecond Q-switched neodymium: YAG lasers. Arch Dermatol. 1998;134:167-71.
- [Google Scholar]
- Evaluation of the Nd/YAG laser for treatment of amateur and professional tattoos. Br J Dermatol. 1996;135:586-91.
- [Google Scholar]
- Optimal tattoo removal in a single laser session based on the method of repeated exposures. J Am Acad Dermatol. 2012;66:271-7.
- [Google Scholar]
- Topical perfluor-odecalin resolves immediate whitening reactions and allows rapid effective multiple pass treatment of tattoos. Lasers Surg Med. 2013;45:76-80.
- [Google Scholar]
- A continuously variable beam-diameter, high-fluence, Q-switched Nd: YAG laser for tattoo removal: Comparison of the maximum beam diameter to a standard 4-mm-diameter treatment beam. Lasers Surg Med. 2013;45:621-7.
- [Google Scholar]
- Safety and effectiveness of black tattoo clearance in a pig model after a single treatment with a novel 758 nm 500 picosecond laser: A pilot study. Lasers Surg Med. 2010;42:640-6.
- [Google Scholar]
- A clinical and histologic prospective controlled comparative study of the picosecond titanium: Sapphire (795 nm) laser versus the Q-switched alexandrite (752 nm) laser for removing tattoo pigment. J Am Acad Dermatol. 1999;40:603-6.
- [Google Scholar]
- Successful and rapid treatment of blue and green tattoo pigment with a novel picosecond laser. Arch Dermatol. 2012;148:820-3.
- [Google Scholar]
- Finite element analysis of thermal and acoustic processes during laser tattoo removal. Lasers Surg Med. 2013;45:108-15.
- [Google Scholar]
- Light and electron microscopic analysis of tattoos treated by Q-switched ruby laser. J Invest Dermatol. 1991;97:131-6.
- [Google Scholar]
- Tattoo removal with the Q-switched ruby laser and the Q-switched Nd: YAGlaser: A comparative study. Cutis. 1995;55:291-6.
- [Google Scholar]
- Clinical, histologic, and ultrastructural evaluation of tattoos treated with three laser systems. Lasers Surg Med. 1994;15:364-72.
- [Google Scholar]
- In vitro and in vivo laser treatments of tattoos: High efficiency and low fluences. Arch Dermatol. 2010;146:39-45.
- [Google Scholar]
- Carbon dioxide laser surgery. In: Goldman MP, Fitzpatrick RE, eds. Cutaneous Laser Surgery (2nd ed). USA: Elseiver; 1999. p. :302.
- [Google Scholar]
- A promising split-lesion technique for rapid tattoo removal using a novel sequential approach of a single sitting of pulsed CO(2) followed by Q-switched Nd: YAG laser (1064 nm) J Cosmetic Dermatol. 2013;12:296-305.
- [Google Scholar]
- A rapid tattoo removal (RTR) technique using a combination of pulsed Er: YAG and Q Switched Nd: YAG in a split lesion protocol. J Cosmet Laser Ther 2015:1-24.
- [Google Scholar]
- Combining fractional resurfacing and Q-switched ruby laser for tattoo removal. Dermatol Surg. 2011;37:97-9.
- [Google Scholar]
- Treatment of tattoo allergy with ablative fractional resurfacing: A novel paradigm for tattoo removal. J Am Acad Dermatol. 2011;64:1111-4.
- [Google Scholar]
- Light propagation in tissues with controlled optical properties. J Biomed Opt. 1997;2:401-17.
- [Google Scholar]
- Concurrent enhancement of imaging depth and contrast for optical coherence tomography by hyperosmotic agents. J Opt Soc Am B. 2001;18:948-53.
- [Google Scholar]
- Can topically applied optical clearing agents increase the epidermal damage threshold and enhance therapeutic efficacy? Lasers Surg Med. 2004;35:93-5.
- [Google Scholar]
- Temporary dermal scatter reduction: Quantitative assessment and implications for improved laser tattoo removal. Lasers Surg Med. 2005;36:289-96.
- [Google Scholar]
- Effects of tattoo ink's absorption spectra and particle size on cosmetic tattoo treatment efficacy using Q-switched Nd: YAG laser. Lasers Med Sci. 2015;30:303-9.
- [Google Scholar]
- In vitro quantitative chemical analysis of tattoo pigments. Arch Dermatol. 2001;137:143-7.
- [Google Scholar]
- Development of permanent but removable tattoos. In: Federal Institute for Risk Assessment, Press and Public Relation. First International Conference on Tattoo Safety. Berlin: BFR-Symposium; 2013. p. :23.
- [Google Scholar]
- Causes and recommendations for unanticipated ink retention following tattoo removal treatment. J Clin Aesthet Dermatol. 2013;6:27-31.
- [Google Scholar]
- Colour shift following tattoo removal with Q-switched Nd-YAG laser (1064/532) Br J Plast Surg. 1999;52:482-7.
- [Google Scholar]
- Surgical pearl: Removal of cosmetic lip-liner tattoo with the pulsed carbon dioxide laser. J Am Acad Dermatol. 2003;48:271-2.
- [Google Scholar]
- Ultrapulse carbon dioxide laser treatment of an iron oxide flesh-colored tattoo. Dermatol Surg. 1997;23:60-1.
- [Google Scholar]
- Successful treatment of a cosmetic tattoo using a combination of lasers. Dermatol Surg. 2004;30:105-7.
- [Google Scholar]
- Comparison of two Q-switched lasers and a short-pulse erbium-doped yttrium aluminum garnet laser for treatment of cosmetic tattoos containing titanium and iron in an animal model. Dermatol Surg. 2010;36:1656-63.
- [Google Scholar]
- Scarring following Q-switched laser treatment of “double tattoos”. Arch Dermatol. 2000;136:269-70.
- [Google Scholar]
- The neodymium: YAG laser in the treatment of traumatic tattoo: A case report. J Oral Maxillofac Surg. 2006;64:850-5.
- [Google Scholar]
- Laser ignition of traumatically embedded firework debris. Lasers Surg Med. 1998;22:157-8.
- [Google Scholar]
- Traumatic tattoo: Use of the variable pulsed erbium: YAG laser. Photomed Laser Surg. 2006;24:605-9.
- [Google Scholar]
- Early treatment of traumatic tattoo by erbium-YAG laser. Br J Dermatol. 2001;144:219-21.
- [Google Scholar]
- Regarding tattoos: Is that sunlight, or an oncoming train at the end of the tunnel? Arch Dermatol. 2001;137:210-2.
- [Google Scholar]




