
Translate this page into:
Repair of Minor True Hare Lip Using V–Y Plasty: How I Do It
Address for correspondence: Dr. Abdelrahman E.M. Ezzat, Department of ENT, Faculty of Medicine, Al-Azhar University Hospitals, Cairo, Egypt. E-mail: aemei_ibrahim@yahoo.co.uk
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Minor true hare lip is rare central midline deficiency of the upper lip. There are multiple techniques but little consensus on the preferred surgical technique.
Materials And Methods:
A transoral approach for repair using mucosal V–Y plasty is described by employing a vertical inverted V incision.
Result:
The contour of the free labial border immediately improves with avoidance of skin scar.
Conclusions:
The midline cleft lip notch or minor true (hare lip) midline clefts can be effectively treated by mucosal lengthening using a V–Y plasty. Moreover, the ability to augment the tubercle with mucosa through a VY plasty is simple and easy.
Keywords
Midline cleft lip
mucosal V–Y plasty
true hare lip

BACKGROUND
Multiple terms have been used to describe the constellations of abnormalities observed with true midline clefts (hare lip), including median cleft face syndrome[1] and Tessier's grade 0 clefts.[2] The incidence of midline cleft of the lip or Tessier's grade 0 cleft is reported to be about 0.43% to 0.73% of the craniofacial cleft population.[3]
Hypertelorbitism, midline craniofacial osseous defects, hairline abnormalities and a midline upper lip cleft may be present to varying degrees in these cases.[4] However, the mildest form including a small notch in the soft tissue of the upper lip that does not cross the vermillion border could occur.[5]
Multiple techniques have been described to repair the median cleft lip deformity. I describe a transoral mucosal V–Y plasty and midline orbicularis oris muscle repair for midline cleft lip notch.
MATERIALS AND METHODS
Clinical presentation
A 17-year-old female presented with a notch in the upper lip including the wet and dry mucosa crossing the vermillion border [Figure 1a]. The maxillary alveolus was notched at the midline, but no osseous cleft was present. Other pertinent facial findings included a shortened nasal length with deviation of the anterior nasal opening on the right side and normotelorism [Figure 1b]. The nasal septum and anterior nasal spine was shifted to the right side.
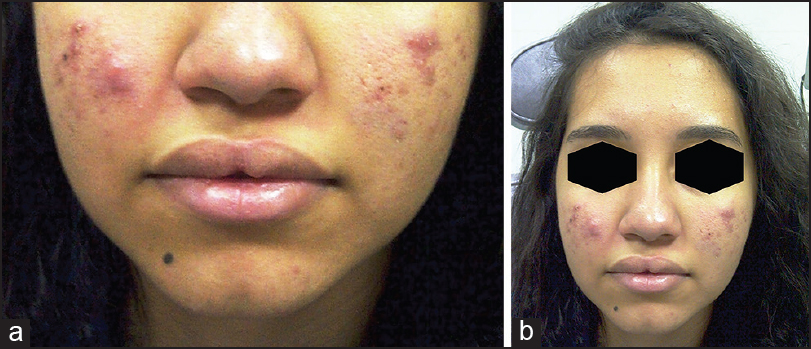
- (a) Preoperative picture of the patient's lip. (b) Preoperative picture of the patient
Surgical technique and outcome
A V–Y plasty was designed by donning a vertical inverted V incision (with the apex upward) in the mucosal side of the upper lip [Figure 2a]. Raising the mucosal flaps exposed the orbicularis oris muscle, which was separated from each other and the underlying median cleft notch between the two muscles [Figure 2b]. The orbicularis oris muscle was dissected on both sides and united in the midline using horizontal mattress sutures [Figure 2c]. Using a 5-0 Vicryl, the V-shaped mucosal flap was sutured into a position as Y shaped giving an additionally mucosal length [Figure 2d]. The extra piece of mucosa was excised. The nasal correction was done in the same site with repositioning of the lower lateral cartilage for tip repositioning, with maxillary augmentation (lengthening of the lower lateral cartilage and elevation of the nasal dorsum) with septal cartilage [Figure 3a–d]. The notch was corrected immediately and appropriate lip height and fullness were achieved with maintenance of shape for 1 year postoperatively [Figure 4a and b].
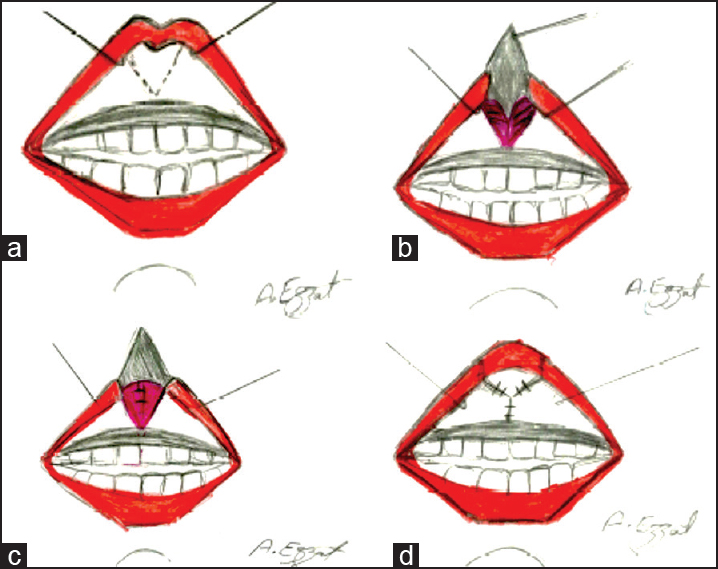
- (a) Intraoperative diagrams showing vertical inverted V incision (with the apex upward) in the mucosal side of the upper lip. (b) Separation of the two orbicularis oris muscles from each other and the underlying median cleft notch between them. (c) The orbicularis oris muscle dissected on both sides and united in the midline using horizontal mattress sutures. (d) The V-shaped mucosal flap sutured into position as Y shaped, giving an additionally mucosal length
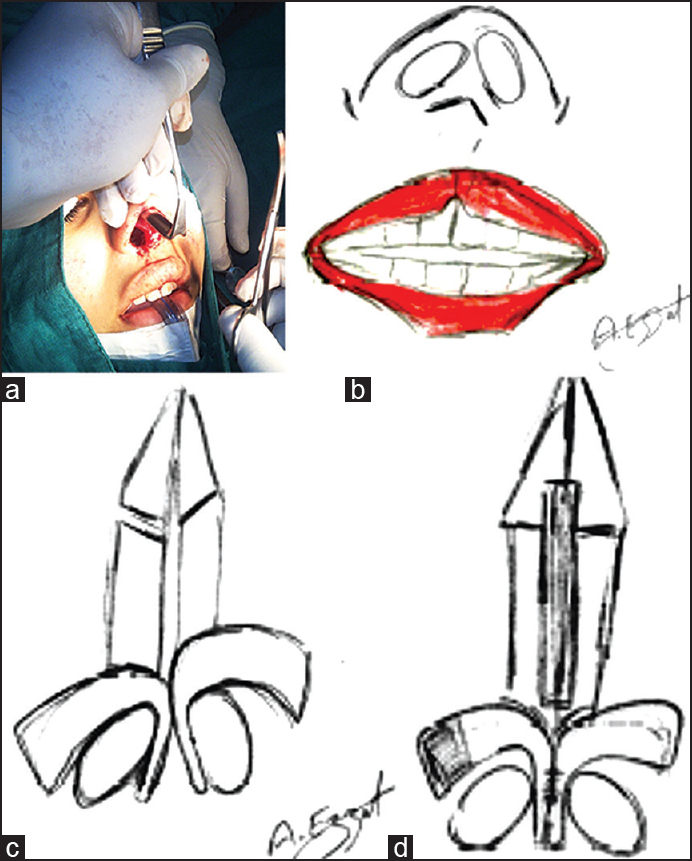
- (a) Intraoperative image of the nasal correction. (b) Diagram of the lip and nasal deformity. (c) Intraoperative diagram of the nasal deformity. (d) Intraoperative diagram showing the correction of the nasal deformity
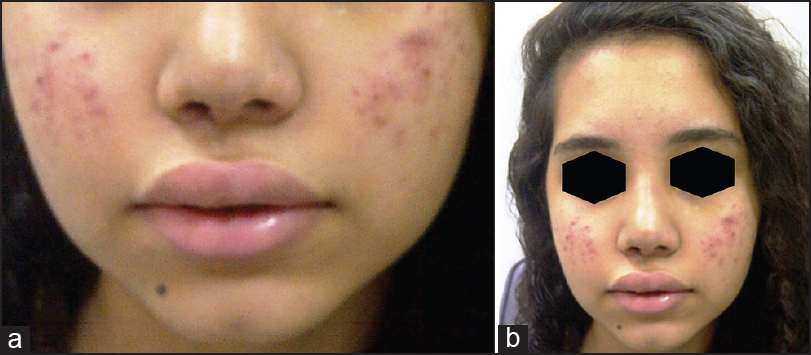
- (a) One year postoperative picture of the patient's lip. (b) One year postoperative picture of the patient
DISCUSSION
In 1937, Veau classified three varieties of median clefts: Notch of the lip, median cleft extending to the columella and a defect due to atrophy of midline facial structures.[6] DeMyer described two groups of syndromes associated with the median cleft lip. The first is associated with orbital hypotelorism and the second with hypertelorism.[1] In this case report, the patient described had a midline cleft of the upper lip without any deformities of philtrum and minor nasal opening shift with normotelorism.
Surgical correction of the true harelip has been described for both minor and severe defects. Weimer[7] described the excision of a diamond-shaped piece of skin and mucosa, as well as a fibrotic band with overlap of the orbicularis oris muscle and a zigzag closure of the mucosa. Buonocore et al.,[8] described a Z-plasty designed on either side of the elongated frenulum with excision of the constriction band.
Urata and Kawamoto[9] described a hidden intraoral incision to correct a mild deformity, which does not cross the vermillion border. Therefore, I have done an intraoral incision and I have found that the intraoral incision allows orbicularis oris muscle and provides the surgeon with the ability to augment the tubercle with mucosa through a V–Y plasty.
CONCLUSIONS
The midline cleft lip notch or minor true hare lip midline clefts can be effectively treated by mucosal lengthening using a V–Y plasty, which successfully releases the notched lip, provides mucosal length and vermillion fullness and with avoidance of skin scar. Moreover, the ability to augment the tubercle with mucosa through a VY plasty is simple and easy.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Familial alobar holoprosencephaly (Arhinencephaly) with median cleft lip and palate. Report of patient with 46 chromosomes. Neurology. 1963;13:913-8.
- [Google Scholar]
- Anatomical classification of facial, cranio-facial, and latero-facial clefts. J Maxillofac Surg. 1976;4:69-92.
- [Google Scholar]
- The bifid nose. With a report of 3 cases of siblings. Plast Reconstr Surg. 1965;36:626-8.
- [Google Scholar]
- Hasencharten menschlicher Keimlinge auf der Stufe 21-23 mm SSL. Z Anat Entwiclungsgesch. 1937;108:459. Quoted from, Patel NP, Tantri MD. Median cleft of the upper lip: A rare case. Cleft Palate Craniofac J 2010;47:642-4
- [Google Scholar]
- Anatomical findings in median cleft of upper lip. Plast Reconstr Surg. 1978;62:866-9.
- [Google Scholar]
- Repair of the median microform cleft lip using Z-plasty. Mode Plast Surg. 2012;2:43-5.
- [Google Scholar]
- Median clefts of the upper lip: A review and surgical management of a minor manifestation. J Craniofac Surg. 2003;14:749-55.
- [Google Scholar]




