
Translate this page into:
Elective Tongue Piercing: Fad with Fallout
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Body piercing is one of the oldest forms of adornment and body modification,[1] which can be dated back to antiquity, reported across a wide range of cultures. Ancient Mayans considered piercing as a symbol of spirituality and courage. Eskimos inserted a ‘labret’ into the lower lip as a symbol of passage to adult hood in boys and was considered as an act of purification for girls. People undergo piercing for different reasons — spiritual, self-expression, aesthetic value, sexual pleasure and to conform to their cultural identity or to rebel against it.[1] Popular sites of body piercing include ears, eyebrows, lips, nose, navel, penis, scrotum, labia, and tongue.[2] The growing popularity of intraoral piercing involves the insertion of jewellery into the oral soft tissues including the lips, cheeks, frenum, and tongue.[3] This case report highlights a complication of oral piercing wherein the dorsal surface of tongue healed over the piercing embedding the barbell without patient's knowledge.
An 18-year-old male presented to the dental office 1 year after having his tongue pierced. The procedure was done by an expert followed by uneventful healing. Three weeks prior the jewellery was not visible and the patient assumed he had swallowed the jewellery. Thereafter he experienced mild pain and swelling leading to restriction of movement of the tongue and alteration in speech. Clinical examination revealed a swollen tongue with a piercing mark on the dorsal surface. The ventral surface showed a clearly visible metal barbell traversing the tongue [Figure 1]. Intraoral radiograph of the tongue showed the barbell embedded inside the tongue [Figure 2]. Manual digital pressure was used from the ventral surface to define the site of the previous piercing and allow removal of the jewellery [Figure 3]. The infection was treated with amoxycillin 500 mg tid and paracetamol for pain relief.
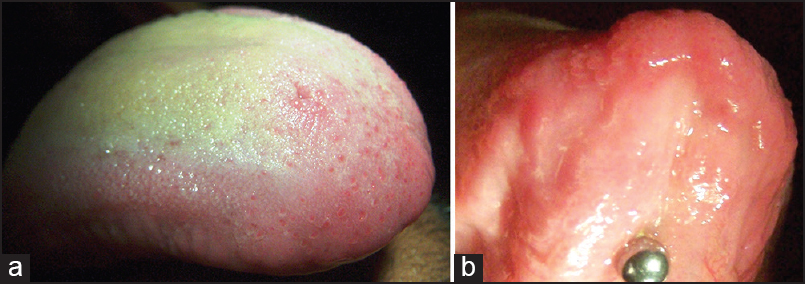
- (a) Preoperative view — dorsum of tongue. (b) Preoperative view showing ventral surface of tongue
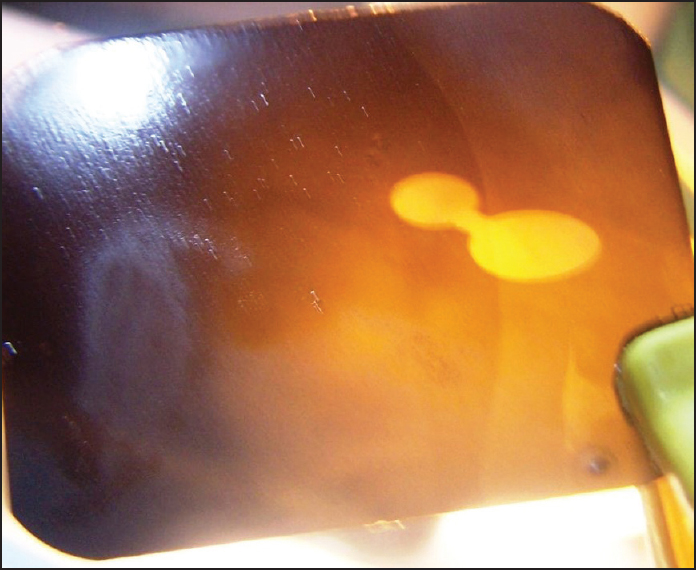
- Intraoral radiograph of tongue showing a foreign object
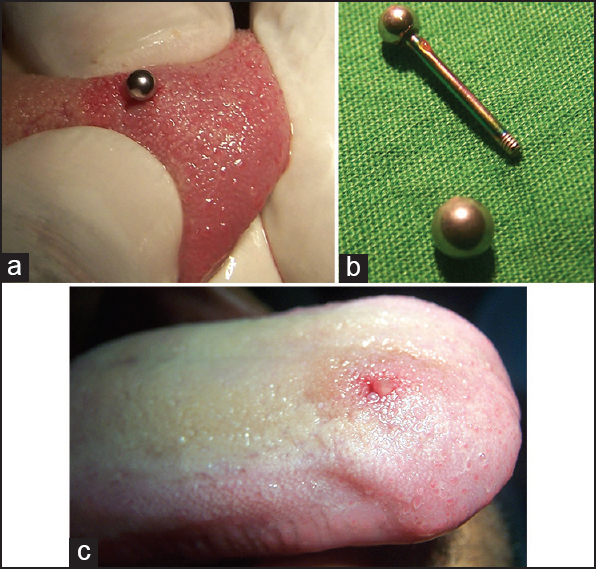
- (a) Manual digital pressure used and the foreign object is retrieved. (b) Removed oral jewellery. (c) Immediate post operative view of dorsum of tongue
The incidence of multiple extreme piercing to make a fashion statement is mostly seen in young people below the age of 30, especially in the male population. It is important to underline that tongue region is at highest risk for hemorrhagic complications, because of the extensive vascularisation in the tongue. Several case reports have documented dental complications such as chipping or cracking of teeth, abrasions, localised gingival recession, hyper salivation, calculus build up on the lingual surface of the barbell and interference with swallowing, mastication and speech.[4] Apart from damage to the dentition, tongue piercings is also associated with life-threatening systemic complications. Perkins et al. reported a case of Ludwig's angina developed secondary to tongue piercing.[5] Piercing of oral sites carries potential high risk of infection and transmission of organisms such as HIV, hepatitis B and C, herpes simplex virus and Epstein-Barr virus.[4]
Thrill-seeking behaviour and peer pressure maybe the driving force for extreme piercing. Growing enthusiasm of such body art makes it imperative that dermatosurgeons, oral surgeons and dental professionals go hand in hand in guiding individuals about the risks they are exposed to after intraoral piercing and to manage post-piercing complications.
REFERENCES
- Multiple dental fractures following tongue barbell placemen: A case report. Dent Traumatol. 2006;22:41-3.
- [Google Scholar]
- Tongue piercing and associated oral and dental complications. Endod Dent Traumatol. 2000;16:232-7.
- [Google Scholar]
- A complication of tongue piercing. A case report and review of the literature. Br Dent J. 2003;194:551-2.
- [Google Scholar]
- Tongue piercing and its adverse effects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:274-6.
- [Google Scholar]




