
Translate this page into:
A Study of the Outcome of Primary Excision and Closure Technique in the Management of Lip Leukoderma in 30 Patients
Address for correspondence: Dr. Shilpa Kanthur, No. 52, OPD, B Block, Victoria Hospital, BMCRI, Bengaluru, Karnataka, India. E-mail: Shilpakvinod@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Lips being one of the graceful cosmetic units of the face, any disfigurement, including depigmentation, can be embarrassing, psychologically distressing, and socially stigmatizing. Even with the evolution of various surgical modalities, none of the techniques ensure 100% pigmentation with a good cosmetic appearance. With this background, this study was undertaken to study the efficacy of the technique—primary excision and closure in treatment of lip leukoderma (LL).
Aims:
To study the efficacy, cosmetic outcome, and recurrence following primary excision and closure technique in the management of LL.
Settings and Design:
A prospective single-center open-label uncontrolled study.
Materials and Methods:
Thirty patients with LL involving inner margin of the lower lip and those who fulfilled inclusion and exclusion criteria were included in the study. After obtaining consent and physician fitness, patients were posted for primary excision and closure of the vitiliginous area of the lip. Patients were followed up at the immediate postoperative period and 6 months later. Patient satisfaction scale was done by asking the patient to grade the response between one and ten.
Statistical Analysis Used:
Mean and percentiles.
Results:
Out of 30 patients, 29 patients achieved complete clearance that was cosmetically acceptable. Only one patient showed recurrence at the end of 6 months. Average patient satisfaction scale showed an average of 9.66.
Conclusions:
Primary excision and closure technique is one of the safe, inexpensive modality in the management of LL involving the inner margin of the lip with immediate result.
Keywords
Lip leukoderma
lip vitiligo
primary excision and closure
stability

INTRODUCTION
Vitiligo is a common condition characterized by hypopigmented and/or depigmented spots on the skin and mucous membrane that can have a major impact on the quality of life of patients. In the present era, we have a wide spectrum of many effective treatments for vitiligo; however, on an average, and considering all affected anatomical locations, the best repigmentation rates do not reach figures beyond 70%, with acral regions and lesions with leukotrichia being the most difficult to repigment.[1] Vitiliginous lesions occurring on sites such as lips, acral areas, nipples, and genitals are particularly resistant to medical treatment. This has led to the evolution of various surgical modalities to treat recalcitrant stable lesions.[2] In such scenarios, a white patch involving facial areas such as lips and eyelids can have a profound effect on the quality of life of vitiligo patients, many of whom feel distressed and stigmatized by their condition.[3] Njoo et al. recommended a surgical technique as first line treatment of segmental vitiligo and vitiligo involving lips and finger tips.[4] The choice of surgical treatment depends on the type of vitiligo, extent and site of the lesions, and the availability of equipment and expertise of the treating surgeon. Various grafting methods have been described, including tissue grafts and cellular grafts.[2] Each technique has its own advantages and disadvantages. The basic principle of tissue and cellular grafts is to transplant autologous melanocytes from pigmented normal skin to the vitiliginous area to achieve cosmetically acceptable pigmentation. Apart from tissue and cellular grafts, other techniques such as micropigmentaion, advancement flaps, and primary excision and closure are additionally described in the management of lip vitiligo. This article highlights the outcome of primary excision and closure in the management of lip vitiligo.
MATERIALS AND METHODS
Thirty patients having stable vitiligo for at least 6 months, involving the inner margin of the lower lip were enrolled for the study. Vitiliginous area involving only less than upper one-third of the total height of the lower lip [Figure 1] were considered for surgery to avoid the inversion of the lips. Proper history regarding the onset, progression of the disease, involvement of other areas, associated autoimmune conditions, keloidal tendency, habit of lip biting, herpes labialis, and smoking were taken. Patients were examined to look for signs of unstability such as koebnerization. Patients with a history of new lesions, increase in the size of existing lesions in the last 6 months or showing koebnerization, signs of infection at the operation site, patients with keloidal tendency were excluded from the study.
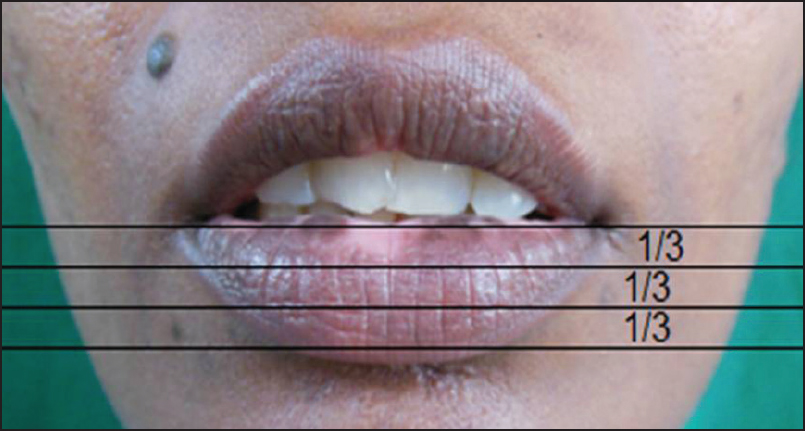
- Showing a vitiliginous area involving upper 1/3 of lower lip that can be excised and closed without distortion of the lip
After proper counseling, complete preoperative evaluation was done and physician fitness was taken. Informed written consent and preprocedure photographs were taken prior to surgery.
Borders of the vitiliginous area were marked before anesthesia. Anesthesia was achieved by giving intraoral mental nerve block. With the patient in a semirecumbent position, 2.5 mL of 2% lignocaine with adrenaline was injected into the gingivolabial sulcus between the first and the second premolar teeth on both sides. This technique ensures complete anesthesia of the lower lip.
Incision was put along the premarked lines and the vitiliginous area was excised. A sponge holding forceps was used to achieve homeostasis during the procedure. Wound edges were approximated with 3-0 chromic catgut with running sutures. After applying topical antibiotic, paraffin dressing, followed by sterile gauze dressing was done [Figure 2a–f]. Dressing was secured with adhesive bandage as shown in the Figure 2f, which prevents slipping.
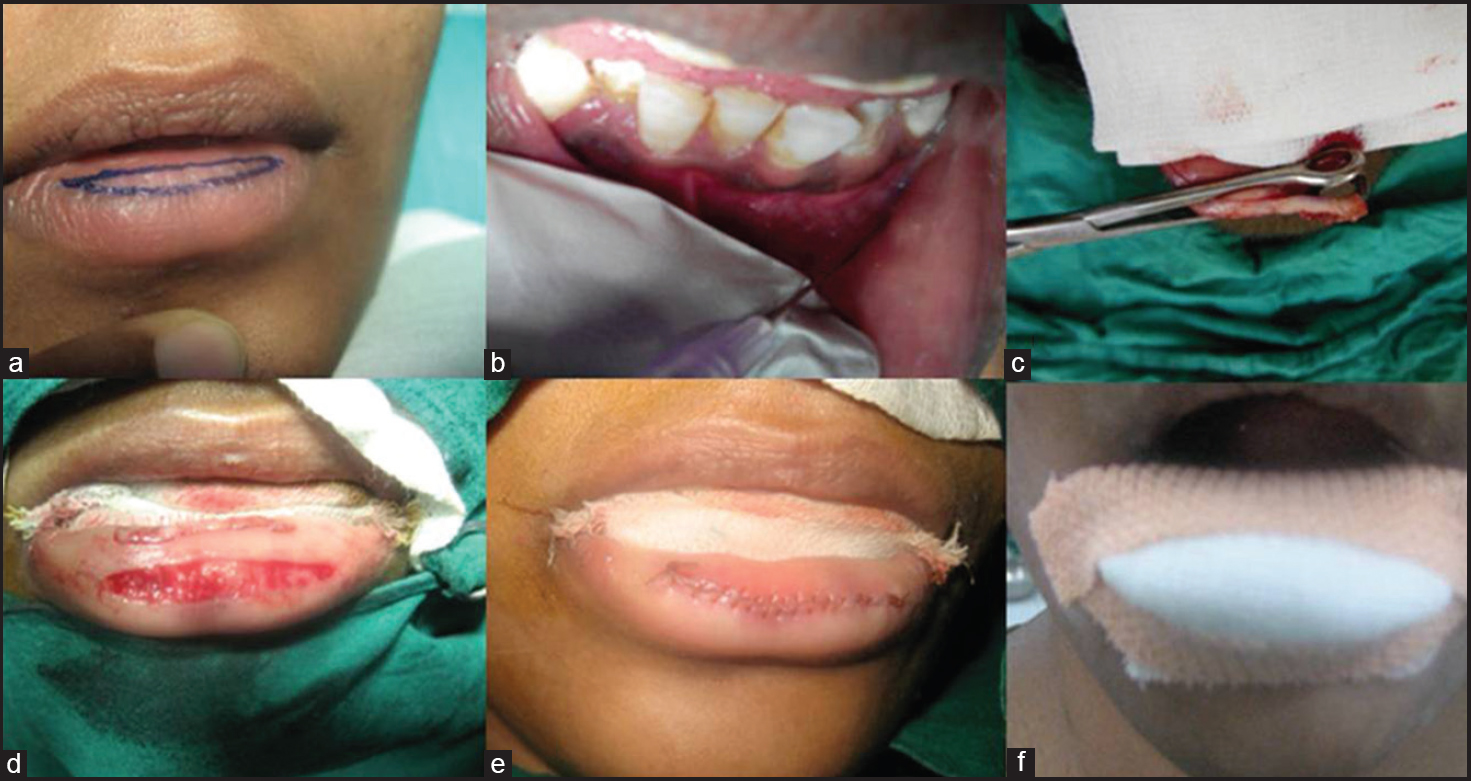
- Intraoperative procedure: (a) Marking vitiliginous area, (b) Mental nerve block, (c) Achieving homeostasis with forceps, (d) Vitiliginous area excised, (e) Wound closed with 3-0 catgut with running sutures, (f) Dressing done
Postoperatively, patients were put on antibiotics and analgesics. They were advised a soft diet and to avoid vigorous chewing for 3 days. They were reviewed after 3 days, 7 days, and 6 months, respectively. After 3 days dressing was removed and the patient was advised to apply topical antibiotic cream for 1 week. Suture material got absorbed in 7 to 10 days. At the end of 6 months, the patients were asked to grade the response between one and ten, with one implicating least and ten excellent satisfactory scale. Operative site was examined for any recurrence, persistence, scarring, pigmentary changes, alteration or distortion in lip architecture.
RESULTS
The mean age group in the study was 29 years. Among 30 patients, 18 were males and 12 were females. Nineteen patients had vitiligo limited only to the lip. Rest of the 11 patients had vitiligo elsewhere on the body for which eight patients had undergone other surgical modalities such as miniature punch grafting (PSG) and follicular unit extraction and were on phototherapy in the form of narrow band ultraviolet B (UVB) therapy. Three patients had not received any kind of treatment. However, none of the patients were on any systemic immunosuppressant. Six patients gave a history of the habit of lip biting. History of smoking was present in eight patients.
The average period of stability was 18 months, between 8 months and 4 years. All the patients tolerated the procedure well. Swelling of the lips with mild discomfort was noted in the immediate postoperative period that persisted for 3-4 days. All the patients showed good improvement with immediate results. At 6 months follow-up, 29 patients had excellent results with no recurrence. Only one patient who had stable disease for 4 years before surgery showed recurrence of vitiliginous area.
Patient satisfactory scale analysis showed the score ranging between 8 and 10, the average being 9.66.
DISCUSSION
Lip leukoderma (LL) is more common in dark races and may occur in 20% of patients with vitiligo.[5] It can occur with cutaneous vitiligo as well as an isolated mucosal lesion. Local inflammatory factors may play a role. Precipitating conditions include smoking, gingivitis, recurrent herpes simplex, discoid lupus erythematosus, etc. More commonly, vitiligo involves the vermillion and spares the wet labial mucosa. An inverse distribution that is sparing of vermillion and band-like involvement of the labial mucosa can occur uncommonly, which may be associated with prolonged gingival inflammation. Another uncommon variant is the involvement of only the lateral most part of the lip [Figure 3].[6] The condition is often resistant to medical management mainly due to the absence of hair follicles. Melanocyte transfer, therefore, by any surgical procedure may repigment this condition.[7]

- Three patterns of lip leukoderma—(a) Involving vermilion, (b) Inverse pattern, (c) Predominantly involving angles of mouth
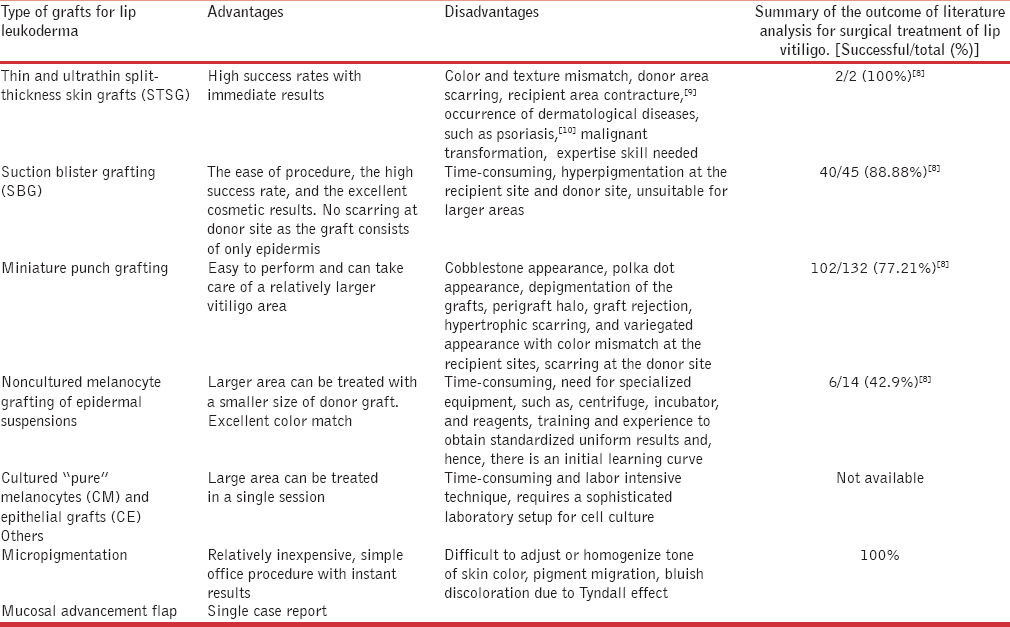
The following transplantation procedures have been found to be commonly used for lip vitiligo [Table 1]. Additionally, the table shows the advantages, disadvantages, and outcome of various surgical methods.
Tissue grafts
Thin and ultrathin split-thickness skin grafts
Thin or ultrathin split-thickness grafts are most successful in the treatment of vitiligo of the lips, with 100% results in literature analysis done by Gupta et al.[8] But very few cases treated with this procedure have been reported in the literature because of certain drawbacks[910] given in Table 1.
Suction blister grafting
The aim of this method is to transfer active melanocytes to the depigmented region through blister induction and separation of the epidermis and transferring it to the vitiligo region.[11] As with any other technique, it has its own advantages and disadvantages given in Table 1.
According to a literature analysis done by Gupta et al., this technique has shown good results in 40 out of 45 cases (88.88%) of lip vitiligo.[8]
Miniature punch grafting
The procedure involves the transfer of circular pieces or punches of skin tissue from the donor area into similar shaped pits that are made on the recipient skin. The advantages and disadvantages[12] of this technique has been given in Table 1.
According to a literature analysis done by Gupta et al., this technique has shown good results in 102 out of 132 cases (77.21%) of lip vitiligo.[8]
In a study by Malakar, graft uptake was achieved in 98 cases (91%), whereas all the grafts were rejected in eight cases of herpes-labialis-induced LL (HILL). Two cases (1.5%) showed depigmentation of grafts. Cobblestoning was the most common complication and was observed in 32 cases (30%). Complete repigmentation was achieved in 78 cases (72%).[7]
A comparative study done by Babu et al. between PSG versus suction blister epidermal grafting (SBEG) in the treatment of stable lip vitiligo with eight patients in each group showed two patients had repigmentation of 50-75%, one had 75-90%, and three had 90-100% in the recipient site in the PSG group. In the SBEG group, one patient had repigmentation of 50-75%, three had 75-90%, and two had 90-100%.[13]
Cellular grafts
Noncultured melanocyte grafting epidermal suspensions
Autologous noncultured melanocyte-keratinocyte transplantation (also called basal cell rich, noncultured melanocyte suspension) is the most commonly reported as well as the simplest cellular grafting technique. The basic principle is to separate the basal cells and the melanocytes by trypsinization, and prepare a suspension that is applied on the dermabraded lesional skin or mucous membrane.[14] In a study conducted by Guerra et al., though this technique had shown average percentage of repigmentation rate of 77% over all areas, the study concluded that cultured epidermal grafts could be considered a real therapeutic surgical alternative for “stable” vitiligo, but not for lip-tip vitiligo.[15]
In literature analysis by Gupta et al., noncultured melanocyte-keratinocyte transplantation for the lips has shown satisfactory results in only 6 out of 14 patients (42.9%).[8]
Cultured “pure” melanocytes and epithelial grafts (CE)
Cultured melanocyte (CM) technique is time-consuming and labor intensive technique that requires a sophisticated laboratory setup for cell culture, though it can cover vitiliginous areas 100 times the donor area. It is, therefore, suitable to cover large body surface areas.[16] Literature on its efficacy and cost-effectiveness in the management of lip vitiligo is unavailable.
Others
Micropigmentation
It is a method in which pigments are injected directly into the dermis and lasts for months to years at a time. Iron oxide is the most common pigment used. Various chemicals used and the respective colors produced include black, camel yellow, light and dark brown (iron oxide), white (titanium dioxide), yellow (cadmium sulfide), and red (mercuric sulfide/cinnabar with cadmium sulfide).[17] This is useful particularly for lesions on the scalp, eyebrows, and lips, which are naturally pigmented. Though it is a relatively inexpensive and simple office procedure with instant results, it has certain disadvantages as well [Table 1]. Though this technique gives immediate and 100% results, its utility is limited by these drawbacks.
Mucosal advancement flap[18]
It is a novel procedure practiced as a therapeutic modality to cover excised lip lesions of varied etiology. This principle has been applied to treat lip vitiligo. There is a single case report of this technique in the management of lip vitiligo.
Surgical excision and primary closure[19]
This technique described by Sacchidanand et al. is one of the surgical procedures that can be used for the treatment of LL.
In our study, this technique has given excellent immediate results in all patients. Cosmetic outcome was very good as well [Figures 4–7]. Recurrence was noted only in one patient at the end of the 6 month follow-up. This procedure gives immediate results as compared to other surgical modalities that take a longer time to repigment. There is no uncertainty of results like in other procedures. There is no risk of displacement of grafts as in skin grafting methods, no cobblestoning, as in miniature PSG, no postoperative hyperpigmentation as in suction blister grafting, no special equipment are required and there is no need to maintain the patient on a liquid diet. The wound heals fast as well.

- (a) Lip leukoderma (lateral involvement), (b and c) After primary excision and closure

- (a) Lip leukoderma with unsightly bluish discoloration due to micropigmentation, (b) Same patient with primary excision and closure for lower lip vitiligo

- (a) Lip leukoderma (inverse pattern), (b and c) After primary excision and closure

- (a) Lip leukoderma, (b) After primary excision and closure
But the following disadvantages of the technique include: It cannot be performed for a larger area involving the vermilion, it may lead to alteration in the shape of the lip if there is excessive tension on the wound edges, and short follow-up period of 6 months is a drawback of the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tissue grafts in vitiligo surgery - past, present, and future. Indian J Dermatol. 2009;54:150-8.
- [Google Scholar]
- The development of guidelines for the treatment of vitiligo. Clinical Epidemiology Unit of the Istituto Dermopatico dell’Immacolata-Istituto di Recovero e Cura a Carattere Scientifico (IDI-IRCCS) and the Archives of Dermatology. Arch Dermatol. 1999;135:1514-21.
- [Google Scholar]
- Dipigmentation of hair and mucous membrane. In: Hann SK, Nordlund JJ, eds. Vitiligo (1st ed). Oxford: Blackwell Science; 2002. p. :76-80.
- [Google Scholar]
- Surgical management of lip vitiligo. In: Gupta S, Narang T, Olsson MJ, Ortonne JP, eds. Surgical Management of Vitiligo (1st ed). Delhi: Blackwell Publishing; 2007. p. :211-9.
- [Google Scholar]
- Surgical management of vitiligo and other leukodermas: Evidence-based practice guidelines. In: Gupta S, Narang T, Olsson MJ, Ortonne JP, eds. Surgical Management of Vitiligo (1st ed). Delhi: Blackwell Publishing; 2007. p. :69-79.
- [Google Scholar]
- The use of processed allograft dermal matrix for intraoral resurfacing: An alternative to split-thickness skin grafts. Arch Otolaryngol Head Neck Surg. 1998;124:1201-4.
- [Google Scholar]
- Dermal psoriasis involving an oral split-skin graft. Case report. Aust Dent J. 1998;43:321-3.
- [Google Scholar]
- Repigmentation of leukoderma by autologous epidermal grafting. J Dermatol Surg Oncol. 1984;10:136-44.
- [Google Scholar]
- Grafting in vitiligo: How to get better results and how to avoid complications. J Cutan Aesthet Surg. 2013;6:83-9.
- [Google Scholar]
- Punch grafting versus suction blister epidermal grafting in the treatment of stable lip vitiligo. Dermatol Surg. 2008;34:166-78.
- [Google Scholar]
- Treatment of “stable” vitiligo by timed surgery and transplantation of cultured epidermal autografts. Arch Dermatol. 2000;136:1380-9.
- [Google Scholar]
- A comparative study of efficacy of cultured versus non cultured melanocyte transfer in the management of stable vitiligo. Med J Armed Forces India. 2014;70:26-31.
- [Google Scholar]
- Mucosal advancement flap: An innovative surgical technique for treatment of lip vitiligo. Dermatol Surg. 2013;39:334-7.
- [Google Scholar]
- Surgical excision and primary closure for the treatment of lip vitiligo. J Cutan Aesthet Surg. 2011;4:216-7.
- [Google Scholar]




