
Translate this page into:
An Unusual Presentation of Piloleiomyoma
Address for correspondence: Dr. Aditya Kumar Bubna, Department of Dermatology, Sri Ramachandra University, Porur, Chennai - 600 116, Tamil Nadu, India. E-mail: zimbabwa21@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Piloleiomyomas are benign tumors arising from the arrector pili muscle of hair follicles. They usually present between the second and third decade of life.[1] Predominantly, these tumors are located over the trunk and extremities, range in size between 2 mm to 2 cm, and are painful and firm in consistency.[2]
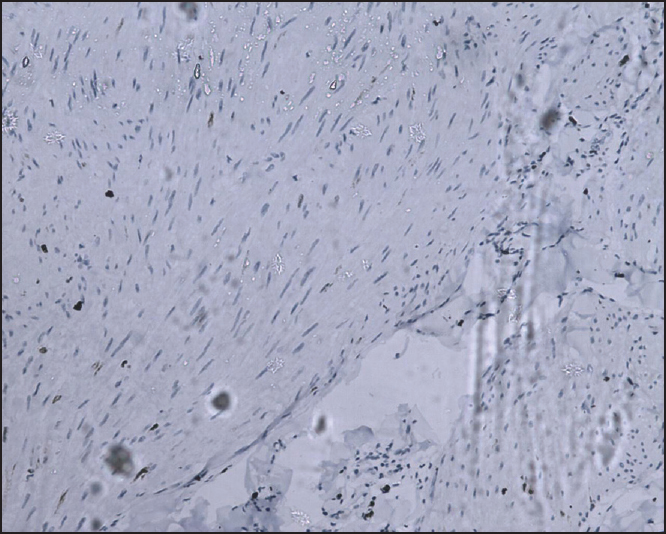
Our patient was a 45-year-old gentleman who presented to the Department of Dermatology with chief complaints of nodular skin lesions over the left upper arm since the past 7 years. It began as a singular, small pea-sized lesion that gradually progressed to reach the current status. Lesions were asymptomatic, the major cause of concern being cosmetic disfigurement. Clinical examination revealed the presence of around 15 nodules over the left upper arm ranging from 5 cm × 4 cm × 6 cm to 1 cm × 2 cm × 2 cm in size [Figure 1]. They were nontender on palpation and demonstrated a soft-rubbery consistency. A skin biopsy from one of the nodules revealed a normal epidermis, with poorly circumscribed interlacing smooth muscle fibers located in the dermis [Figure 2]. On higher magnification these fibers were individually composed of eosinophilic cytoplasm with an elongated eel-like nuclei [Figure 3]. Immunohistochemistry for smooth muscle actin (SMA) was positive [Figure 4]. However, S100 and Ki67 staining were negative [Figures 5 and 6]. With these findings a diagnosis of cutaneous leiomyoma was made. The patient was counselled regarding his treatment. However, he declined any surgical intervention.

- Fleshy rubbery clustered nodules over the left upper arm
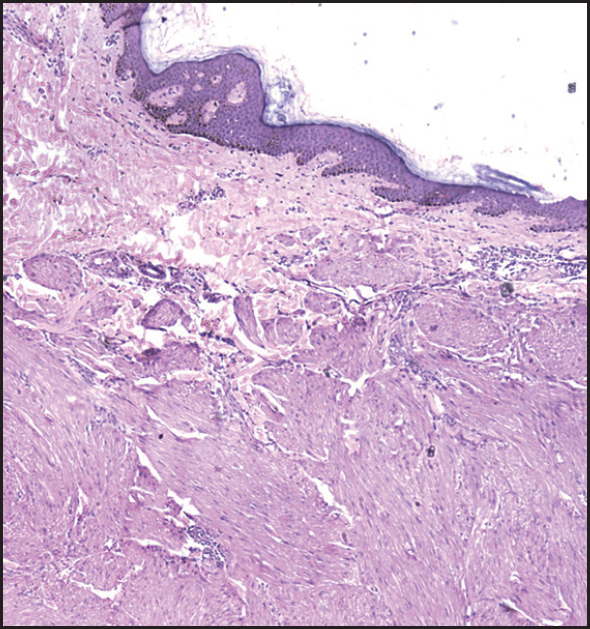
- Scanner view of an H&E skin biopsy specimen from one of the nodules showing a normal epidermis with poorly circumscribed interlacing smooth muscle fibers in the dermis
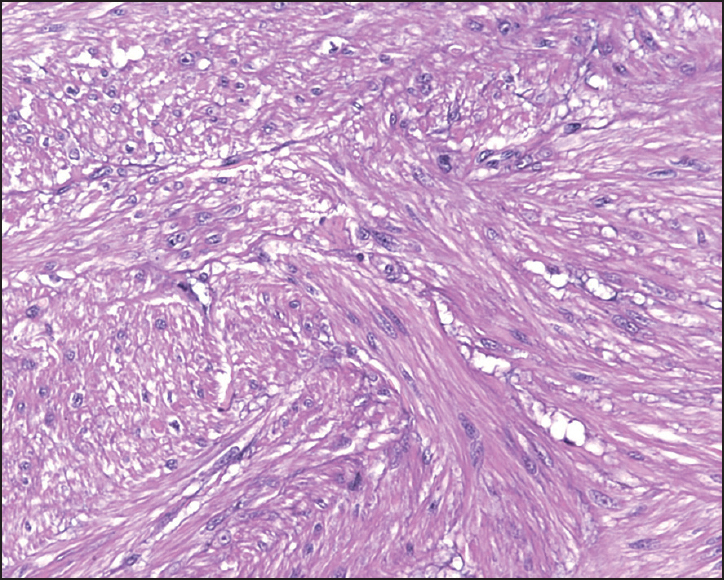
- Individual smooth muscle fibers demonstrating an eosinophilic cytoplasm and an elongated eel-like nuclei (H and E 20×)
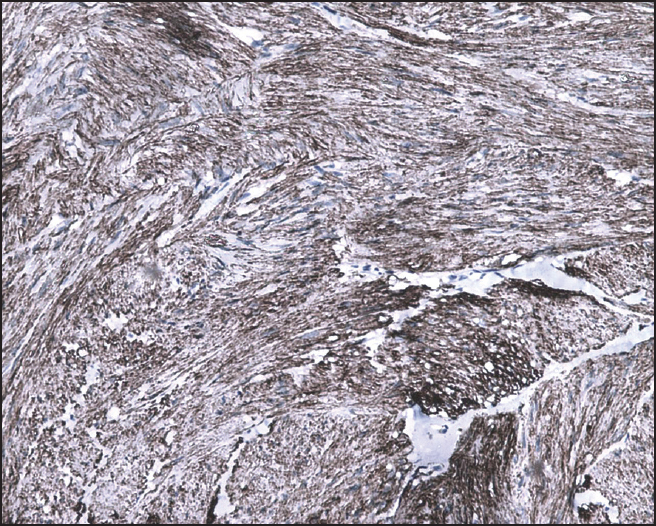
- Immunohistochemistry positive for SMA
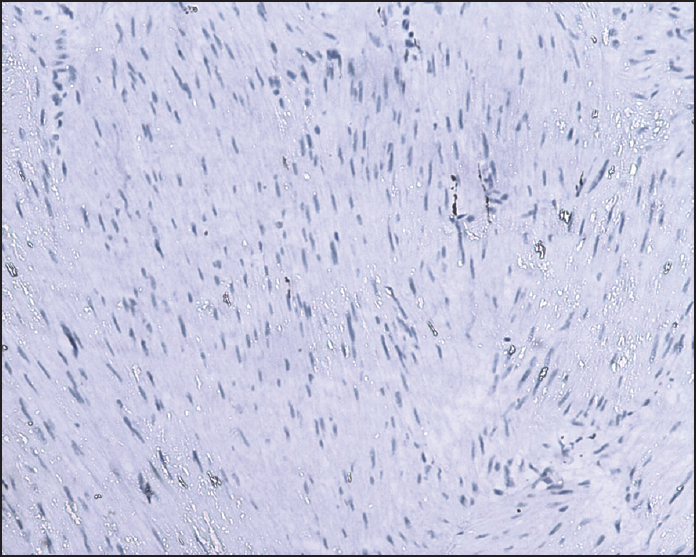
- Immunohistochemistry negative for S 100
- Immunohistochemistry negative for Ki67
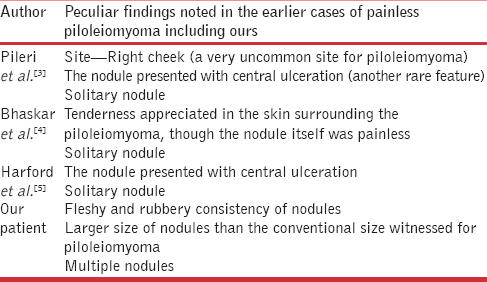
Painless piloleiomyoma has not been a commonly encountered entity. A thorough literature search revealed only three case reports manifesting the painless display of piloleiomyoma.[345] Interestingly, in all these three cases piloleiomyoma presented as a solitary nodule, a feature dissimilar to our case, which presented as multiple nodules. Other salient features of the previous three cases including ours have been summarized in Table 1.
With evaluation of our case and study of previous reported cases of painless piloleiomyoma, the authors would like to highlight that the painless quality of these lesions are not only a rarity, but painless leiomyomas are usually accompanied by other atypical findings that need vigilant identification. As far as treatment is concerned, surgical excision is the only available therapeutic modality at present, and given the high recurrence rate after surgery, this line of therapeutic intervention would not be practical with existent multiple nodules. To conclude, further exploration in the emergence of a concrete therapeutic modality in this setting is needed, as this domain still remains vastly unexplored.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Atypical leiomyoma: An unusual variant of cutaneous pilar leiomyoma. Dermatol Online J. 2009;15:6.
- [Google Scholar]
- Cutaneous pilar leiomyoma: Clinicopathologic analysis of 53 lesions in 45 patients. Am J Dermatopathol. 1997;19:2-9.
- [Google Scholar]
- Atypical piloleiomyoma of the face presenting with central ulceration. Dermatol Reports. 2011;3:e50.
- [Google Scholar]
- An atypical piloleiomyoma presenting as a nonhealing ulcerated nodule. Cutis. 1996;57:168-70.
- [Google Scholar]




