
Translate this page into:
A Solitary Firm Nodule on the Palm
Address for correspondence: Dr. Arun C Inamadar, Department of Dermatology, Venereology and Leprosy, SBMP Medical College, Hospital and Research Center, BLDE University, Vijayapur - 586 103, Karnataka, India. E-mail: aruninamadar@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
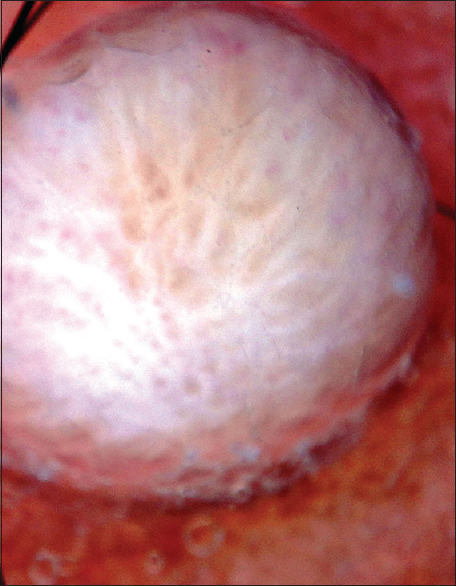
A 60-year-old female presented with a gradually enlarging asymptomatic lesion on the right palm from the past 8 months [Figure 1]. The general health of the patient was otherwise unremarkable and she denied any history of preceding trauma. Clinical examination revealed a 1 cm × 1 cm firm, non-tender dome-shaped nodule on the right palm near the base of index finger surrounded by a rim of thick raised skin [Figure 2]. The entire lesion was excised under local anesthesia and hematoxylin and eosin examination revealed a hyperkeratotic epidermis with subjacent dense fibrocollagenous mass with numerous interspersed blood vessels [Figure 3].

- A 1 cm × 1 cm, dome shaped nodule near the base of index finger on right palm

- Close-up view of the lesion showing a nodule with a peripheral collarette of raised skin
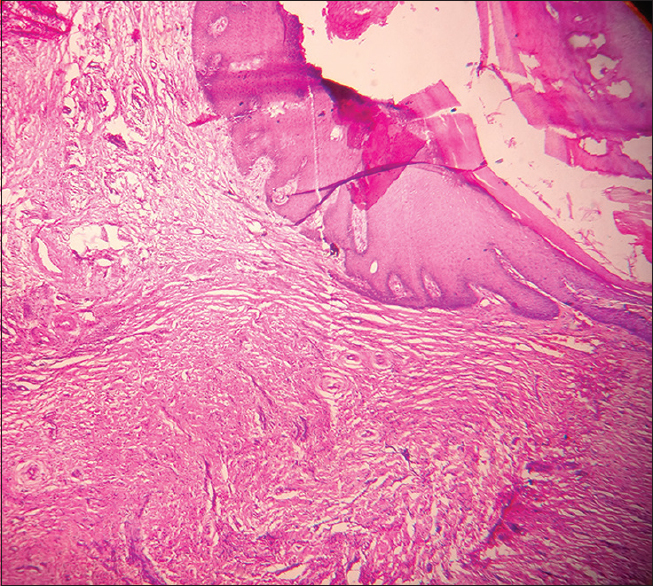
- Acanthotic epidermis overlying dense fibrocollagenous mass in the reticular dermis with numerous interspersed blood vessels (H and E, ×100)
What is your diagnosis?
ANSWER
Quiz - Answer: Acral fibrokeratoma.
Acral fibrokeratoma is an acquired benign tumor often seen in adults. The tumor is often solitary and frequently occurs on the digits and hence usually referred to as acquired digital fibrokeratoma. The characteristic feature of the tumor is the moat-like collarette of hyperkeratotic skin that surrounds a central firm papule or nodule that may have a warty surface. Histologically, increased vertically oriented collagen fibers together with increased blood vessels in the dermis are noted underlying a hyperkeratotic and acanthotic epidermis.[1] Dermoscopy usually shows a central homogenous pale yellowish area reflecting the central increased dermal collagen with peripheral white scaly collarette [Figure 4].[2] Differential diagnoses include eccrine poroma, pyogenic granuloma, a rudimentary supernumerary digit, viral wart, dermatofibroma, and a cutaneous horn.[34] The first three may also have a collarette of skin surrounding the central lesion but can be differentiated histopathologically from fibrokeratoma. Acral fibrokeratoma may be almost indistinguishable clinically from a rudimentary supernumerary digit when located at the base of little finger. However, the supernumerary digit is congenital and although histologically quite similar to fibrokeratoma, presence of increased nerve bundles at the center of the lesion helps in differentiating it from fibrokeratoma. The periungal fibromas of tuberous sclerosis (Koenen tumor) should also be considered which also show the clinical and histological resemblance.[5] Simple excision is curative.[3]
- Dermoscopy under polarized light showing central pale area indicative of increased fibrocollagenous tissue with peripheral scaling
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Soft-tissue tumours and tumour-like conditions. In: Burns T, Breathnach S, Cox N, Griffiths C, eds. Rook's Textbook of Dermatology (8th ed). Oxford: Wiley-Blackwell; 2010. p. :56.1-65.62.
- [Google Scholar]
- Fibrous and fibrohistiocytic proliferations of the skin and tendons. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology (2nd ed). London: Elsevier; 2008. p. :1813-29.
- [Google Scholar]
- Histopathologic study of Koenen tumors. Are they different from acquired digital fibrokeratoma? J Am Acad Dermatol. 1988;18(2 Pt 1):369-72.
- [Google Scholar]




