
Translate this page into:
Objective Brow Height Measurements Following Pretrichial Brow Lift and Upper Lid Blepharoplasty
Address for correspondence: Dr. Adam S Hassan, 2757 Leonard St NE, Grand Rapids - 49525, MI, USA. E-mail: aahassan2@comcast.net
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
As the ptotic brow drops below the supraorbital rim, it can exacerbate dermatochalasis by pushing the adjacent skin of the upper lid further down.
Aim:
The purpose of this study was to evaluate the outcomes associated with a combined pretrichial brow lift and upper lid blepharoplasty in patients with dermatochalasis and mild to moderate brow ptosis.
Materials and Methods:
A retrospective case series of 46 patients with dermatochalasis and mild to moderate brow ptosis treated with a combined, bilateral pretrichial brow lift and upper lid blepharoplasty from January 2008 to December 2011. Main outcome measures included measurements of brow lift at 3 months post-operatively, complications encountered, patient satisfaction and surgeon satisfaction.
Results:
Outcomes from 46 patients were evaluated. The mean brow lift was 1.85 mm at the lateral canthus, 1.54 mm at the lateral limbus, 1.31 mm at the mid-pupil, and 1.07 mm at the medial limbus. Brow lift at the lateral canthus was significantly more elevated than at the medial limbus (P < 0.001). Minor complications were encountered in seven of 46 patients (15.2%). Mean patient satisfaction score was 3.20 and surgeon satisfaction 3.24 (max = 4, very satisfied).
Conclusions:
The modified pretrichial brow lift offered effective lateral lift that complements an upper lid blepharoplasty. This technique was met with a high degree of patient and surgeon satisfaction, and had a minimal complication profile.
Keywords
Brow ptosis
pretrichial brow lift
temporal brow lift

INTRODUCTION
The upper third of the face, of which the eyelid-brow complex is of primary importance, is integral to both facial expression and beauty.[12] With age, gravity and loss of elastic tissue support can lead to progressive descent of the brows and lateral hooding of the upper lids. As the ptotic brow drops below the supraorbital rim, it can exacerbate dermatochalasis by pushing the adjacent skin of the upper lid further down. Not only does this result in a tired or angry appearance, but it may also produce functional visual impairment.[345678] When a patient has excess tissue and heaviness in the upper eyelids, a problem-specific approach is imperative to selecting the most appropriate therapeutic modality.[34]
Failure to recognise brow ptosis as a contributing factor prior to blepharoplasty can lead to worsening of the brow ptosis and/or over-resection of skin in the lateral half of the upper eyelid.[348] Over-resection of this lateral eyelid skin may subsequently result in corneal exposure and lagophthalmos.[910] Instead, a brow lift procedure can be used to restore proper brow position, allowing for re-suspension of the upper lid complex and a more conservative removal of upper eyelid skin during blepharoplasty.[38] While upper lid blepharoplasty technique is fairly standard, several brow-lift techniques exist: Coronal, endoscopic, mid-forehead, direct, trans-blepharoplasty, and pretrichial brow lifts.[123456789101112] While each technique has its advantages and disadvantages, no single technique or combination is clearly superior.[313]
In patients seeking functional improvement of vision secondary to dermatochalasis and mild to moderate brow ptosis, selecting a targeted approach that is technically easy and quick, yet cosmetically acceptable is of interest. The authors present a series of such patients that were treated with a modified pretrichial brow lift combined with upper lid blepharoplasty. The purpose of this study was to evaluate the outcomes associated with the aforementioned technique.
MATERIALS AND METHODS
In this retrospective case series, surgical logs were reviewed for all patients who underwent combined bilateral upper lid blepharoplasty and modified pretrichial brow lift at the senior authors' practice between January 2008 and December 2011. Inclusion criteria included all patients with both pre-operative and 3-month post-operative photos. Those missing either a pre-operative or post-operative photo were excluded. Patients only receiving unilateral brow lift were also excluded. Charts were reviewed for patient demographics and the following outcome variables: Measurements of brow lift at 3 months, complications, patient satisfaction and surgeon satisfaction.
Brow measurements were retrospectively analyzed by comparing non-standardised photos taken in office with a Canon EOS 30D digital camera. To allow for comparison, images were standardised for measurements using Adobe Photoshop imaging software. By scaling the horizontal corneal diameter to 11 mm, measurements of pre- and post-operative brow position were made possible. All patients' horizontal corneal diameters were clearly visible thus allowing for scaling to be performed on all patients. Brow height was measured from a horizontal line through the centre of the pupil to the top of the eyebrow at four set points: Medial limbus, centre of the pupil, lateral limbus, and the lateral canthus [see Figure 1]. In order to minimise inter-observer variability, the same grader (MM) scaled all patient photographs and measured pre- and post-brow height measurements. Given that this was not a comparative study, the grader was not blinded to the procedure when taking measurements. Pre- and post-operative brow positions were compared with a Paired T-test (2-tail).

- Brow height measurements. Brow height was measured from a horizontal line through the centre of the pupil to the top of the eyebrow at four set points: Medial limbus (ML), middle of the pupil (MP), lateral limbus (LL), and the lateral canthus (LC). Pupil resized and standardised at 11 mm
Charts were retrospectively reviewed for mention of potential complications which included but were not limited to alopecia, scar visibility, asymmetry, dimpling, paraesthesia, haematoma, skin necrosis, posterior displacement of hairline, shortened forehead, suture migration, blepharospasms, lagophthalmos and need for surgical revision. Subjective patient and doctor satisfaction were also evaluated by grading the chart on a scale from one to four (1 = very dissatisfied, 2 = somewhat dissatisfied, 3 = satisfied, 4 = very satisfied).
Surgical technique
The face is prepped and draped in the usual sterile fashion for eye plastic surgery under monitored sedation. The upper eyelid skin to be excised is outlined with a skin marker, and the area to be excised is infiltrated with a local anaesthetic solution of 2% lidocaine with epinephrine 1:100,000.
Next, ellipses of skin, typically measuring 3 cm × 1 cm are outlined bilaterally in the pretrichial skin of the temporal forehead [see Figure 2]. Local anaesthetic consisting of 2% lidocaine with 1: 100,000 epinephrine mixed equally with 0.5% Marcaine anaesthetic is injected beneath the markings. The ellipses of pretrichial skin are then excised with a #15 blade, extending into the subcutaneous fat. Haemostasis is ensured. The skin and subcutaneous tissues inferior to the excised skin are undermined with tenotomy scissors down to the superior orbital rim. This dissection is carried out in a subcutaneous plane, taking care to avoid neurovascular bundles. A 4-0 PDS suture is used to suspend the lower, undermined flap to the periosteum immediately deep to the upper edge of the elliptical excision. This is repeated with three to four interrupted stitches, to provide an effective “lift” of the brow. The subcutaneous tissue is closed with 5-0 monocryl suture. The skin is then closed with a running 5-0 Prolene suture. This is repeated on the contralateral side. Following the brow lift, the blepharoplasty was performed.
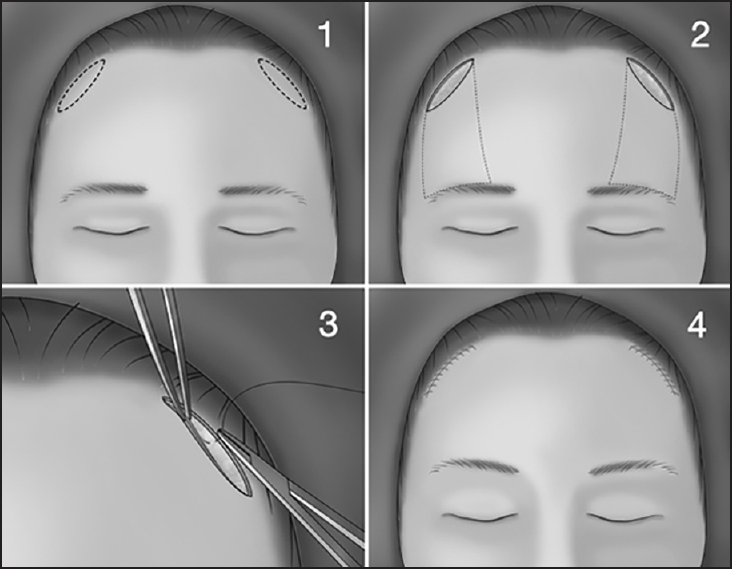
- Surgical technique
When performing the upper eyelid blepharoplasty, care was taken not to create lagophthalmos. The tissue removal was performed so that greater than 2.0 cm of upper eyelid skin was left in each patient's upper eyelid postoperatively. A small strip of orbicularis oculi muscle was removed just above the lid crease. No pre-tarsal or sub-brow orbicularis muscle was removed. With this limited resection of upper eyelid muscle, it was felt to be unlikely to contribute to any elevation of the brow.
RESULTS
During the study period, 46 patients met inclusion criteria. All 46 patients were white women with a mean age of 64 years old (range 51-84). Of these patients, only two were smokers. The mean brow lift at the four selected points was 1.85 ± 2.22 mm at the lateral canthus, 1.54 ± 2.19 mm at the lateral limbus, 1.31 ± 2.02 mm at the mid-pupil, and 1.07 ± 1.83 mm at the medial limbus. Brow lift at the lateral canthus was significantly more elevated than at the medial limbus (1.85 mm vs 1.07 mm respectively, P< 0.001). Brow lift at the lateral limbus was also significantly more elevated than at the mid-pupil (1.54 mm vs 1.31 mm, respectively, P = 0.005). See Figure 3 for sample pre and post-operative photos.
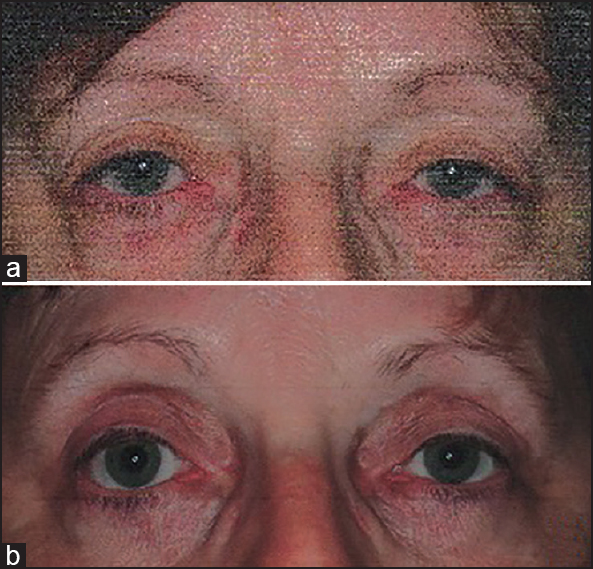
- (a) Pre-operative photo (b) 7 months post-operative photos following bilateral modified pretrichial brow lift and blepharoplasty
Post-operative complications were seen in seven of the 46 study patients. These included a case of transient forehead paraesthesia, three cases of infection of the incision that healed with a short course of oral antibiotics, and three cases of incision opening requiring a minor procedure performed in the office to reclose. None of the complications required a return trip to the operating room. Mean patient satisfaction score was 3.20, while the mean surgeon satisfaction score was 3.24.
DISCUSSION
In this study, we found that the modified pretrichial brow lift was a useful adjunct to an upper lid blepharoplasty. The 1.85 mm of lateral lift safely complemented the blepharoplasty in correcting the visual field obstruction without increasing the potential for lagophthalmos. Moreover, the targeted lateral lift allows for the correction of the “angry” appearance of the eyelid-brow complex. Our results were in agreement with the approximately 2-mm brow elevation reported by McGuire and Gladstone in their description of a novel pretrichial brow lift.[1] While there are conflicting reports on whether or not upper lid blepharoplasty lowers the brow,[1415] our technique demonstrated an ability to significantly elevate the brow despite being combined with a blepharoplasty. Additionally, this technique was met with a high degree of patient and surgeon satisfaction, and had a minimal complication profile. This modified pretrichial brow lift offers certain advantages over conventional brow lift techniques.
Compared to the coronal or full pretrichial lift that has long contiguous incisions extending the width of the scalp, this modified pretrichial technique offers smaller and less invasive incisions. By utilising two temporal incisions immediately anterior to the hairline, there is less risk of alopecia and it leaves two smaller scars more ammendable to camouflaging with hairstyling than seen with a direct brow lift.[1234] These features in combination with the low complication rate offer advantages similar to an endoscopic approach. Furthermore, the modified pretrichial brow lift does not suffer from the disadvantages of an endoscope such as less direct surgical exposure, need for retraining, or the expense of additional equipment.[12] Another approach that offers similar appeal in this patient population is the trans-blepharoplasty brow lifts; however, much of the literature either only describes the technique or focuses on subjective patient/doctor satisfaction outcomes without focus on anthropometric measurements.[111216] In short, this type of modified pretrichial brow lift offers a minimally invasive, open technique that is both safe and effective while providing a good cosmetic result in the appropriately selected patient.[1]
A major contributing factor to the patient and surgeon satisfaction with the modified pretrichial brow lift was the careful selection of our patient population. Given our patients roughly experienced 1.0 to 1.85 mm of lift to the overall brow, this technique should be reserved for patients with mild to moderate brow ptosis. What is more, discussion of a patient's cosmetic expectations remains an important component of the pre-operative exam. Men may not find the preferential lateral lift to be cosmetically acceptable, as most men prefer the more masculine flat brow configuration. On the other hand, the ideal female brow aesthetic features a brow that peaks between the lateral limbus and lateral canthus.[4] With regards to concealing post-operative scars, bitemporal incisions may become conspicuous in men with receding hairlines. By selecting older women with deep forehead rhytids and a definitive or thick anterior hairline, post-operative scars can easily be hidden.
It is important to note some limitations of this study. First, we cannot comment on the longevity of the brow lift, as our study had limited follow-up and brow measurements were only measured once at the 3-month follow-up visit. This was likely because patients were both highly satisfied and free of complications, and did not require return office visits. Also, despite standardisation of photos by scaling the iris to 11mm, this method inherently introduces error into measuring differences between pre-operative and post-operative photos. Other limitations included the retrospective nature and lack of a comparison group.
CONCLUSIONS
In closing, the pretrichial brow lift is a safe, effective and technically easy procedure to accompany upper lid blepharoplasty in the appropriate patient. Furthermore, the use of anthropometric measurements should be routinely incorporated into future brow lift studies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Novel pretrichial browlift technique and review of methods and complications. Dermatol Surg. 2009;35:1390-405.
- [Google Scholar]
- Contemporary management of the aging brow and forehead. Laryngoscope. 1997;107:710-5.
- [Google Scholar]
- Brow ptosis correction: A comparison of five techniques. Facial Plast Surg. 2010;26:186-92.
- [Google Scholar]
- Endoscopic pretrichial brow lift: Surgical indications, technique and outcomes. Ophthal Plast Reconstr Surg. 2004;20:268-73.
- [Google Scholar]
- Brow lift for the correction of visual field impairment. Aesthet Surg J. 2008;28:512-7.
- [Google Scholar]
- Current concepts in aesthetic upper blepharoplasty. Plast Reconstr Surg. 2004;113:32-42e.
- [Google Scholar]
- Browpexy through the upper lid (BUL): A new technique of lifting the brow with a standard blepharoplasty incision. Aesthet Surg J. 2011;31:163-9.
- [Google Scholar]
- Transblepharoplasty brow suspension: An expanded role. Ann Plast Surg. 2008;60:2-5.
- [Google Scholar]
- Small incision subperiosteal and trans-blepharoplasty forehead and browlift. J Plast Reconstr Aesthet Surg. 2007;60:195-200.
- [Google Scholar]
- Brow lift in facial rejuvenation: A systematic literature review of open versus endoscopic techniques. Plast Reconstr Surg. 2011;128:335-41e.
- [Google Scholar]
- Changes in eyebrow position and shape with aging. Plast Reconstr Surg. 2009;124:1296-301.
- [Google Scholar]
- The forehead lift: Endoscopic versus coronal approaches. Aesthetic Plast Surg. 2001;25:35-9.
- [Google Scholar]




