
Translate this page into:
Tattoo Practices in North-East India: A Hospital-based Cross-sectional Study
Address for correspondence: Dr. Binod Kumar Thakur, Dermatology and STD, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong - 793 018, Meghalaya, India. E-mail: binod.k.thakur@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Tattooing has become increasingly popular, particularly among young people. However, little is known about the tattoo practices in North-East India.
Objectives:
The primary objective of this study was to know the reasons and motivations of tattoo application and tattoo removal in individuals asking for tattoo removal. The secondary objective was to identify the demography, methods and safety of tattoo practices in these tattooed individuals.
Materials and Methods:
A hospital-based cross-sectional study was carried out in 212 consecutive individuals seeking tattoo removal. Chi-square and Fisher's exact tests were performed for intergroup comparisons.
Results:
There were 178 (84%) males and 34 (16%) females. The mean ± standard deviation (SD) age of individuals seeking tattoo removal was 21.8 ± 4 years. The mean ± SD age of doing tattoo was 15.8 ± 3 years. Most individuals possessed an amateur tattoo (94.3%), 4.2% a professional one and 1.4% had a combination. Sewing needle was the most common instrument used for making tattoos in 51.4%. The individuals made their tattoos in an unsterile manner in 49.1%. The most common reason for doing tattoo was for fashion in 87.7%. The participants wanted tattoo removal to qualify for jobs, especially in armed forces in 49.5% and due to regret in 21.7%. Black was the most preferred colour in 37.3% followed by green in 28.3%. The fabric ink was the choice of ink in maximum number of individuals, i.e. 93.9%.
Limitations:
It was a hospital-based study done only on individuals seeking tattoo removal. It needs caution to generalise the findings in population. In addition, there may be recall bias in the participants.
Conclusion:
The tattoo was done mostly below 18 years of age in a crude unsterile way. The individuals had poor risk perceptions about various infections and complications of tattooing. There is an urgent need to caution and educate the youngsters and school-going children about safe tattooing and consequences of tattooing.
Keywords
Body image
scarring
tattooing

INTRODUCTION
Tattooing has been practised all over the globe since ancient times. There is a rich cultural heritage of tattooing in the tribes of North-East India. Tattooing was more of a social issue than a personal choice in early days. The girls of ‘Apatani tribes’ of Arunachal Pradesh were forced to do tattoo on their face [Figure 1]. The head-hunting ‘Konyak tribe’ of Nagaland used to tattoo their faces. The right to be tattooed was earned on the battlefield and if a man or clan brought back human trophies, then the victors were tattooed by the Queen. With the modernisation and urbanisation of North-East India over the decades, the tattoo culture has shifted significantly. Tattoos are becoming popular among the youngsters mostly as a fashion statement or improvement of body image. The motivation and reasons for requesting tattoo removal have been investigated in Western countries.[123456] There is no study about the present-day tattoo practices in North-East India and the information is limited regarding the motivations and reasons for requesting tattoo removal in India. The primary objective of the present study was to know the reasons and motivations of tattoo application and tattoo removal in individuals asking for tattoo removal. The secondary objective was to identify the demography, methods and safety of tattoo practice in these tattooed individuals.

- Tattoo on the forehead, nose and chin in a female of ‘Apatani’ tribe
MATERIALS AND METHODS
A cross-sectional hospital-based study was carried out at a tertiary care centre which caters patients from the entire North-East India. The individuals who attended the Dermatology Out-patient Department for tattoo removal from July 2014 to September 2015 were included in the study. A sample of 212 consecutive patients was enrolled with convenient sampling. A questionnaire was developed to collect the data regarding age, gender, methods of tattooing, whether amateur or professional tattoo, types of instrument used for tattooing, sterilisation of instruments, colour, numbers, site of tattoo, ink used, age of doing tattoo and reasons for doing and removing tattoo. Data were collected after obtaining informed consent from all the participants through face-to-face interview. All patients were subjected to HbsAg, anti-hepatitis C virus and human immunodeficiency virus (HIV) tests. The study was approved by the Institutional Ethics Committee.
Statistical analysis
The collected data were analysed using SPSS version 22 (IBM SPSS Statistics, Version 22.0. Armonk, IBM Corp., NY, USA). Chi-square and Fisher's exact tests were performed for intergroup comparisons. P < 0.05 was considered statistically significant. The confidence interval (CI) for proportions was calculated by PEDro (Physiotherapy Evidence Database Confidence Interval Calculator, 2013, www.pedro.fhs.usyd.edu.au).
RESULTS
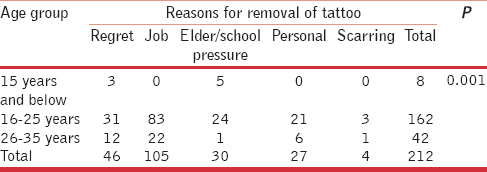
In total, 212 participants were enrolled in the study. There were 178 (84%) males and 34 (16%) females. The median duration between tattooing and seeking removal of tattoo was 5 years (range 0–18). The mean ± standard deviation (SD) age of individuals seeking tattoo removal was 21.8 ± 4 years (range: 13–35). Seventy-six percent of these individuals were in the age group of 16–25 years. The mean ± SD age of doing tattoo was 15.8 ± 3 years (range: 8–26). The tattoo was done below 16 years of age in 49.1% of the participants. The most common reason for doing tattoo was for fashion in 87.7% (95% CI 82.6–91.4) of the individuals. Fun and peer pressure were the other reasons for doing tattoo in 6.6% and 4.7% of the participants, respectively. The participants wanted tattoo removal to qualify for job application, particularly in armed forces in 49.5% (95% CI 42.8–56.2) and due to regret in 21.7% (95% CI 16.6–27.7) of the participants. The association between reasons for removal of tattoo and the age group for seeking tattoo removal was statistically significant [Table 1; P = 0.001].
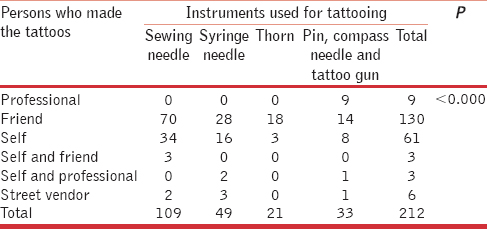
Most individuals possessed an amateur tattoo in 94.3%, professional one in 4.2% and combination in 1.4%. The tattoo was done mostly by their friends in 61.3% (95% CI 54.6–67.6) and self in 28.8% (95% CI 23.1–35.2) of the participants. Sewing needle was the most common instrument used for making tattoos in 51.4% (95% CI 44.7–58) followed by syringe needle in 23.1% (95% CI 17.9–29.2) of the participants. A statistically significant association was noted between the use of different instruments for doing tattoo and the persons who made their tattoos [Table 2; P < 0.001].
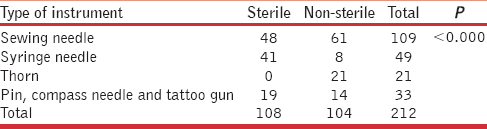
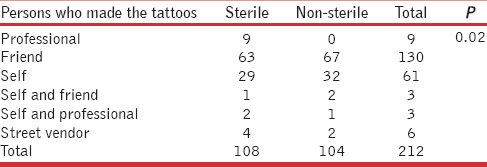
The individuals made their tattoos in an unsterile manner in 49.1% (95% CI 42.4–55.7). There was statistically significant association between sterility of the procedure with type of instruments used for tattooing [Table 3; P < 0.001] and the persons who made the tattoos [Table 4; P = 0.024].
Black was the most preferred colour in 37.3% (95% CI, 31–43.9) followed by green in 28.3% (95% CI, 22.6–34.7) of the participants. However, the preferred colour among female participants was green which was seen in 35.3% (95% CI, 21.4–52) followed by blue in 29.4% (95% CI, 16.8–46.1) of the participants. The fabric ink was the choice of ink in the maximum number of individuals, i.e., 93.9% (95% CI, 89.7–96.3).
Majority favoured upper limbs for tattooing their skin, i.e., 76.4% (95% CI 70.2–81.6). Multiple tattoos were seen in 75% (95% CI 68.7–80.3) of the participants and the mean number of tattoos was four (range: 1–26).
A very few tattoo complications were observed in the study. Only one person had hepatitis C virus infection and three individuals had tattoo granulomas in red tattoo [Figure 2]. Four individuals (1.9%) developed hypertrophic scarring following tattooing, for which they wanted tattoo removal, whereas five individuals developed scarring on tattoo area in an attempt to remove the tattoo by putting acids and lime [Figure 3].

- Tattoo granuloma due to red ink

- Scarring on tattoo area in self-attempt to remove the tattoo
DISCUSSION
The present study has highlighted many important issues regarding the present-day tattoo practices in North-East India. The maximum number of tattoos was amateur tattoos done by mostly unqualified persons. Around 50% of the individuals got their tattoo done when they were as school-going children. This may be attributed to their emotional immaturity and influence of fashion. Varma and Lanigan[1] reported in their study that the mean age of tattooing is 16 years, mostly amateur tattoos (54%) and the most common cause of tattoo application is fashion. Latreille et al.[2] found that 44% got their tattoo before 18 years, 39.1% had amateur tattoo and the common reasons for application of tattoo were imitation or influence of entourage (24%), aesthetic reasons (21%) and sentimental reasons (20%). However, in our study, 94.3% of the tattoos are amateur which is quite high in comparison to other studies, and the most common reason for tattooing was fashion (87.7%). Since 1969, it has been illegal to tattoo individuals <18 years in the United Kingdom.[7] However, 71% of the patients had done their tattoo before the age of consent as reported by Varma and Lanigan.[1] Preventive education targeted at school children emphasising scarring, disease transmission, complications, permanency, possible effects on employment, social stereotypes and cost of removal may reduce under-age tattooing.[18] In our country, there is no law and regulation restricting an individual to get tattoo done at an early age.
In a recently published study, the author found that only 17.6% of the individuals placed their tattoo outside a tattoo parlour.[9] Whereas in our study, 95.8% of the individuals placed their tattoos outside a tattoo parlour. Hence, there was no professionalism in doing tattoo to these persons. The tattoo was done in an unsterile way in 49.1% of the participants. The commonly available instruments such as sewing needle, thorns, compass and table pins were used for tattooing. Fifty-six percent of the sewing needle users did not sterilise the needle and 16.3% of the syringe needle users shared their needles while tattooing. The statistical significant association noted between sterility of tattooing and instruments used for tattooing is due to the inherent nature of few instruments used for tattooing to be unsterile, for example, thorns, table pins, etc. However, only one person had hepatitis C virus infection and the test for HIV and hepatitis B was negative in all the other individuals. Tattooing at very early age by friends and self may be the reason for extremely low prevalence of blood-borne infections in our study participants. In addition, the reason for no HIV positivity could be due to a very low prevalence of HIV (0.06%) in Meghalaya (NACO, India HIV estimations, 2015, technical report).
Tattoo inks are commonly made up of a mixture of small organic pigments, water and isopropyl alcohol.[10] However, in our study sample, 93.9% of the participants preferred to use conventional colour paints and fabric inks for tattooing. Tattoo inks can contain polycyclic aromatic hydrocarbons at a range of concentrations, which are reported to be carcinogenic, mutagenic and could pose other health risks to the skin.[11] In a study done in Western Australian high school adolescents, the authors found that the tattoo was done with crude implements in a majority of the individuals.[12] Lack of awareness and poor risk perceptions among our study participants enabled them to use painting colour for tattooing.
Laumann and Derick conducted a random survey of 500 men and women and found a prevalence of tattooing in 26% of males and 22% of females in the United States and 17% of them considered tattoo removal.[13] The prevalence of tattooed individuals in India is not known. However, there has been a remarkable increase in the patients seeking removal of tattoos for various reasons. The reasons for laser tattoo removal in a study were improvement of self-esteem (48 patients), followed by social reasons (24 patients), family pressure (13 patients), improving potential for employment (12 patients) and a change of partner (4 patients).[1] The three major reasons mentioned for laser tattoo removal in another study were ‘Never been pleased with tattoo (21%)’, ‘Embarrassment or shame (20%)’ and ‘Professional reasons (17%)’.[2] The reasons for tattoo removal in our sample were quite different from the Western studies. To be eligible for armed force jobs was the most common reason for tattoo removal (49.5%), followed by regret (21.7%), elder or school pressure (14.2%), personal (12.7%) and unsightly appearance such as hypertrophic scarring in tattoo (1.9%). The significant association noted between the age group of tattoo removal and reasons for tattoo removal suggests that the reason for tattoo removal varies with the age group. For example, 39.2% of the individuals who wanted tattoo removal to be eligible for job were in the age group of 16–25 years, 10.4% in the age group of 26–35 years and 0% in the age group below 15 years. Many individuals also used crude methods in desperate need for tattoo removal to join the armed forces resulting in complications such as scarring. The mean age for seeking tattoo removal is also lower in our study than that reported in other studies.[12] This is because the cohort in our study were mostly young people (13–35 years).
The limitation of the present study is that it was a hospital-based cross-sectional study done on individuals seeking tattoo removal. Hence, its needs caution to generalise the findings in population due to the selection bias of including only those individuals who came for tattoo removal. Moreover, there may be recall bias in the participants. However, this is the first Indian study on tattoo practices. In addition, the tattooed individuals asking for tattoo removal in our study are representatives of the random sample of tattooed individuals of the population.
CONCLUSION
It has been noted from the present study that the tattoo was done mostly before 18 years of age in a crude unsterile way. The participants at the time of tattooing were ignorant that many professions such as Indian armed forces do not allow recruitment of tattooed individuals. The individuals had poor risk perceptions about various infections and complications of tattooing. The participants also did not know that laser tattoo removal is a prolonged procedure which needs multiple sittings and all colours cannot be removed completely. We recommend increasing the awareness and educating the youngsters and school-going children about safe tattooing and the consequences of tattooing. As a long-term measure, we suggest the regulation of tattooing by government legislation so that it is done with strict hygiene and minors are prevented from tattooing.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Reasons for requesting laser removal of unwanted tattoos. Br J Dermatol. 1999;140:483-5.
- [Google Scholar]
- Decorative tattoos and reasons for their removal: A prospective study in 151 adults living in South of France. J Eur Acad Dermatol Venereol. 2011;25:181-7.
- [Google Scholar]
- Motivation for contemporary tattoo removal: A shift in identity. Arch Dermatol. 2008;144:879-84.
- [Google Scholar]
- Complications of tattoos and tattoo removal: Stop and think before you ink. J Cutan Aesthet Surg. 2015;8:30-6.
- [Google Scholar]
- The demographics and rates of tattoo complications, regret, and unsafe tattooing practices: A cross-sectional study. Dermatol Surg. 2015;41:1283-9.
- [Google Scholar]
- Tattoo ink nanoparticles in skin tissue and fibroblasts. Beilstein J Nanotechnol. 2015;6:1183-91.
- [Google Scholar]
- Tattoo inks contain polycyclic aromatic hydrocarbons that additionally generate deleterious singlet oxygen. Exp Dermatol. 2010;19:e275-81.
- [Google Scholar]
- Amateur tattooing practices and beliefs among high school adolescents. J Adolesc Health. 1996;19:420-5.
- [Google Scholar]
- Tattoos and body piercings in the United States: A national data set. J Am Acad Dermatol. 2006;55:413-21.
- [Google Scholar]




