
Translate this page into:
Onychomatricoma: A Case Report with 5-year Follow-up
Address for correspondence: Prof. Cleide Eiko Ishida, Rua Carlos Góis, 375 - Sala 401, Rio de Janeiro 22440-040, Brazil. E-mail: cleide-ishida@uol.com.br
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The authors present a case of onychomatricoma, a rare benign tumour of the nail matrix, first described by Baran and Kint in 1992. The lesion appeared on the proximal nail fold, covering half the nail of the second left finger. The nail was thickened and yellowish with longitudinal melanonychia. It was surgically removed with very satisfactory aesthetic results even after 5 years. A review on the subject is also presented.
Keywords
Adnexal tumour
nail matrix
onychomatricoma

INTRODUCTION
Onychomatricoma (OM) is a rare benign tumour of the nail matrix. This subungual tumour of unknown aetiology was described in 1992 by Baran and Kint[1] and is the only tumour in which the change of the nail plate is actively caused by the lesion. It occurs in the nail matrix and has finger-like projections embedded in the nail plate. Although described as a rare tumour, it is believed to be underdiagnosed.[1] There are clinical criteria and specific histopathological features for the diagnosis. The clinical criteria are a longitudinal band of yellow thickening of the nail plate, increased transverse curvature of the nail and splinter haemorrhages in the proximal part of the nail. Once the nail plate is removed, finger-like fibrokeratogenous projections appear through the proximal nail fold. Histologically, the tumour is characterised by filiform epithelial projections. In the centre of these projections, lacunar clefts or parakeratotic columns are visible and detachment of the thickened keratogenous zone from the matrix basaloid cells occurs. In addition, there may be longitudinal melanonychia, proximal nail swelling and splinter haemorrhages found in capillaroscopy.[2]
The authors described a Brazilian patient with OM, who was followed up 5 years. The surgical results were observed after 5 years.
CASE REPORT
A 42-year-old female patient had a 15-year history of nail deformity affecting the second finger of her left hand. Physical examination showed swelling in the proximal nail fold and its junction with the lateral nail fold and a thickened yellowish nail with longitudinal melanonychia, covering half the nail [Figure 1]. An X-ray of left hand, mycological examination and culture were requested. These examinations excluded exostosis, bone deformities and onychomycosis. Surgical excision of the altered half of the nail was performed [Figure 2]. During the surgery, filamentous, tufted material under the proximal nail was seen [Figure 3]. Immediate post-operatory aspect is shown in Figure 4. Microscopy revealed fibroepithelial projections with epithelial proliferation invaginating into cellular and fibrous stroma [Figure 5]. Multi-layered epithelial invaginations presented central clear clefts and stromal cells were CD34 positive [Figure 6]. With the clinicopathological correlation, a definitive diagnosis of OM was established.

- Clinical features of the left second finger nail

- Intraoperative aspect before excision
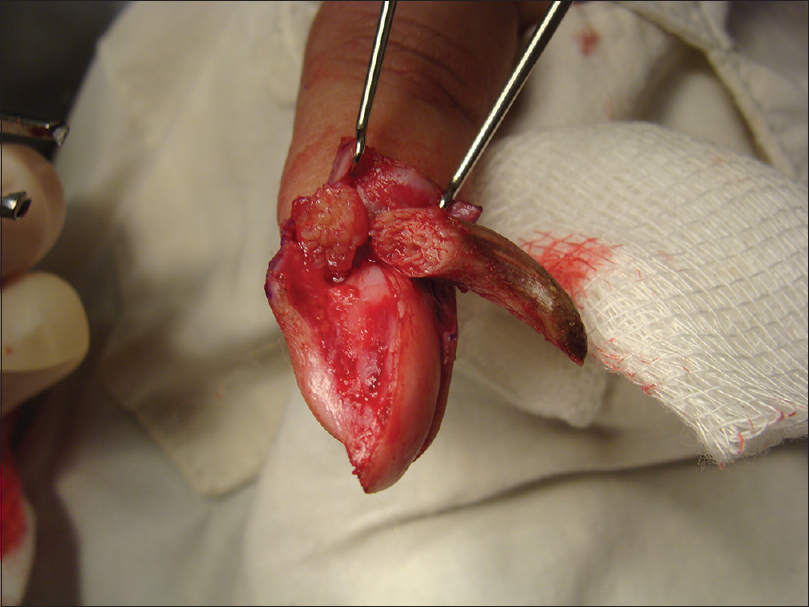
- Filamentous, tufted material under the proximal nail

- Immediate post-operatory
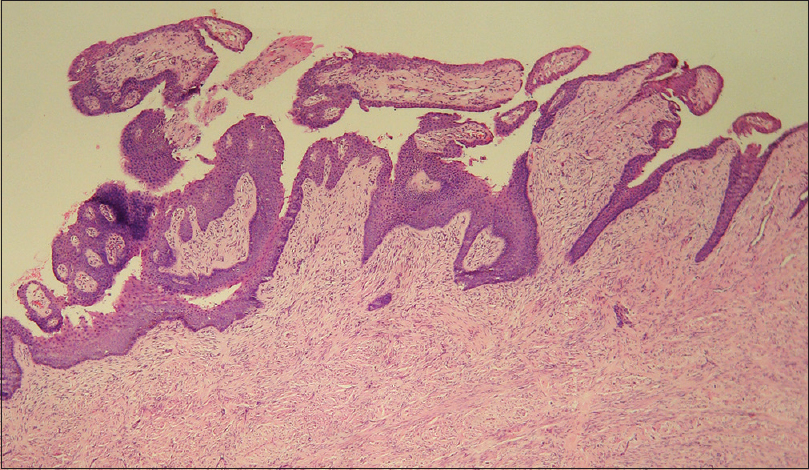
- Histopathology: Fibroepithelial invagination with the clear cleft (H and E, ×100)
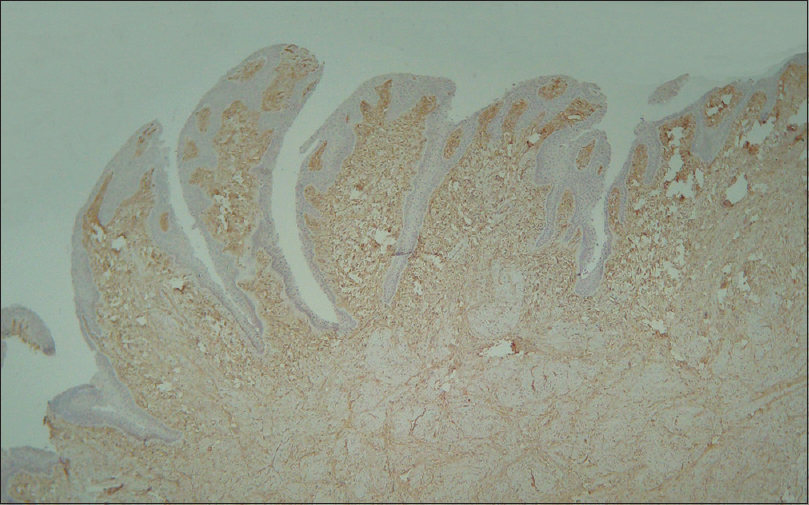
- CD34 positive stromal cells (immunostaining, ×100)
The patient evolved with no pain and no secondary infection. There was only small amount of granulation tissue. Suture was removed on the 15th post-operative day, and the patient progressed well with the growth of the entire nail. The aspect was very good after 2 months, but there was still a nail dystrophy [Figure 7]. During the 5-year follow-up, there was no recurrence or deformity and the patient is satisfied with the aesthetic post-surgical result [Figure 8].

- Two months of follow-up

- Five years of follow-up
DISCUSSION
OM, a condition described 21 years ago, has been reported in several countries.[3] Baran and Kint[Ή] first described OM and confirmed the nail matrix origin of the tumour. Other authors, however, have proposed it as a fibroproliferative hamartoma, which simulates the nail matrix histology. OM has a female: male ratio of 2.16:1; mean age of presentation is 51 years and occurs more frequently in Caucasian patients. It occurs less frequently in African Americans and exceptionally in Mexican patients. This tumour was not previously described in Brazilian patients. Its predominant location is the fingernail (75%). Predisposing factors such as trauma or onychomycosis have been suggested but its aetiology remains unknown. Pathology shows a wide histological spectrum as recently described by Perrin et al.[2] but typically consists of fibroepithelial tumour composed of a proximal pedunculated base and a distal zone with multiple projections. There is a two-layered stroma with a collagenous and fibroblastic superficial coat and a deep core with less cellularity and thicker collagen; a V-shaped hyperkeratogenous zone can be observed. Beyond the lunula, the nail plate is thickened and burrowed with cavities containing serous fluid. Immunohistochemistry for cytokeratin 5 and 14 is positive, along with K17, K6, K16, and K75 in most cases, suggesting a differentiation towards the nail bed and the nail isthmus. Recently, CD34 was also reported to be positive[4] as we found in our patient.
Complete surgical excision is the first line of treatment. Recurrence and malignant transformation have not been reported although dysplasia may be present.[4] Our patient underwent a large follow-up, which confirmed no recurrence, no dysplasia and the maintenance of good aesthetic result.
In some cases, as in the present patient, the clinical presentation may be confusing, because longitudinal melanonychia may hide the yellow hue, and the proximal nail fold may be swollen at its junction with the lateral nail fold. This swelling gives the affected nail, the texture of a cutaneous horn. In some cases, this horn is completely separated from the nail plate. Histologic examination establishes the diagnosis.[3]
Differential diagnosis for OM includes fibrokeratoma of the nail matrix, glomus tumour, squamous cell carcinoma, Bowen's disease, viral warts and ungual fibroma. Recently, a new tumour called onychocytic carcinoma (OC) was described and should be distinguished from malignant OM, which has not been described in the literature yet. OC presents small and numerous cavities in the thickened nail plate, contrasting to the broad and less numerous cavities seen in OM. Furthermore, OC does not have a fibroepithelial growth pattern, and there is absence of stroma as seen in OM.[5]
CONCLUSION
Because OM can easily mimic other ungual diseases, physicians and particularly dermatologists should be acquainted with the proper diagnosis and treatment of this adnexal tumour.
In this case report, the OM was characterised as a painless, slow-growing tumour with benign evolution. The conservative complete surgical excision appears to provide long-term resolution, and in this case report, recurrence or malignant transformation has not been observed after 5 years.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Onychomatrixoma. Filamentous tufted tumour in the matrix of a funnel-shaped nail: A new entity (report of three cases) Br J Dermatol. 1992;126:510-5.
- [Google Scholar]
- Onychomatricoma: New clinical and histological features. A review of 19 tumors. Am J Dermatopathol. 2010;32:1-8.
- [Google Scholar]
- Onychomatricoma: An infrequent nail tumor. Indian J Dermatol Venereol Leprol. 2012;78:382-3.
- [Google Scholar]




