
Translate this page into:
Utility of Laser in Lobuloplasty
Address for correspondence: Dr. Ravi Kumar Chittoria, Department of Plastic Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry - 605 006, India. E-mail: drchittoria@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Torn ear lobe surgeries need great precision due to small size, less working space and cosmetic concern. Skin incision by surgical blade causes bleeding which obscures the field and reduces precision. Control of bleeding is cumbersome for the surgeon because of the small size of lobule, lack of support and firmness. Repeated attempts for haemostasis traumatises the tissues and ultimately causes adverse effects on wound healing and cosmetic outcome. Various methods to control bleeding in ear lobule surgery are - epinephrine infiltration, electrocautery, haemostatic clips and key chain method.[1]
In medical field, laser is being used for photocoagulation of retina, in fields like dentistry and oral surgery, dermatosurgery, etc. The various lasers used include CO2 laser, Neodymium: Yttrium Aluminium Garnet (YAG), Holmium: YAG, Erbium, Chromium Doped Yttrium Scandium Gallium Garnet, Neodymium doped Yttrium Aluminium Perovskite, Gallium arsenide (diode) and Argon laser. Diode laser has advantage of relatively low cost, small size, portable and ease to use.[23]
Suter et al. compared use of CO2 laser and diode laser in the oral cavity. Both lasers showed almost equal advantages but CO2 laser was associated with high intraoperative bleeding as compared to diode laser.[4]
A 38-year-old female presented with bilateral torn ear lobule [Figure 1]. Surgical repair was planned by Pardue method. We used diode laser of the frequency of 2.5 W and a wavelength of 850 nm [Figure 2] for skin incision instead of surgical blade [Figure 3]. Rest of the procedure was completed in a usual manner. It was noticed that the bleeding was very minimal, fine suture line was obtained, both surgeon and assistant were comfortable, time taken to complete the procedure was significantly less, use of epinephrine was avoided and dose of local anaesthetic was less [Figures 4 and 5]. The wound healed completely without any complications resulting in almost invisible scar [Figure 6].

- Pre-operative photo of patient

- Picture of diode laser console and probe used for skin incision

- Intraoperative picture demonstrating laser being used for incision

- Post-operative picture showing anterior layer repair
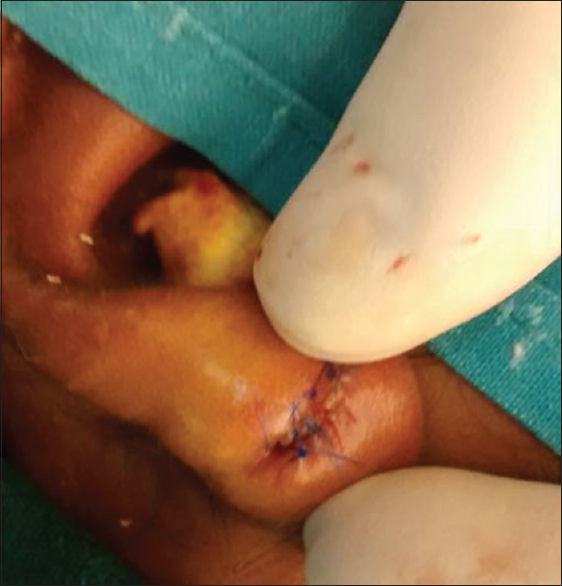
- Post-operative picture showing posterior layer repair

- Delayed picture showing good healing and almost invisible scar
We found various advantages of diode laser for skin incision-Sharp cutting edge allowing precise cut, better coagulation, instant sterilisation reduces bacterial load, less operative and anaesthesia time, minimum discomfort to surgeon and assistant, better healing, less scarring. Use of laser in lobuloplasty is not described in literature our case demonstrates successful use of diode laser in lobuloplasty.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The work was supported by Mr. Bala, who is the technical staff of laser in our institute. We are thankful to him as he helped us in understanding the technical qualities and helped us in using laser.
REFERENCES
- A Simple and Cost Effective Method for Haemostasis in Ear Lobe Repair: A Case Report. N Indian J Surg. 2015;6:83-5.
- [Google Scholar]
- 980 nm diode lasers in oral and facial practice: Current state of the science and art. Int J Med Sci. 2009;6:358-64.
- [Google Scholar]
- CO2 and diode laser for excisional biopsies of oral mucosal lesions. A pilot study evaluating clinical and histopathological parameters. Schweiz Monatsschr Zahnmed. 2010;120:664-71.
- [Google Scholar]




