
Translate this page into:
Giant Pedunculated Tumour on the Finger
Address for correspondence: Dr. Arun C Inamadar, Department of Dermatology, Venereology and Leprosy, SBMP Medical College, Hospital and Research Center, BLDE University, Bijapur - 586 103, Karnataka, India. E-mail: aruninamadar@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
A 28-year-old female presented with a large, 3 cm × 2 cm skin-coloured pedunculated growth arising from underneath the proximal nail fold of the left fourth digit [Figure 1] for the past 8 months. The lesion was non-tender, had a lobulated consistency and a smooth surface. There was no history of recurrent bleeding, either spontaneously or following trauma. Radiologic examination did not reveal any connection with the underlying bone [Figure 2]. The lesion was completely excised under local anaesthesia by exposing the base of the peduncle with a diagonal incision running from the junction of the proximal and lateral nail folds till the distal crease towards the radial side of the hand. The wound was then closed primarily with a 6–0 non-absorbable suture [Figure 3]. Clinical differential diagnoses of superficial acral fibromyxoma, lobular capillary haemangioma and acral fibrokeratoma were considered and specimen was sent for histopathological analysis. Haematoxylin and eosin analysis showed proliferation of capillaries arranged in a multilobular fashion occupying almost the entire dermis with multiple small intralobular capillaries exhibiting well-differentiated lumina with extravasation of red blood cells [Figure 4a and b]. A final diagnosis of giant lobular capillary haemangioma (pyogenic granuloma) was established.

- A 3 cm × 2 cm skin-coloured pedunculated growth arising from underneath the proximal nail fold of the left ring finger

- A plain X-ray (anterolateral and lateral views) of the left hand showed a well-defined soft tissue shadow around the tip of the ring finger without any connection with the distal phalynx
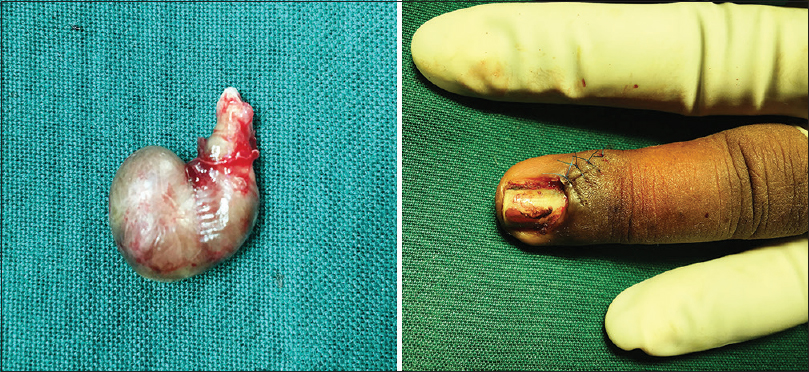
- Lesion completely excised with primary closure of the wound
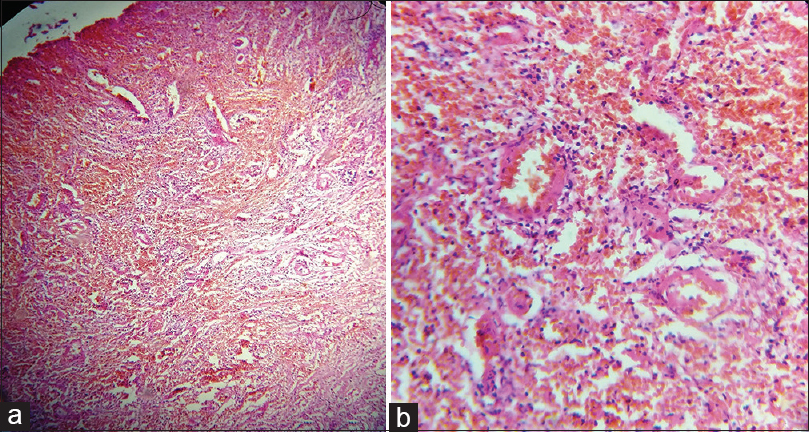
- Photomicrograph showing multiple blood vessels occupying almost the entire dermis (a) H and E, ×100. High power view showed proliferated capillaries with luminal differentiation and extravasated red blood cells (b) H and E, ×400
Lobular capillary haemangioma or pyogenic granuloma is a common acquired proliferative vascular lesion affecting the skin and mucous membranes. They appear mostly as solitary friable vascular papules that may be sessile or pedunculated. The lesions are rapidly growing and may have polypoid morphology. They do not generally enlarge beyond two centimetres but giant forms are seen.[1] A surrounding collarette of scale may be noted at the base of the lesion in most cases. Children and young adults account for most of the cases although any age, race and either gender may be affected.[2] Trauma, including burns and surgery, are often implicated in the development of pyogenic granuloma, so have been certain drugs.[3456] Association with pregnancy is a well-known entity as well when the lesions commonly involve the gingivae. The hands, forearms, face, and the lips are frequently involved. Multiple eruptive and disseminated forms associated with drugs, burns and exfoliative dermatitis have also been documented.[7] Bleeding with minimal trauma, ulceration, or development of multiple satellite lesions following traumatic or surgical destruction can complicate the existing lesions. The presence of lobular proliferation of capillary-like vessels, enmeshed in a loose stroma is the hallmark histopathological feature of lobular capillary haemangioma.[8] Treatment options include shave excision, curettage, cryosurgery and ablation with neodymium-doped yttrium aluminium garnet laser or pulsed dye lasers with the choice of treatment guided by the site and extent of the lesion.
Superficial acral fibromyxoma has a similar clinical appearance, as it almost always involves the digits, and can be seen arising from the nail bed. However, it is mostly sessile and histopathologically characterised by proliferation of spindle-shaped or stellate fibroblasts that typically express CD34, CD99, and epithelial membrane antigen.[9] Acquired digital fibrokeratoma (acral fibrokeratoma) also commonly involves the digits and usually resembles a rudimentary supernumerary digit with a characteristic moat-like collarette of skin surrounding its base. Histopathologically, it shows fibrovascular proliferation in the dermis with an overlying hyperkeratotic and acanthotic epidermis.[10] Thus lobular capillary haemangioma or pyogenic granuloma should be considered in the differential diagnosis of vascular lesions in the acral areas.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Two cases of giant pyogenic granuloma of scalp. Indian Dermatol Online J. 2013;4:292-5.
- [Google Scholar]
- Vascular neoplasm and neoplastic-like proliferations. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology (3rd ed). London: Elsevier; 2012. p. :1915-41.
- [Google Scholar]
- Multiple giant disseminated pyogenic granuloma in a burn lesion. J Burn Care Res. 2006;27:247-9.
- [Google Scholar]
- Pyogenic granuloma of the penile shaft following circumcision. Pediatr Dermatol. 2002;19:39-41.
- [Google Scholar]
- A rare side-effect of systemic isotretinoin treatment: Pyogenic granuloma. J Eur Acad Dermatol Venereol. 2003;17:609-11.
- [Google Scholar]
- Painless periungual pyogenic granulomata associated with reverse transcriptase inhibitor therapy in a patient with human immunodeficiency virus infection. Br J Dermatol. 2007;156:163-4.
- [Google Scholar]
- Disseminated pyogenic granuloma developing after an exfoliative dermatitis. J Am Acad Dermatol. 1995;32(2 Pt 1):280-2.
- [Google Scholar]
- Vascular tumors. In: Weedon D, ed. Weedon's Skin Pathology (3rd ed). Edinburgh: Churchill Livingstone Elsevier; 2010. p. :887-925.
- [Google Scholar]
- Dermal and subcutaneous tumors. In: James WD, Berger TG, Elston DM, Neuhaus IM, eds. Andrew's Diseases of the Skin Clinical Dermatology (12th ed). Philadelphia: Elsevier Saunders; 2016. p. :579-624.
- [Google Scholar]




