
Translate this page into:
Squamous Cell Carcinoma of the Nail Bed: The Great Mimicker
Address for correspondence: Dr. Swagata Arvind Tambe, Department of Dermatology, Topiwala National Medical College and BYL Nair Hospital, Mumbai, Maharashtra, India. E-mail: swagatatambe@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Squamous cell carcinoma (SCC) of the nail bed is a rare malignant subungual tumour. It can be often misdiagnosed as a chronic paronychia, onychomycosis, pyogenic granuloma, subungual wart, glomus tumour, ingrown nail, subungual exostosis, chronic osteomyelitis, traumatic dyschromia, keratoacanthoma and melanotic nevus.
Trauma, chronic paronychia, chronic solar irradiation, X-irradiation, burn scars, arsenic exposure, actinic damage, polycyclic aromatic hydrocarbons, genodermatoses, immunosuppression and human papillomavirus infection are considered to be the risk factors for the development of SCC.[1]
A 78-year-old male presented with a non-healing ulcer over the right ring finger since 2 years. He gave a history of few raw lesions on the lateral aspect of the right ring finger 2 years ago following a trauma to the right hand. He consulted a local practitioner for the same complaints and was treated with oral antibiotics, antifungals and anti-inflammatory drugs with topical antibacterial cream, with improvement over a period of 3 months.
Two 2 years back, the patient developed a persistent ulcerative lesion over right fingernail which gradually involved the left lateral aspect of the nail and did not show any improvement with medications. Since the last 7 months, there was complete destruction of the nail plate.
There were no similar lesions elsewhere on the body. The patient did not give a history of diabetes mellitus or hypertension. There was no history of tuberculosis or tuberculosis contact.
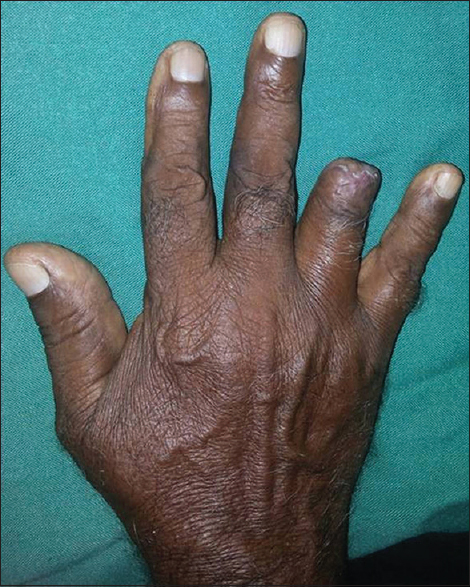
Cutaneous examination revealed an extremely tender ulcer of 1.5 cm × 0.7 cm size over the right ring finger nail bed with destruction of overlying nail plate [Figure 1a]. The ulcer extended onto both lateral and proximal nail folds. Floor of the ulcer showed granulation tissue. There was no evidence of regional lymphadenopathy. Differential diagnosis of SCC, pyoderma gangrenosum and amelanotic melanoma was considered.

- (a) Ulcer of 1.5 cm × 0.7 cm size over right ring finger nail bed with destruction of overlying nail plate. (b) X-ray of the right ring finger revealed osteophyte at the distal interphalangeal joint with widening of the trabeculae. (c) Biopsy shows epidermal proliferation with crowding of keratinocytes with atypical cells above the basal layer with formation of horn pearls. The dermis shows moderately dense lymphoplasmocytic infiltrate (H and E, ×100). (d) Biopsy shows atypical cells with altered nuclear cytoplasmic ratio with increased mitotic figures (H and E, ×400)
X-ray of the right ring finger revealed osteophyte at the distal interphalageal joint with widening of the trabeculae with no periosteal reaction or osteomyelitis [Figure 1b]. Biopsy from the edge and centre of the of the ulcer revealed epidermal proliferation with crowding of keratinocytes with altered nuclear-cytoplasmic ratio with increased mitotic figures above the basal layer with the formation of horn pearls with completely keratinising centres. The dermis showed moderately dense lymphoplasmocytic infiltrate. These features were suggestive of moderate to poorly differentiated SCC [Figure 1c and d].
The patient was subjected to complete excision of the tumour with disarticulation of the distal interphalangeal joint and amputation done up to the upper part of middle phalanx [Figure 2]. The excised tissue revealed dysplastic epidermis overlying the invasive SCC extending into the dermis and superficial subcutaneous tissue with clear margins.
- Excision of the tumour with disarticulation of the distal interphalangeal joint
The patient showed excellent result postoperatively with no recurrence even after 4 years of follow-up.
Cancers of the perionychium are relatively rare occurrences and are often related to chronic inflammation associated with trauma, infection, exposure to ultraviolet radiation, or other carcinogens. SCC is the most common tumour reported of the nail bed.
Subungual SCC is a low-grade malignant tumour with >150 cases reported in literature. It may arise from nail bed, matrix, groove or nail folds.[2] It usually affects elderly males with thumb being the most common site of involvement.[3] Early clinical manifestations are paronychia, onychomycosis, onycholysis, dyschromia of the nail plate, subungual hyperkeratosis, chronic granulation of the nail bed, ingrown nail and nail deformity.
The presence of ulceration, bleeding and nodule formation indicates its invasive nature. The nail plate changes include dystrophic nail, ingrown nail and partial or total nail loss.
Multiple digit involvement of the nail bed is a rare presentation, also known as synchronous SCC.[4] Trauma and radiation are suspected as predisposing factors in such cases.
Bone involvement is seen in >20% of patients. Nodal involvement is seen in 2% of patients.[5]
Nail biopsy is important in recurrent and persistent lesions for early diagnosis of SCC and to preserve maximal function of the hand. Treatment modalities include Mohs micrographic surgery, amputation of the distal phalanx, electrosurgery, liquid nitrogen, photodynamic therapy, radiation therapy, intra-arterial infusion with chemotherapy, imiquimod, 5-fluorouracil and lymph node dissection in case of metastasis. Amputation has the highest cure rate and is indicated in case of long-standing carcinoma or bony involvement.[6]
We present this case for rare occurrence of SCC of nail bed of ring finger as thumb being the most common site and role of histopathology in the diagnosis of SCC. A biopsy is essential in all patients with any chronic nail condition that fails to respond to conventional treatment, for a reasonable period of time as an underlying malignancy can mimic a benign nail pathology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Mohs micrographic surgery of the nail unit and squamous cell carcinoma. Dermatol Surg. 2001;27:246-51.
- [Google Scholar]
- The perionychium. In: Green DP, ed. Green's Operative Hand Surg (5th ed). Philadelphia, Pennsylvania: Elsevier Churchill Livingstone; 2005. p. :389-416.
- [Google Scholar]




