
Translate this page into:
Easing the Excision of Earlobe Keloid
Address for correspondence: Dr. Harish Prasad BR, Vitals Klinic, 8th Main, 7th Cross, BTM Layout, Bengaluru, Karnataka, India. E-mail: harish.harris@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Earlobe keloids are commonly encountered in this era where ear piercing is routine in various traditions. Various medical and surgical methods have been tried for its management. Surgically, fillet flap surgery has better acceptability worldwide. Various difficulties are faced during keloid excision, and we hereby describe few innovative modifications (use of needle, hydrodissection, pressure dressing, bolster button) using cost-effective and simple materials (needles, dynaplast, buttons) to ease the excision of keloids. These have easy adaptability and also reduce the recurrence rate of earlobe keloids.
Keywords
Buttons
earlobe keloid
fillet flap
needles

INTRODUCTION
Earlobe keloids are commonly encountered in this era of body piercing. Traditionally, they have been treated in a similar manner as to keloids elsewhere on the body with recurrences and disappointing results. Earlobe keloids are aesthetically unacceptable and are frustrating for patients and the treating doctors.
Various treatment modalities exist, including medical, surgical, radiotherapy, and combination of these. Several options for surgically treating keloid of the pinna have been used, including direct suture, healing by second intention, skin grafts, and local flaps; however, comparative studies of the different techniques have not been carried out yet.[1]
Among the surgical modality, keloid core excision or the fillet flap surgery has better acceptable results. However, there are few difficulties during the surgery [Table 1], and we herein describe few innovative ideas to address them one by one.
INNOVATIONS
1. Reducing tissue handling
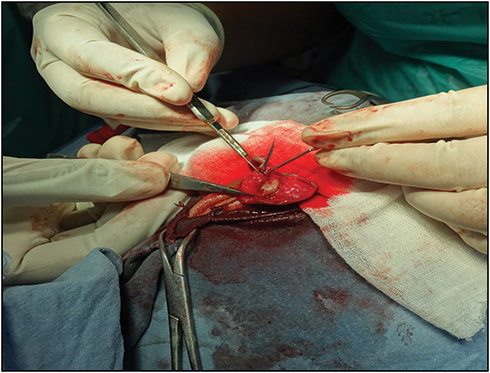
After planning and execution of a flap, the keloid tissue under the flap is carefully excised preventing its damage. Excision of keloid tissue is a challenging task as the operative field is smaller and use of requisite instruments is hampered by the lack of space. Hence, we used a 24-G needle and inserted it into the bulky part of the keloid tissue, which helps us to easily hold, elevate, and cut the keloid tissue to precision without damaging the flap [Figure 1].

- Needle being inserted into the bulky part of keloid
Advantages of using a 24-G needle: They are easily available. Dissection is finer and precise. There is least injury to flap and lesser tissue handling.
2. Removing excess of central bulk
Another reason for keloid recurrence is leaving an extra tissue at the center of the keloid due to fear of perichondrial damage during aggressive dissection, tough access to the site with the available instruments, and delay of surgery due to bits and pieces removal. We here again used a 24-G needle, which was bent to make it like a J-shaped hook, with which one can easily hold the central bulk of tissue and remove it without any compromise to the flap [Figure 2].
- Needle bent like a J hook for excising central bulk of keloid
Advantage of J hook: It helps in avoiding any damage to the flap and perichondrium. It helps in faster excision and better visibility of the operative area.
3. Hydrodissection
Keloid tissues are very vascular as well. So, when an incision has been made, bleeding is an expected feature that further reduces the already small operative area, makes dissection difficult, and delays the operative time. Hence, we tried hydrodissection. Here, normal saline is taken in a 1-mL syringe and the needle is inserted into the keloid tissue by entry through normal skin, thus avoiding damage to flap, and then the saline is pushed into the region just below the flap [Figures 3 and 4]. This creates a plane between the flap and the keloid tissue and makes dissection easier [Figure 5].

- Illustrating hydrodissection being done away from flap

- Illustrating visible blanching after hydrodissection
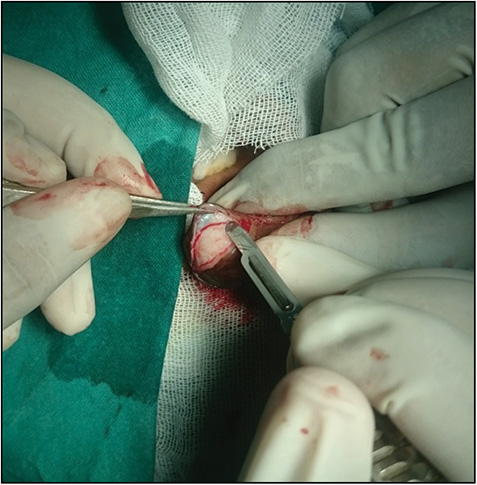
- Finer dissection, minimal bleeding post hydrodissection
Advantage of hydrodissection: It is easier to separate the skin and the keloid tissue. Excision of the keloid issue becomes much easier. Bleeding is comparatively lesser, dissection is faster, and least damage is done to the flap.
4. Protractor-like dressing
Dressings should serve the purpose of preventing complications as well as should address aesthetic aspects. We used dynaplast that was folded into half and stuck on itself at the closed end, leaving a gap between the two halves at the distal end. The two ends are stuck anteriorly and posteriorly with adequate pressure. The proximal end that is stuck to each other is then cut into the shape of auricle like a protractor [Figure 6].
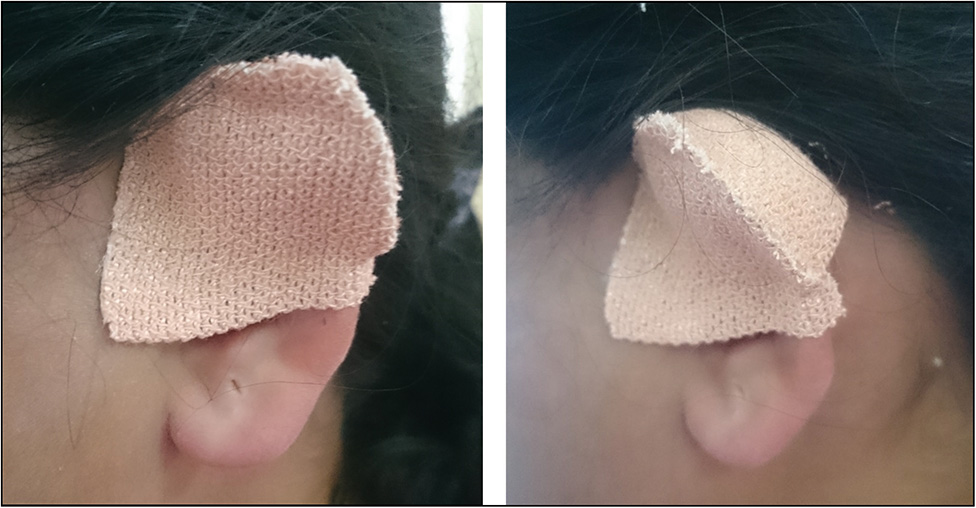
- Protractor like dressing
Advantage of protractor dressing: It is simple, easier, and effective dressing. It gives adequate pressure and good aesthetic appearance.
5. Bolster buttons
Surgery followed by pressure treatment has shown a good response rate of 90–100%, after excision of earlobe keloids. However, pressure must be maintained day and night for a minimum of 6–9 months, and premature release is frequently followed by recurrence of the lesion.
Keloid compression is based on collagen fragmentation and fibroblast degradation; the minimum effective pressure for this purpose being greater than 24 mmHg, so as to exceed the capillary pressure.[2] Various compression therapies have been devised, including silicone sheet earring plates with varied compliance and results.
We used commercially available buttons with four holes, which are stitched onto shirts, trousers, and the like. After sterilization, these buttons are sutured to the site of closure of the flaps [Figure 7], with absorbable sutures and left for a duration of 3 months.
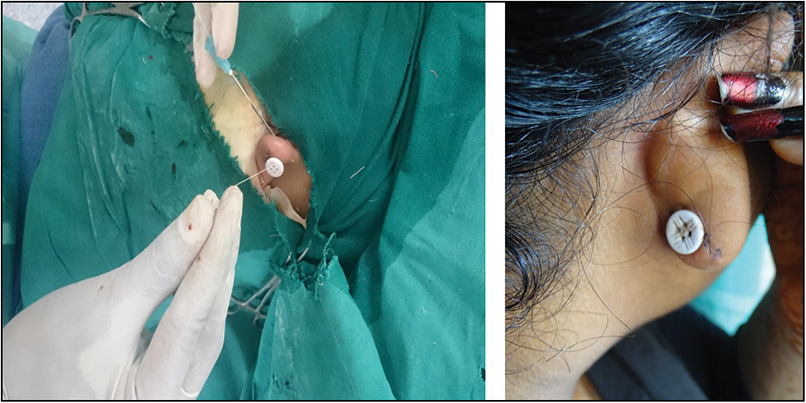
- illustrating insertion of a button
Advantage of bolster buttons: They are easily available and also hypoallergic. They prevent the formation of hematoma due to firm pressure. Use of this compression early helps in reducing recurrence rates. They are aesthetically pleasing, especially when different colors are used.
DISCUSSION
Several options for surgically treating keloid of the pinna have been used. The anatomic complexity of the area and the variability in the presentation of the keloid scars (size, location, etc.) are probably the determining factors that make standardizing a particular surgical procedure difficult.[3]
The procedures such as reduced tissue handling, complete excision of central keloid bulk, hydrodissection, and pressure dressing immediately after surgery have all made excision of keloid simpler, easier, and still accurate, with the added advantage of drastic reduction of time consumed. There is definitely and importantly a reduction in recurrence rates of keloids with these procedures.
We would hereby like to add 1C (compression with bolster button) and 1D (dressing) to the classic gold-standard method in anti-keloid surgery of 5As and 1B, i.e., from asepsis, atraumatic technique, absence of raw surface, avoidance of tension, accurate approximation of wound margin, and complete bleeding control are important factors for getting a successful outcome of the treatment.[45] Any technique that meets these criteria would, theoretically, provide a greater likelihood of success. The simple materials used and technically innovative modifications as described earlier will certainly meet these criteria and can be easily adapted, thus giving the hope that earlobe keloid excision becomes better and easier by the day.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
- A surgical approach for ear lobe keloid: keloid fillet flap. Plast Reconstr Surg. 2004;113:1668-74.
- [Google Scholar]
- Hydration and occlusion treatment for hypertrophic scars and keloids. Br J Plast Surg. 1992;45:599-603.
- [Google Scholar]
- Description of site-specific morphology of keloid phenotypes in an Afrocaribbean population. Br J Plast Surg. 2004;57:122-33.
- [Google Scholar]
- A new surgical treatment of keloid: keloid core excision. Ann Plast Surg. 2001;46:135-40.
- [Google Scholar]




