
Translate this page into:
Multiple Asymptomatic Juxta-Articular Nodules Mimicking Tuberous-Xanthoma–A Unusual Presentation of Tophaceous Gout
Address for correspondence: Dr. Kabir Sardana, Professor, Department of Dermatology, STD and Leprosy, Dr.RML Hospital and PGIMER, Baba Kharag Singh Marg, New Delhi, 110001. E-mail: kabirijdvl@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Asymptomatic, juxta-articular nodules are an uncommon morphology, which is usually diagnosed as xanthomas, calcinosis cutis or rheumatoid nodules. This study was represented as a case of gout, which is a disorder of purine metabolism resulting in elevation of serum uric acid and deposition of monosodium urate crystals within and around joints and manifests clinically as inflammatory arthritis. Urate crystal deposits have also been found in tendons, ligaments, viscera, and the skin, with the term “tophi” being used for the non-articular deposits. In the chronic stage, the lesion can be asymptomatic lesions and is often misdiagnosed.
Keywords
Differential
gout
juxta-articular
nodule
tophi

INTRODUCTION
Tophaeceous gout refers to the non-articular deposition of monosodium urate crystal resulting from a disorder in purine metabolism causing elevation of uric acid in the blood. Gout after many years of asymptomatic hyperuricemia may present with three different stages which include acute gouty arthritis; inter-critical gout, and chronic tophaceous gout.[1] We present a case of an elderly male presenting with the last stage of gout.
CASE HISTORY
A 60-year-old male patient presented with a 2-year history of asymptomatic multiple skin-colored nodules, which first appeared over the dorsal aspect of the right great toe and progressed to involve the extensor aspect of the elbows, right index finger, and both the lateral malleoli. He had been previously diagnosed as a case of tuberous xanthoma in another hospital. On detailed history, there was a history of ulceration of these nodules. He also gave a history of recurrent episodes of joint pains in the night since past 5 years, which gradually improved over the years. The patient was on oral antihypertensive agents and lipid-lowering agents for dyslipidemia.
Physical examination revealed multiple erythematous to skin-colored juxta-articular nodules of variable sizes with the largest nodule being about 8 cm in size present over the right lateral malleoli [Figure 1]. The nodule over the right index finger was ulcerated with the discharge of chalky white material [Figure 2]. A 4 mm punch biopsy was taken from the nodule over the extensor aspect of the right elbow [Figure 3]. X-ray examination was performed for all the involved joints [Figure 4].

- A large nodule of size 8 cms×5 cms present over the right lateral malleoli

- Multiple periarticular nodules on bilateral hands and feet with a single ulcerated nodule present over the right index finger
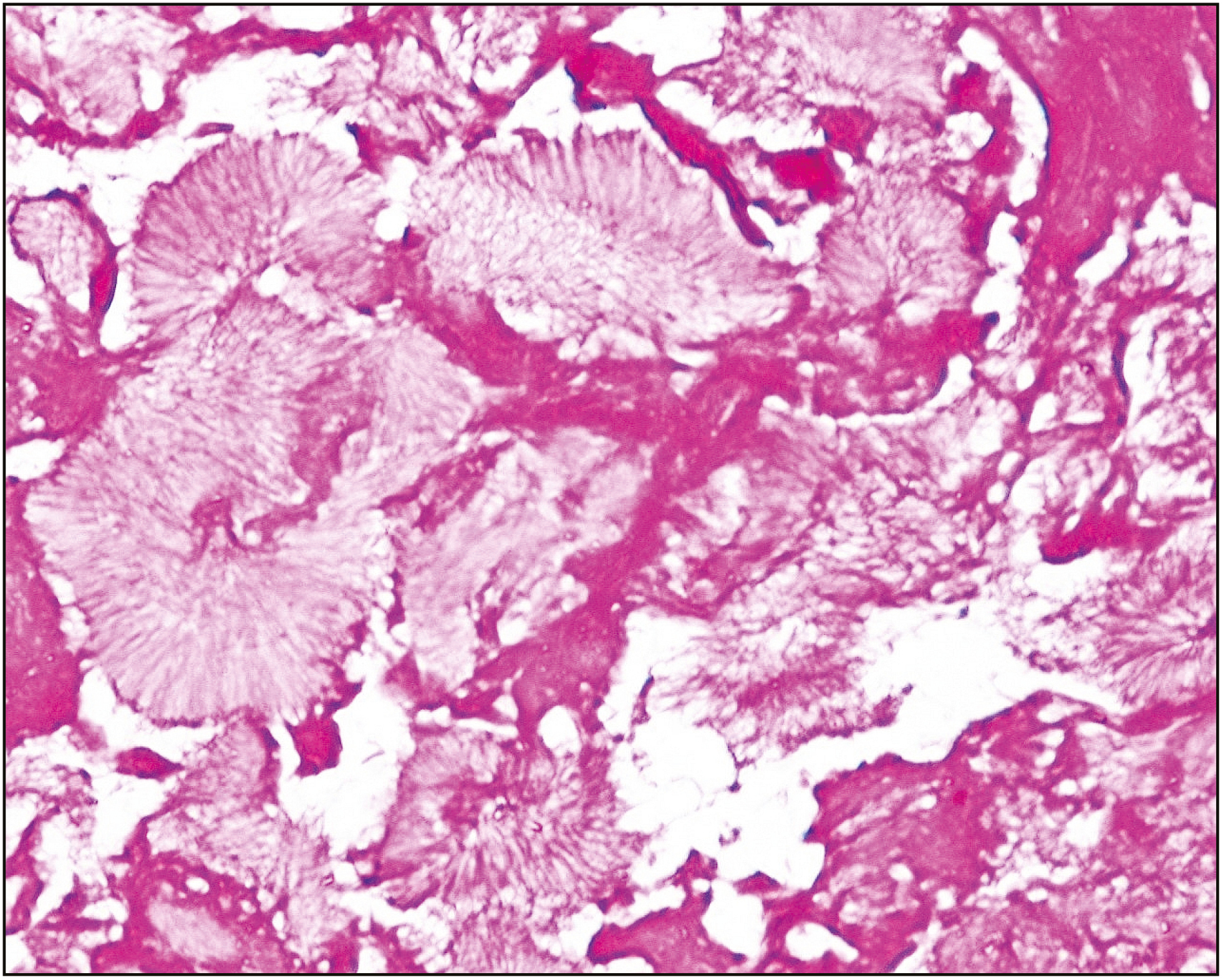
- Punch biopsy specimen stained with hematoxylin-eosin under 40X magnification that revealed characteristic foreign body inflammation surrounding aggregates of eosinophilic feathery material
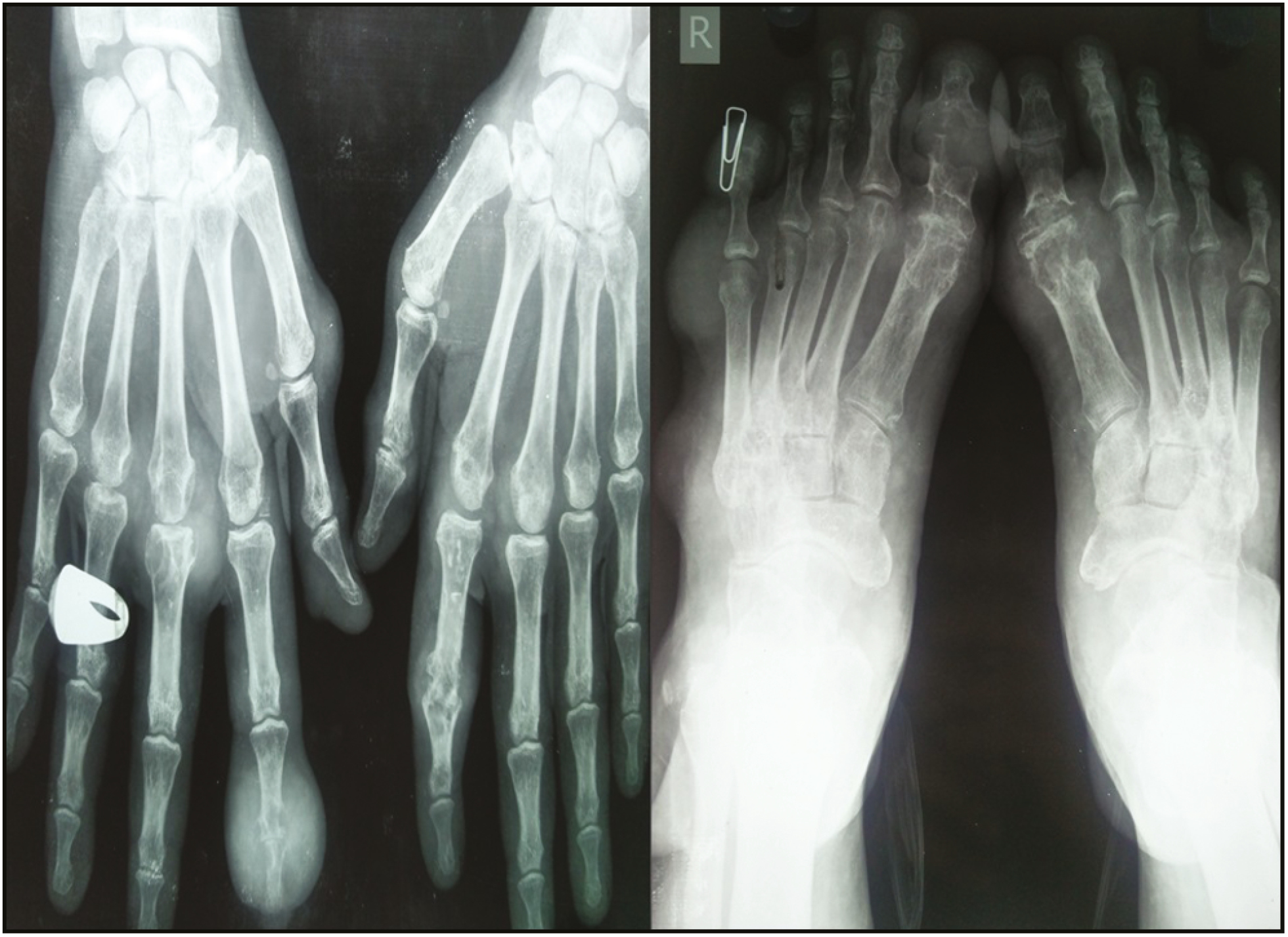
- X ray AP view of Hands and Feet show periarticular destruction, marginal and subchondral erosions with periarticular soft tissue swelling
A biopsy specimen revealed epidermal hyperkeratosis and irregular acanthosis. Mid and deep dermis showed foci of amorphous eosinophilic material along with needle-shaped crystals in a radial array. von Kossa stain for calcium was negative. The microscopic findings were in favor of a diagnosis of gouty tophi. Laboratory examination showed normal levels of serum calcium and phosphorus and an elevated level of uric acid (8.8 mg/dl, reference range: 2.6–7.5 mg/dL). X-ray examination revealed periarticular destruction, marginal and subchondral erosions with periarticular soft tissue swellings in the involved joints.
The patient was started on tablet febuxostat 40 mg twice a day and tablet colchicine 0.5 mg once daily. There has been a gradual improvement in his condition over the past 3 months with a reduction in the size of the lesions and stoppage of onset of new lesions with a reduction in the uric acid levels to 6.3 mg/dl. The patient was also offered surgical removal of the tophi but he refused to undergo a surgical excision.
DISCUSSION
Gout is a result of a purine metabolism defect that causes the elevation of serum uric acid and deposition of monosodium urate crystals within and around joints and manifests clinically as inflammatory arthritis. Urate crystal deposits have also been found in tendons, ligaments, viscera, and the skin, with the term “tophi” being used for the nonarticular deposits. Tophaceous gout can present with varied cutaneous manifestations including papular, nodular, ulcerative, and pustular forms.[2] The nodules can be firm, smooth or multilobulated and are situated in the subcutaneous plane.[3] The 3 different stages of gout, which may be seen after years of asymptomatic hyperuricemia, are acute gouty arthritis; intercritical gout, which includes the intervals between attacks; and chronic tophaceous gout.[1] In our case, the patient was in the last stage of gout, which explains the marked lack of symptomology and the mistaken diagnosis of xanthomas.
Multiple risk factors have been implicated in the development of chronic gout, including male gender, metabolic syndrome, renal insufficiency, purine over ingestion, ethanol use, and intake of a variety of medications such as cyclosporine.[45] The average interval from the first gouty attack to the onset of tophi is about 12 years.[6] Complications of tophi include pain, soft tissue damage and deformity, joint destruction and nerve compression syndromes such as carpal tunnel syndrome.[7] The principles of treatment for chronic tophaceous gout are based on dietary modifications along with medical and surgical therapy. Medical therapy is based on lowering the uric acid levels by using Xanthine oxidase inhibitors such as allopurinol and febuxostat or by uricosuric agents such as probenecid and silfinpyrazone. Surgical excision of tophi is undertaken in case it causes joint deformities with loss of range of motion, intractable pain or chronic ulceration. Acute inflammatory attacks are managed with colchicine and non-steroidal anti-inflammatory drugs.[2]
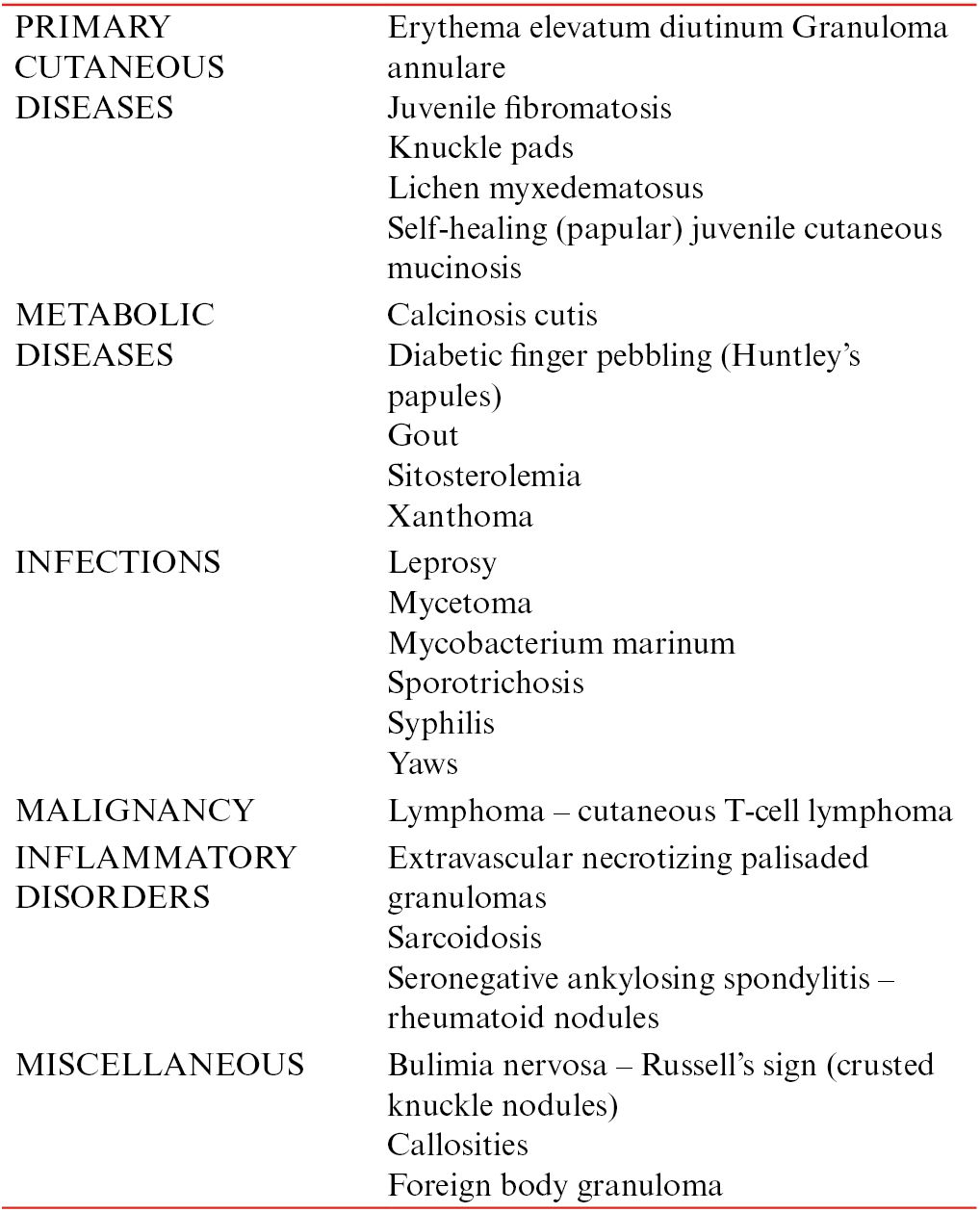
The differential diagnosis considered in a case of juxta-articular nodules are many but the ones relevant in our case included, multicentric reticulohistiocytosis wherein the nodules are yellowish papules and plaques with a characteristic “coral bead” like appearance around the nail folds and rarely ulcerate.[8] Tendon xanthomas are seen in familial hypercholesterolemia and are most commonly found attached to the extensor tendons over the knuckles and Achilles tendon. The histopathological examination reveals collagen in addition to foamy macrophages.[9] In calcinosis cutis, insoluble calcium salts are deposited in the cutaneous tissue as multiple chalky nodules, staining with Alizarin red S or von Kossa stain.[10] In our case, apart from the above diagnosis, gouty tophus was considered and the biopsy revealed the characteristic foreign body inflammation surrounding aggregates of eosinophilic feathery material.[2] This in conjunction with the raised uric acid and the X-ray findings was in favor of a diagnosis of tophaceous gout [Table 1].
Thus, chronic gout should be considered in cases of asymptomatic juxta-articular nodules and an early diagnosis can enable appropriate intervention and amelioration of the disorder.
Financial support and sponsorship
Nil.
Conflict of interest
None.
REFERENCES
- Multiple cutaneous creamy papules and nodules: A case of miliarial gout. J Cutan Med Surg. 2015;19:317-9.
- [Google Scholar]
- Deposition diseases. In: Bolognia J, Jorizzo H, Rapini R, eds. Dermatology. New York NY: Mosby Elsevier Ltd; 2003. p. :669-72.
- [Google Scholar]
- Tophaceous gout in the elderly: A clinical case review. Clin Rheumatol. 2012;31:1127-32.
- [Google Scholar]
- The past four decades of progress in the knowledge of gout, with an assessment of the present status. Arthritis Rheum. 1973;16:431-45.
- [Google Scholar]
- Cutaneous Histiocytoses. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, eds. Rook’s textbook of dermatology (9th ed). United Kingdom, U.K: Wiley Blackwell; 2016. p. :136.22-136.24.
- [Google Scholar]
- Xanthomas and abnormalities of lipid metabolism and storage. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, eds. Rook’s textbook of dermatology (9th ed). United Kingdom, U.K: Wiley Blackwell; 2016. p. :62.2-62.3.
- [Google Scholar]
- Calcifying and ossifying disorders of the skin. In: Bolognia J, Jorizzo J, Rapini R, eds. Dermatology. New York NY: Mosby Elsevier Ltd; 2003. p. :729-36.
- [Google Scholar]
- Rheumatoid Nodules - American Osteopathic College of Dermatology (AOCD). Available from: http://www.aocd.org/?page=RheumatoidNodules
- Rheumatoid nodules: differential diagnosis and immunohistological findings. Ann Rheum Dis. 1993;52:625-26.
- [Google Scholar]




