
Translate this page into:
Carpal Tunnel Syndrome Caused by Intraneural Lipoma of the Median Nerve and Arteriovenous Malformation
Address for correspondence: Dr. Arif Aydin, Department of Plastic, Reconstructive and Aesthetic Surgery, Beyhekim State Hospital, Konya, Turkey. E-mail: arifaydin4@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Carpal tunnel syndrome can be the result of a wide variety of etiologic factors. Compressive causes are rare and tumors causing compression are even rarer. We present a case with a carpal tunnel syndrome caused by an intraneural lipoma and an arteriovenous malformation concomitantly. The lesions were excised, and the patient recovered with full hand function and entire disappearance of acroparesthesia. To our knowledge, this is the first case report of carpal tunnel syndrome caused by an intraneural lipoma and an arteriovenous malformation concomitantly.
Keywords
Arteriovenous malformation
carpal tunnel syndrome
intraneural lipoma

INTRODUCTION
Carpal tunnel syndrome (CTS) is the most frequent peripheral compression neuropathy. It is usually idiopathic and rarely caused by a space-occupying lesion. Adipose cells are located in epineurium between fascicles of peripheral nerves. However, lipomatous tumors that arise in the peripheral nerves are extremely rare. Many terms have been used to refer to lipomatous tumors involving peripheral nerves such as intraneural lipomas, neural fibrolipoma, lipofibromatous hamartoma, perineural lipoma, macrodystrophia lipomatosa, and lipomatosis of nerve.[1] Intraneural lipomas most commonly occur in the forearm and the wrist, particularly within the median nerve.[2] Large lesions may cause progressive compression neuropathy. Arteriovenous malformation causing compression of a nerve is extremely rare.[3]
CASE REPORT
We report a 51-year-old woman presenting with a history of an enhancing subcutaneous mass on the left hand over the past 5 years. She had a history of CTS on her right hand and she had a carpal tunnel release operation 2 months ago for her right hand. She had no history of trauma. She experienced episodes of moderate pain and paresthesias on the first, second, and third fingers of her left hand. Physical examination identified a 3×3-cm subcutaneous tumor on the center of the left palmar region. Tinel’s sign was present in the wrist. The electromyographic examination inferred severe CTS. An ultrasound was performed and two separate masses were seen, but they could not be specified. A magnetic resonance imaging (MRI) was recommended by the radiologist. MRI revealed an 8×27×29-mm contrast-free soft-tissue formation in the midpalmar space and another 6×8-mm lesion in the third and fourth metacarpal base region, which was contrast enhanced [Figure 1]. Under axillary block anesthesia and tourniquet, an incision was made over the transverse carpal ligament through the midpalmar area. A 0.8×1.2-cm vascular mass was identified proximal to the third and fourth metacarpal base region just above the carpal tunnel causing compression to the tunnel [Figure 2]. The mass was totally excised and hemostasis was achieved. The transverse carpal ligament was released and median nerve was exposed. An encapsulated mass was found to originate distal to the division of the nerve, spreading the fibers of the median nerve [Figure 3]. The tumor was totally removed after microdissection under loupe magnification without damaging the nerve fibers. Histological examination revealed the midpalmar mass as a lipomatous tumor composed of mature adipocytes without intermingling nerve fibers and the vascular mass was diagnosed as an arteriovenous malformation [Figures 4 and 5]. This patient was diagnosed with intraneural lipoma based on the clinical and pathological findings. Two months postoperatively, the patient recovered with full hand function and entire disappearance of acroparesthesia. On follow-up 1.5 years postoperatively, the patient was free from hypesthesia and paresthesia, with no evidence of tumor recurrence.

- (A) MRI findings of intraneural lipoma spreading the median nerve fibers. (B) MRI findings of the arteriovenous malformation, a contrast-enhanced mass located at the base of the third and fourth metacarpal base region
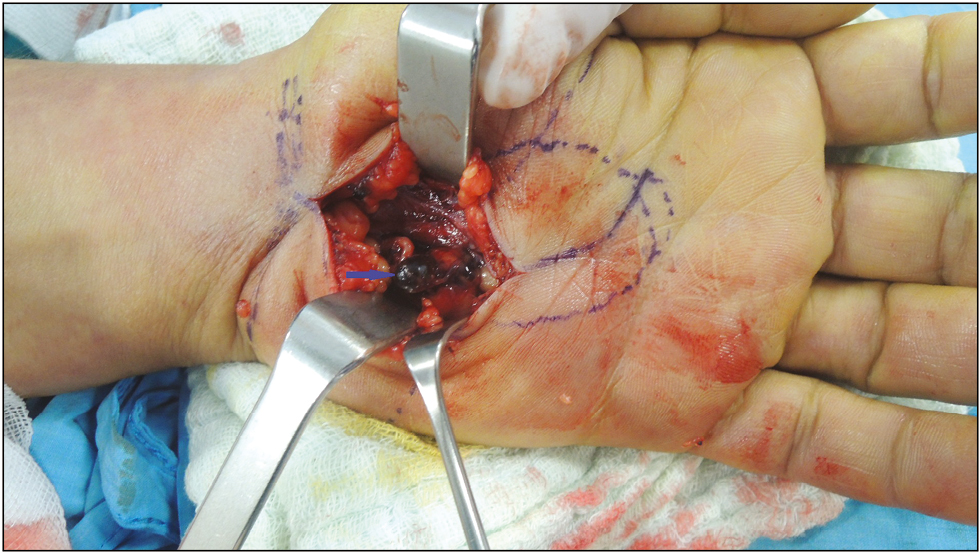
- Arteriovenous malformation marked with blue arrow
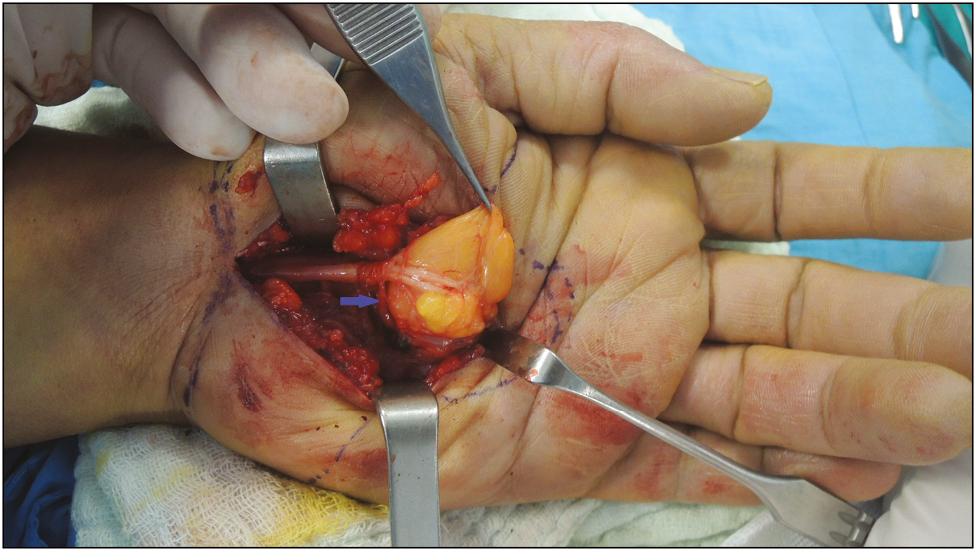
- Intraneural lipoma marked with blue arrow
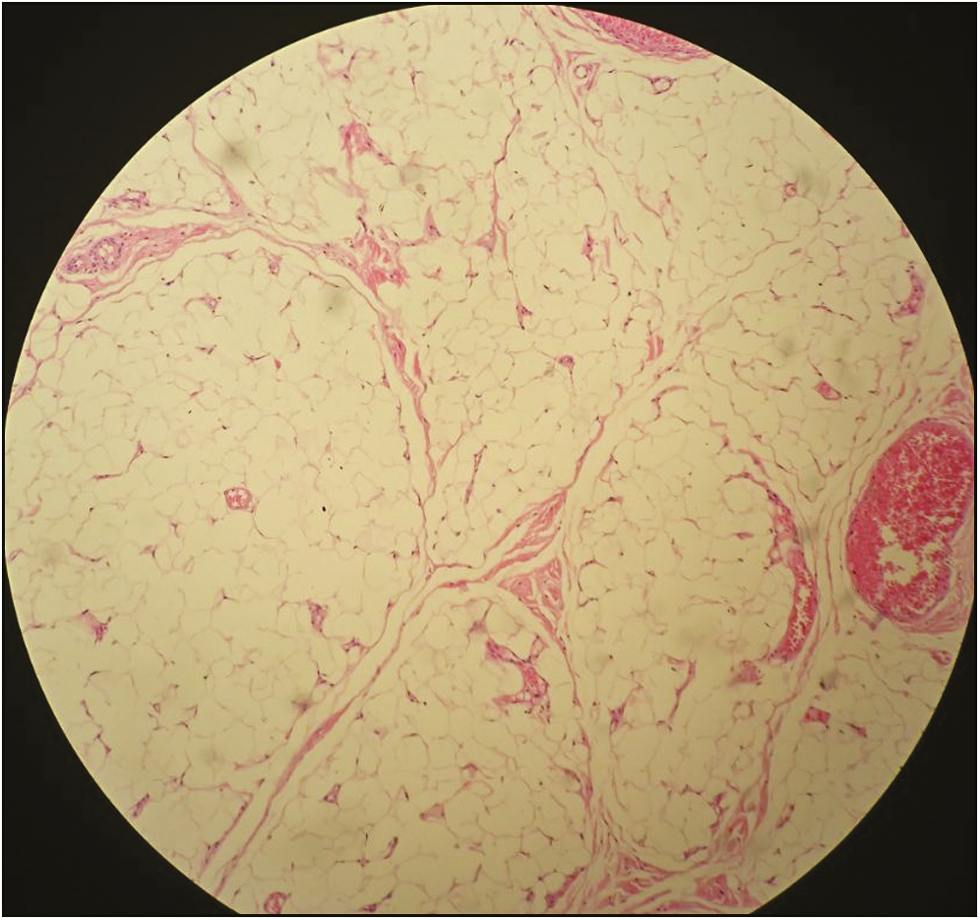
- Histopathological view of intraneural lipoma
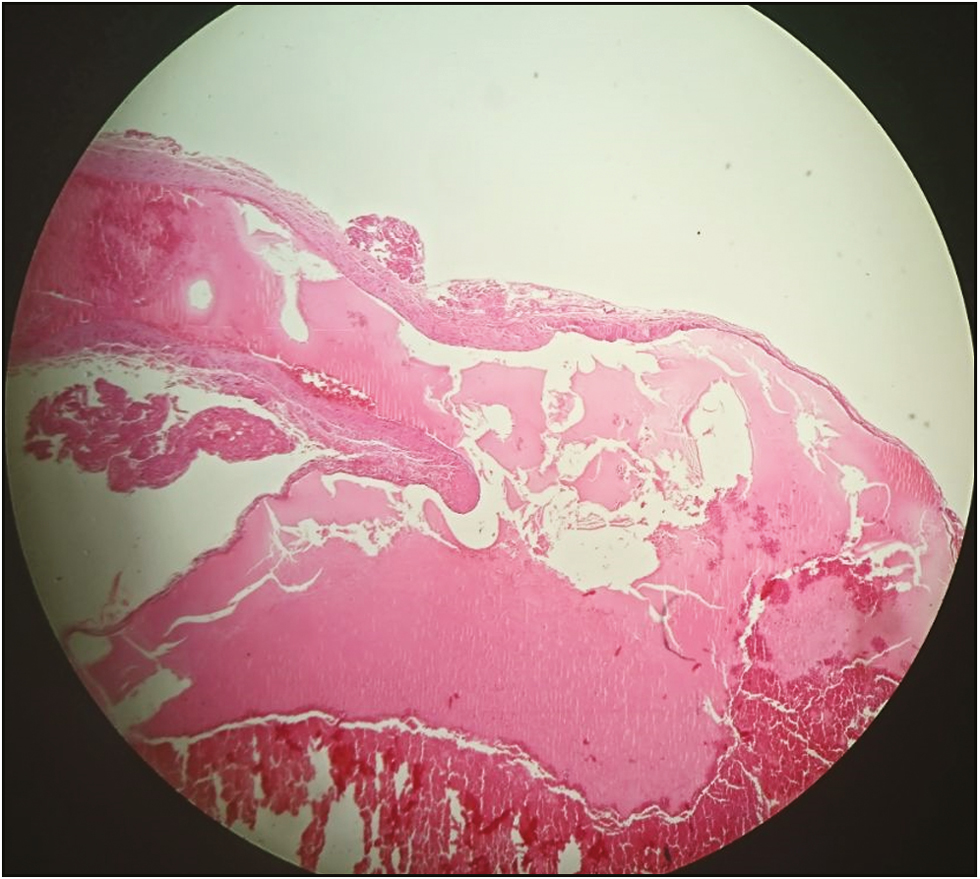
- Histopathological view of arteriovenous malformation
DISCUSSION
The most common cases of the CTS are idiopathic. One of the rare etiologic factors of CTS is a space-occupying lesion such as the swelling of tendon sheath, distal radius fracture, rheumatoid arthritis, volar dislocation of lunate, ganglion, and gout. If these lesions are not treated, the patient’s symptoms will not improve.[4] Idiopathic CTS is usually bilateral. When unilateral symptoms and unilateral abnormal nerve conduction tests are present, secondary causes of CTS, like space-occupying lesions, should be kept in mind. Nakamichi and Tachibana[5] reported an increased prevalence of space-occupying lesions in patients with unilateral CTS. In their study, of 20 patients with abnormal unilateral symptoms and unilateral positive electrophysiological tests, 65% showed various causes for median nerve compression, such as occult ganglion, occult calcified mass, tuberculous synovitis, and nonspecific synovitis. In contrast to their study, our patient had bilateral CTS and she had tumoral masses on her left hand compressing the median nerve. On physical examination, if the patient has swelling or palpable mass in the volar area of hand or wrist, ultrasound or MRI should be performed.
Vascular tumors causing a CTS are extremely rare conditions. Hariri et al.[6] reported a venous malformation causing CTS at the level of the wrist. Oztekin and Karaarslan[7] reported a CTS due to a cavernous hemangioma of the median nerve. However, we could not find any arteriovenous malformation compressing median nerve in the literature.
The tumors that could be separated from the neural elements, which showed the pathological characteristics of a benign lipoma without intermingling neural elements, were termed as ‘true intraneural lipoma’ by Rusko and Larson.[8] Most of the intraneural lipoma tend to occur in the median nerve and have a female predominance.
Spinner et al.[9] proposed a new classification for lipomatous tumors, involving the peripheral nerves based on the pathological definitions of lipoma and lipomatosis of the nerve by the WHO. Their classification is according to the location (intraneural or extraneural) and the presence of focal (lipoma) or diffuse (lipomatosis) lesion. Lipomatosis of nerve consists of diffuse mature fatty or fibroadipose tissue, which can be epineural or interfascicular with macroscopically normal entrapped fascicles. Lipomas are focal masses that can affect epineurium (intraneural lipomas) or they may originate from an extraneural region and compress the nerve. The authors grouped adipose tumors into two main categories: (1) Basic lipomas or lipomatosis of nerve (either intra- or extraneural) and (2) combined lesions. Combined lesions are combinations of intra- and extraneural lesions, combinations of lipomas with lipomatosis, or combined intra- and extraneural lipomas in the setting of lipomatosis.[19]
Because intraneural lipomas are encapsulated tumors displacing the nerve fascicles, surgical excision of the lipoma is safe and effective in reducing neuropathic symptoms.
CONCLUSION
Surgeons should be suspicious about the soft-tissue tumors of the hand, especially in unilateral CTS cases, and further special studies using ultrasound or MRI should be performed when necessary. Transverse carpal ligament release and excision of the lesions provide excellent recovery. To our knowledge, this has been the first case report of CTS caused by an intraneural lipoma and an arteriovenous malformation concomitantly.
Previous Presentation: This study was presented at the National Congress of Turkish Plastic, Reconstructive and Aesthetic Surgery Association in 2016 in Antalya, Turkey.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of interest.
REFERENCES
- Peripheral nerve lipoma: Case report of an intraneural lipoma of the median nerve and literature review. Asian J Neurosurg. 2016;11:458.
- [Google Scholar]
- Intraneural lipomatous tumor of the median nerve: Three case reports with a review of literature. Int J Surg Case Rep. 2012;3:407-11.
- [Google Scholar]
- Intraneural hemangioma of the median nerve: A case report. J Brachial Plex Peripheral Nerve Inj. 2008;22:3-5.
- [Google Scholar]
- Giant lipoma: An unusual cause of carpal tunnel syndrome. Pan Afr Med J. 2011;9:29.
- [Google Scholar]
- Unilateral carpal tunnel syndrome and space-occupying lesions. J Hand Surg Br. 1993;18:748-9.
- [Google Scholar]
- Venous malformation involving median nerve causing acute carpal tunnel syndrome. J Hand Surg Eur Vol. 2011;36:431-2.
- [Google Scholar]
- [Carpal tunnel syndrome due to a cavernous hemangioma of the median nerve] Acta Orthop Traumatol Turc. 2003;37:170-2.
- [Google Scholar]
- Intraneural lipoma of the median nerve: Case report and literature review. J Hand Surg Am. 1981;6:388-91.
- [Google Scholar]
- Adipose lesions of nerve: the need for a modified classification. Clinical article. J Neurosurg. 2012;116:418-31.
- [Google Scholar]




