
Translate this page into:
Asymptomatic Pinkish-Red Nodule over the Posterolateral Tongue
Address for correspondence: Dr. Sidharth Sonthalia, SKINNOCENCE: The Skin Clinic and Research Centre, C-2246 (Ground Floor), “Suhridaya,” Sushant Lok-1, Block-C, Gurugram, Haryana 122009, India. E-mail: sidharth.sonthalia@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A young otherwise healthy male presented with asymptomatic pinkish-red nodule over postero-lateral tongue with the suspicion of having developed oral cancer. Biopsy from the lesion showed multiple circumscribed nodules in the lamina propria comprised of numerous oval and spindle-shaped cells. Abundant lymphatic tissue with germinal centres were also observed. Differentials included mucosal neuroma, traumatic neuroma, subgemmal neurogenous plaque, neurofibroma, and lingual tonsils. This quiz discusses the diagnosis and approach to the differential diagnoses in such a clinical setting.
Keywords
Mucosal neuroma
SNP
subgemmal neurogenous plaque
tongue
traumatic neuroma

CASE PRESENTATION
A 28-year-old man presented with otherwise completely asymptomatic fleshy swelling over the posterolateral surface of right side of tongue for 6 months. Bruxism and tongue bite were ruled out on questioning. He denied addictions such as chewing of betel nut/tobacco and smoking. No systemic complaints were reported. Despite lack of symptoms, the patient was anxious about the lesion being oral cancer. Intraoral examination revealed an oval nodular swelling of 1×2cm size in the foliate papillae of the right posterolateral tongue. The pinkish-red nodule was firm, non-tender, and had subtle transverse grooves and superficial erosion over the surface [Figure 1]. Dental history was noncontributory and cervical lymphadenopathy was absent. Histopathology showed numerous oval and spindle-shaped cells in the lamina propria arranged as circumscribed nodules. Within the circumscribed neural plexus, the deepest portion showed small nerve fascicles and the superficial portion revealed linear bundles of spindle cells interspersed with thin fibrillary collagen fibers. Abundant lymphatic tissue with germinal centers was conspicuous [Figures 2 and 3].

- Clinical image displaying a single horizontal oval pink-colored nodule, approximately 1×2cm in size in the foliate papillae located in the right posterolateral tongue. Note the presence of subtle transverse grooves and superficial erosion on the surface
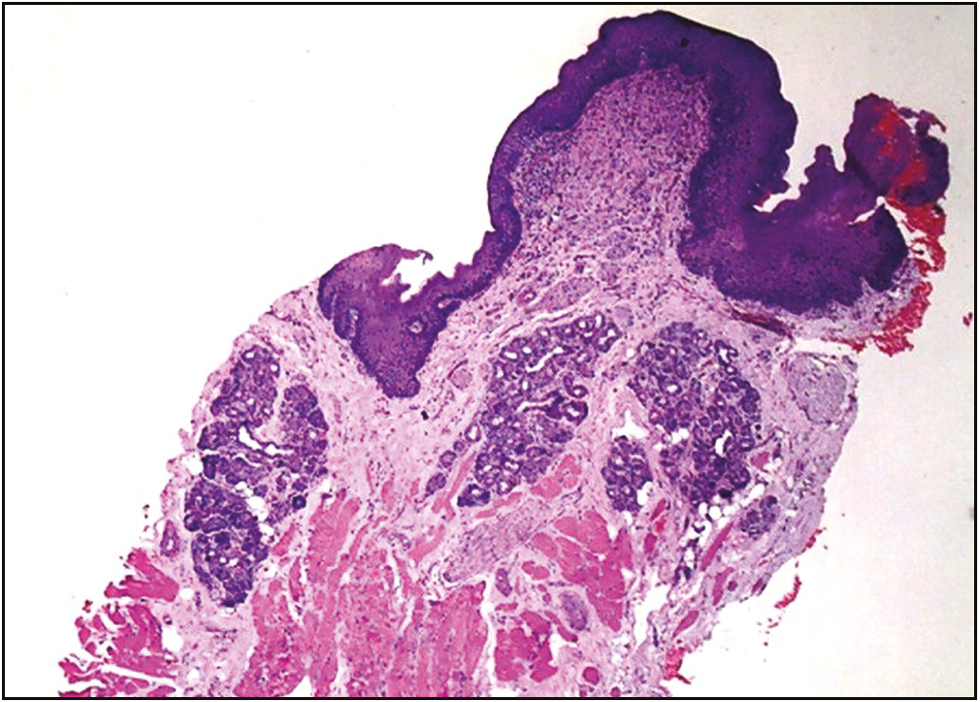
- Histopathology showing normal mucosal epithelium, numerous oval- and spindle-shaped cells arranged as circumscribed nodules in the lamina propria, and abundant lymphatic tissue (hematoxylin and eosin, 100×)
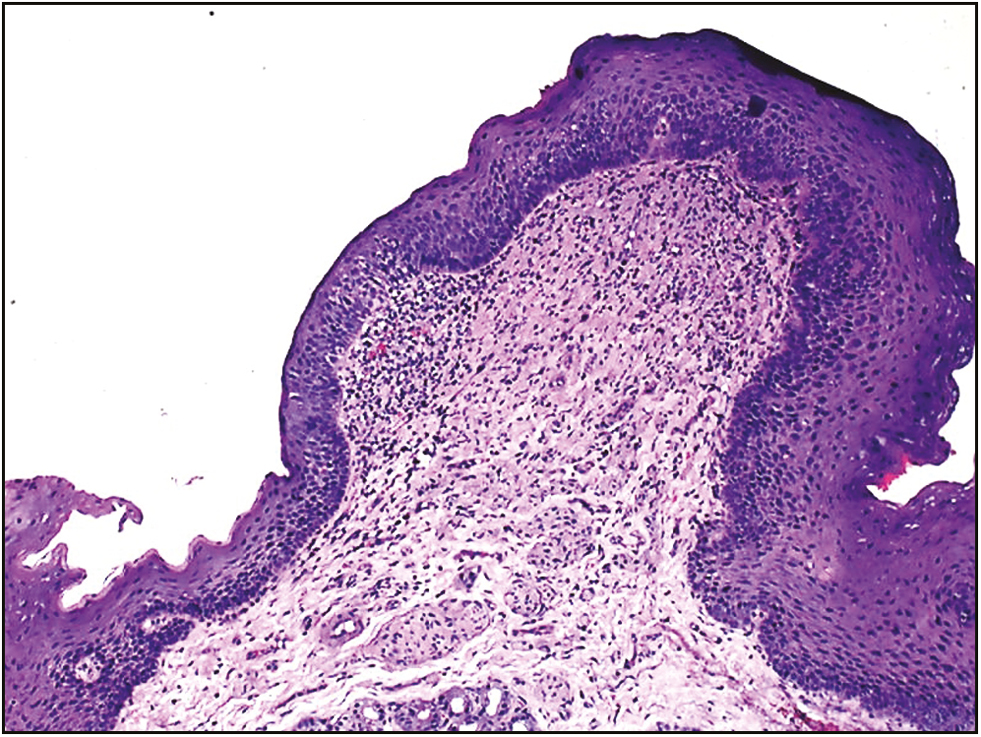
- Histopathology at higher magnification revealed two components of the circumscribed neural plexus, small nerve fascicles present in the deepest portion and linear bundles of spindle cells interspersed with numerous thin fibrillary collagen fibers in the superficial portion. Note the abundant lymphatic tissue with germinal center formation (hematoxylin and eosin, 400×)
What Is Your Diagnosis?
Answer: Subgemmal Neurogenous Plaque (SNP)
DISCUSSION
The extreme posterolateral borders of the tongue consist of foliate papillae that show vertically oriented corrugations and lamellations. Subgemmal neurogenous plaque (SNP) typically arises in foliate papillae as an asymptomatic or rarely painful pinkish nodule or a frankly exophytic lesion, sometimes accompanied by trauma-induced ulceration.[12345] SNPs may affect any age and gender. The lesions of SNP could be reactive, representing neuronal dysplasia, or result from trophic influences of gustatory nerve fibers.[4] The location and morphology of SNP may mimic soft tissue lesions such as inflammatory fibrous hyperplasia, fibroma, neurofibroma, and mucosal neuroma.[123] Hyperplastic lingual tonsils and lingual thyroid are distinguishable on histopathology.[3] The histological hallmark of SNP is subepithelial proliferation of nerve plexus with aggregates of ganglion cells.[12345] A biphasic microscopic pattern has been observed in SNP; a circumscribed nerve plexus parallel to the epithelial surface with a deep and superficial portion composed of small nerve fascicles and spindle cells interspersed with fibrous connective tissue, respectively.[1] Presence of lymphocytic infiltrate and lymphoid follicles is frequent.[12345] Marked S-100 positivity in the spindle cells of the neural plexus (Schwann cells) and positive immunoreaction to pancytokeratin (taste buds) are seen on immunohistochemistry.[14]
Neurofibroma, traumatic neuroma, and mucosal neuroma are often confused on histopathology.[124] Neurofibroma is usually deep seated and displays characteristic cellular arrangement in short fascicles, whorls, or storiform pattern.[46] Clusters of ganglion cells may also be seen in a traumatic neuroma; however, the histological features that differentiate it from related differentials including SNP subsume: haphazard proliferation of prominent nerve fascicles, including axons with their investitures of myelin, Schwann cells, and fibroblasts embedded in a fibrotic stroma with focal areas of hyalinized collagen.[6]
Mucosal neuroma was the initial histopathological diagnosis reported for this patient. Oral mucosal neuromas, which are often associated with multiple endocrine neoplasia MEN2b, indeed constitute the closest histological differential of SNP.[7] The oral lesions present tortuous bundles of nerves with a prominent perineurium within a fibrous stroma. Mature ganglion cells within enlarged lingual nerves may be rarely encountered.[6] Patients with MEN2b with lingual mucosal neuroma(s) present with early gastrointestinal (GI) symptoms secondary to GI ganglioneuromatosis.[7]
Conclusively, the diagnosis of SNP was clinched based on the lack of symptoms, characteristic histology with prominent lymphoid proliferation, and lack of clinical and histological features typical of other differentials. Lesion excision or biopsy is usually required only in symptomatic cases to rule out neoplasia.[12] Veritably, en bloc resection of the left posterolateral tongue had been suggested for this patient also by two oromaxillofacial surgeons. The patient was rescued opportunely from unnecessary aggressive surgery after we sorted the clinicopathologic correlation with our dermatopathologist in detail. Thus, awareness about this condition is imperative for clinicians and pathologists to avoid misdiagnosis and prevent unnecessary procedures.
Five learning points are as follows:
-
SNP typically arises in foliate papillae as an asymptomatic pinkish nodule or a frankly exophytic lesion, sometimes accompanied by trauma-induced ulceration.
-
Histological hallmark of SNP is subepithelial proliferation of nerve plexus with aggregates of ganglion cells with a biphasic microscopic pattern comprising a circumscribed nerve plexus and spindle cells.
-
Clinical differentials include soft tissue lesions such as inflammatory fibrous hyperplasia, fibroma, neurofibroma and mucosal neuroma, and hyperplastic lingual tonsils and lingual thyroid.
-
Neurofibroma, traumatic neuroma, and mucosal neuroma are often confused on histopathology because of the abundant neuronal cells.
-
Awareness about this condition is imperative for clinicians and pathologists to avoid misdiagnosis and prevent unnecessary procedures.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We thank Dr. Uday Khopkar from the Department of Skin, STD and Leprosy, Seth Gordhandas Sunderdas Medical College and the King Edward Memorial Hospital, Mumbai, Maharashtra, India for providing us with the histopathological images of the mucosal biopsy.
REFERENCES
- Subgemmal neurogenous plaque of the tongue: a report of three cases. Oral Maxillofac Surg. 2017;21:351-5.
- [Google Scholar]
- Subgemmal neurogenous plaque: clinical and microscopic evaluation of 7 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:920-4.
- [Google Scholar]
- Asymptomatic nodule in the tongue. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:281-3.
- [Google Scholar]
- Structural organization of subgemmal neurogenous plaques in foliate papillae of tongue. Hum Pathol. 2004;35:991-9.
- [Google Scholar]
- Lingual subgemmal neurogenous plaques with pseudoepitheliomatous hyperplasia: incidental pseudomalignant condition. Pathol Int. 2006;56:462-5.
- [Google Scholar]
- Oral traumatic neuroma with mature ganglion cells: a case report and review of the literature. J Oral Maxillofac Pathol. 2009;13:67-9.
- [Google Scholar]
- Oral mucosal neuromas leading to the diagnosis of multiple endocrine neoplasia type 2B in a child with intestinal pseudo-obstruction. Gastroenterol Hepatol (N Y). 2007;3:208-11.
- [Google Scholar]




