
Translate this page into:
Cross-Sectional Study of Dermatoscopic Findings in Relation to Activity in Vitiligo: BPLeFoSK Criteria for Stability
Address for correspondence: Dr. Balakrishnan Nirmal, Department of Dermatology, Christian Medical College, Vellore, Tamil Nadu, India. E-mail: nimu2swash@yahoo.co.in
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Stability in vitiligo is an important concept in guiding patient management and a vital prerequisite before vitiligo surgery. Disease activity of vitiligo based on patient’s history is imprecise. It is practically impossible to perform biopsy from all lesions of vitiligo to ascertain stability. Dermatoscopy can be used to examine all clinical lesions in a patient of vitiligo. There is a need to validate many reported dermatoscopic findings for universal use.
Aims:
To analyze the significance of dermatoscopic findings in the activity of vitiligo and to devise a cutoff score for stable vitiligo.
Materials and Methods:
Dermatoscopic examination was performed in 85 patients clinically diagnosed with vitiligo. Six dermatoscopic parameters, namely, border, pigment network, perilesional hyperpigmentation, perifollicular pigmentation, satellite lesions, and micro-Koebner phenomenon (acronym: BPLeFoSK) were evaluated against Wood’s lamp findings as standard. Chi-square test was used to test association between categorical variables. Cutoff values for stability for these six parameters were plotted in receiver operating curve.
Results:
A total of 131 vitiligo lesions were analyzed with dermatoscopy. Absence of satellite lesions and absence of micro-Koebner phenomenon were the most sensitive parameters (96.7% and 100%, respectively). Sharp border and absent or reticulate pigment network within the vitiligo patch were the most specific findings (100% and 91.5%, respectively).
Conclusion:
A cutoff score of more than or equal to 1.5 using the “BPLeFoSK criteria” indicates stability in the vitiligo lesion.
Keywords
Dermatoscopy
stability
vitiligo

INTRODUCTION
Vitiligo is an acquired disorder of depigmentation because of loss of melanocytes. The disease has an incidence of 0.5%–2% with no ethnic or sex predilection. It is clinically characterized by white macules because of loss of melanocytes either by melanocytorrhagy or autoimmune destruction.[1] Though vitiligo is a benign disorder, it has a huge impact on the psychological well-being of the patient and can lead on to emotional distress.[2] Medical management has its limitations and might not produce complete repigmentation in a subset of patients. Advances in vitiligo surgery have offered a ray of hope in many of these patients.
However, stability of the patch is a prerequisite before surgery. According to Falabella,[3] a lesion with lack of progression or no new lesions for 2 years, absence of recent Koebner phenomenon, positive minigrafting test, absence of Koebner phenomenon at donor site, and evidence of repigmentation of existing patches either spontaneously or with medical therapy is considered stable. Assessing stability with patient history may be unreliable and performing minigrafting in all patients is not practical.[4] Also, according to the concept of lesional stability,[5] the same patient can have both stable and unstable lesions making it practically impossible to biopsy all lesions. Hence, a noninvasive method is necessary to assess all the lesions. Dermatoscopy allows for examination of all lesions and appreciation of subtle features invisible to naked eye. Vitiligo dermatoscopy is relatively underused and there is a paucity of studies indicating it.
MATERIALS AND METHODS
Aim and objectives
Our aim and objectives were to analyze the various dermatoscopic findings in vitiligo, to define patterns in stable as against unstable lesions, and also to ascertain the significance of each finding in the assessment of stability of vitiligo. We also aimed to devise a scoring system for each of these dermatoscopic findings and a cutoff value for stable vitiligo.
Study design
The study was designed as an observational cross-sectional study using dermatoscopy to ascertain stability of vitiligo lesions in 131 lesions from 85 patients from August 2014 to August 2015. Patients attending dermatology outpatient department with a clinical diagnosis of vitiligo and willing to participate in the study were included in the study.
Ethical considerations
A written and signed informed explanatory consent was obtained from all the patients before the initiation of therapy. This clinical study was performed in accordance with the Declaration of Helsinki after approval by the ethics committee of our hospital.
Wood’s lamp evaluation
A detailed history was obtained from the included 85 patients and clinical examination was performed using a Wood’s lamp. Four Wood’s lamp findings, namely, achromic with sharply defined border, hypopigmented with poorly defined border, trichrome, and inflammatory were used. Of which, achromic with sharply defined border was considered stable and the latter three findings were for unstable vitiligo. Wood’s lamp examination was considered standard as its findings have been validated by previous studies.
Dermatoscopic evaluation
Dermatoscopic analysis was performed using a handheld Dermlite DL3 dermatoscope (Dermlite DL3, 3Gen Inc, USA). Images were obtained with a Sony Cybershot DSC-W800 20.1 MP digital camera (Sony corp., Tokyo, Japan) attached to the dermatoscope with a universal adapter. The following six dermatoscopic parameters denoted by the acronym “BPLeFoSK” were analyzed in 131 lesions of vitiligo.
Border
Pigment network within the patch
Perilesional hyperpigmentation
Perifollicular hyperpigmentation
Satellite lesion
Micro-Koebner phenomenon
Border can be sharp, ill-defined, or trichrome [Figure 1]. Pigment network within the lesion can be absent, reticular, reduced, or reverse [Figure 2]. A stable vitiligo lesion has four positive predictors: sharp border, reticular or absent pigment network within the patch, perilesional hyperpigmentation [Figure 3A], and perifollicular pigmentation [Figure 3B] and two negative predictors: satellite lesions [Figure 3C], micro-Koebner phenomenon [Figure 3D].
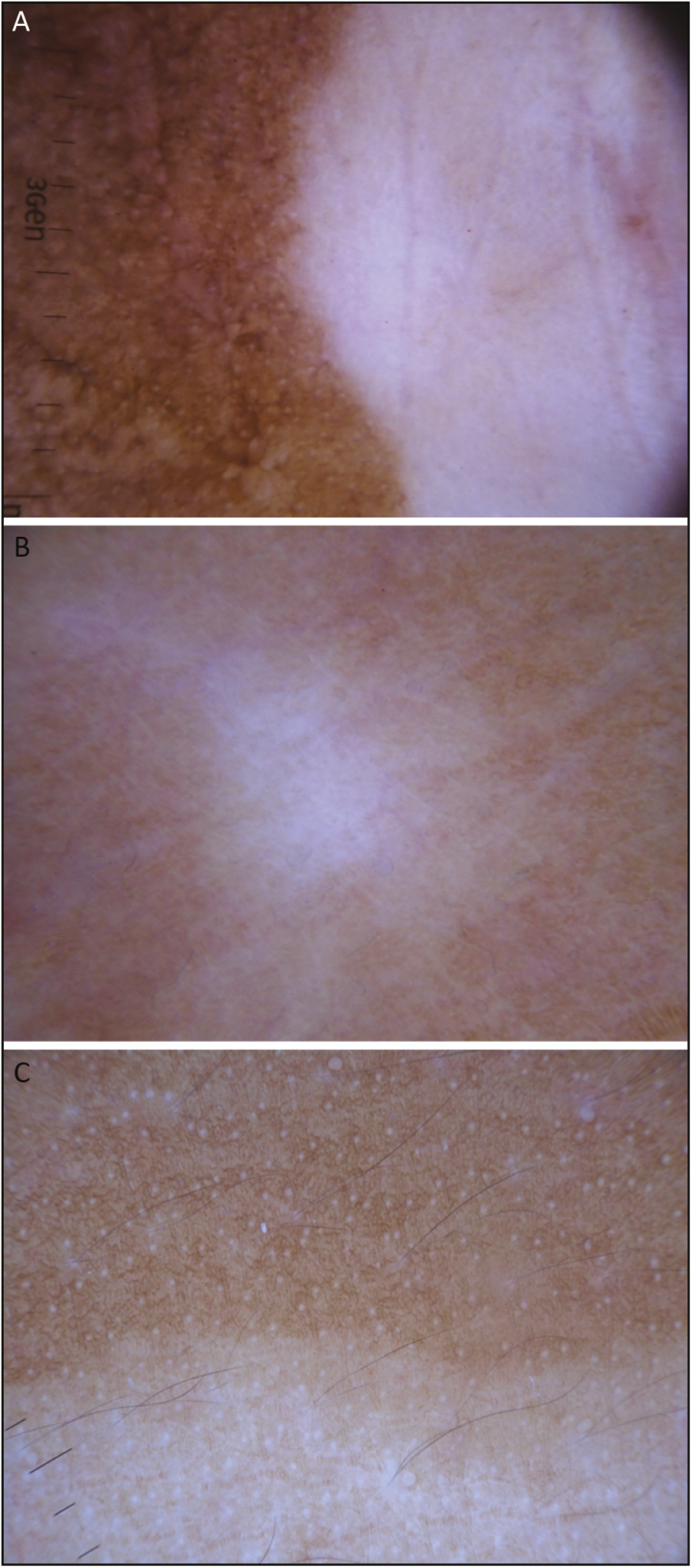
- Border. (A) Sharp. (B) Ill-defined. (C) Trichrome
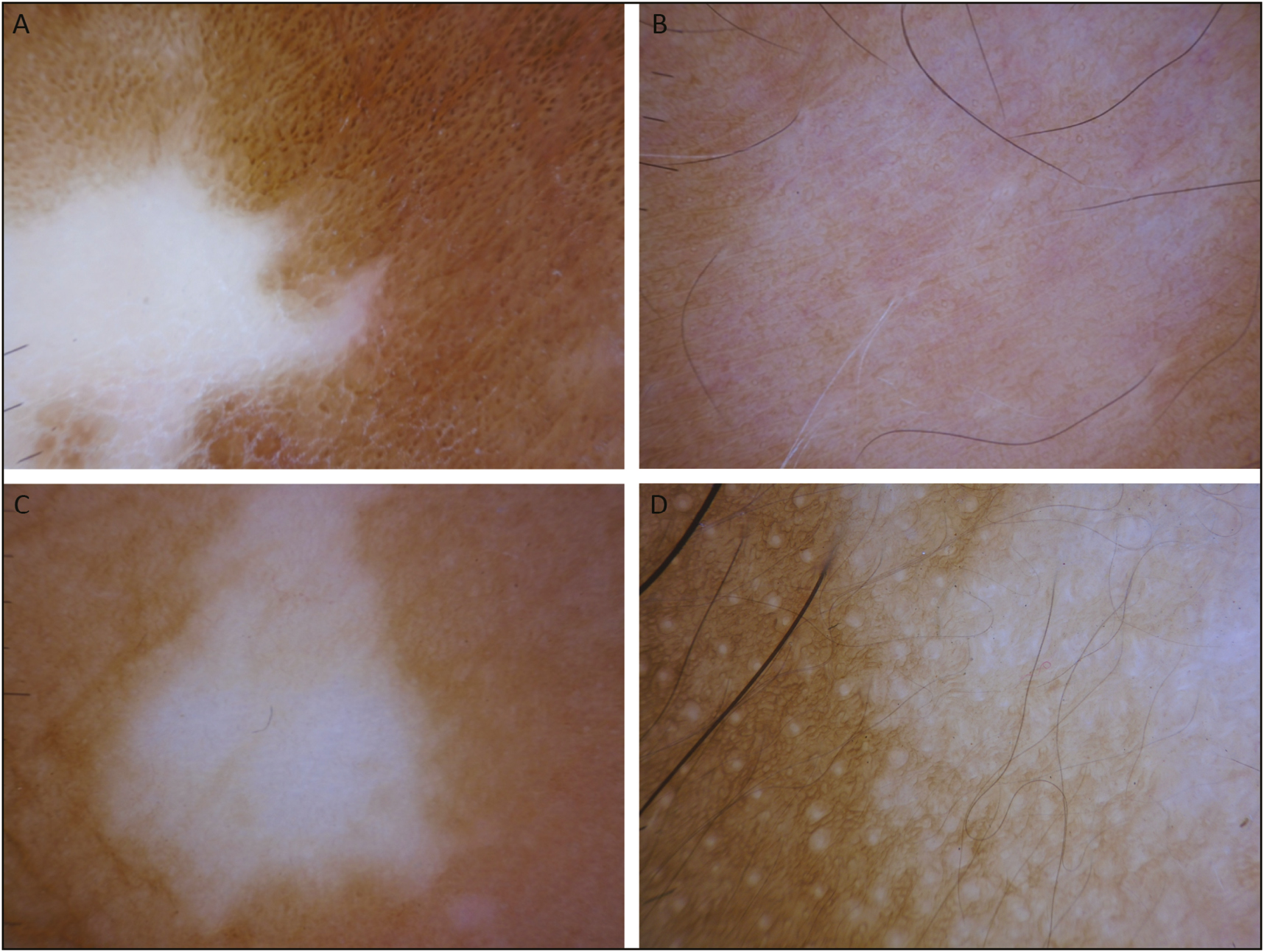
- Pigment network within the vitiligo lesion. (A) Absent. (B) Reticular. (C) Reduced. (D) Reverse
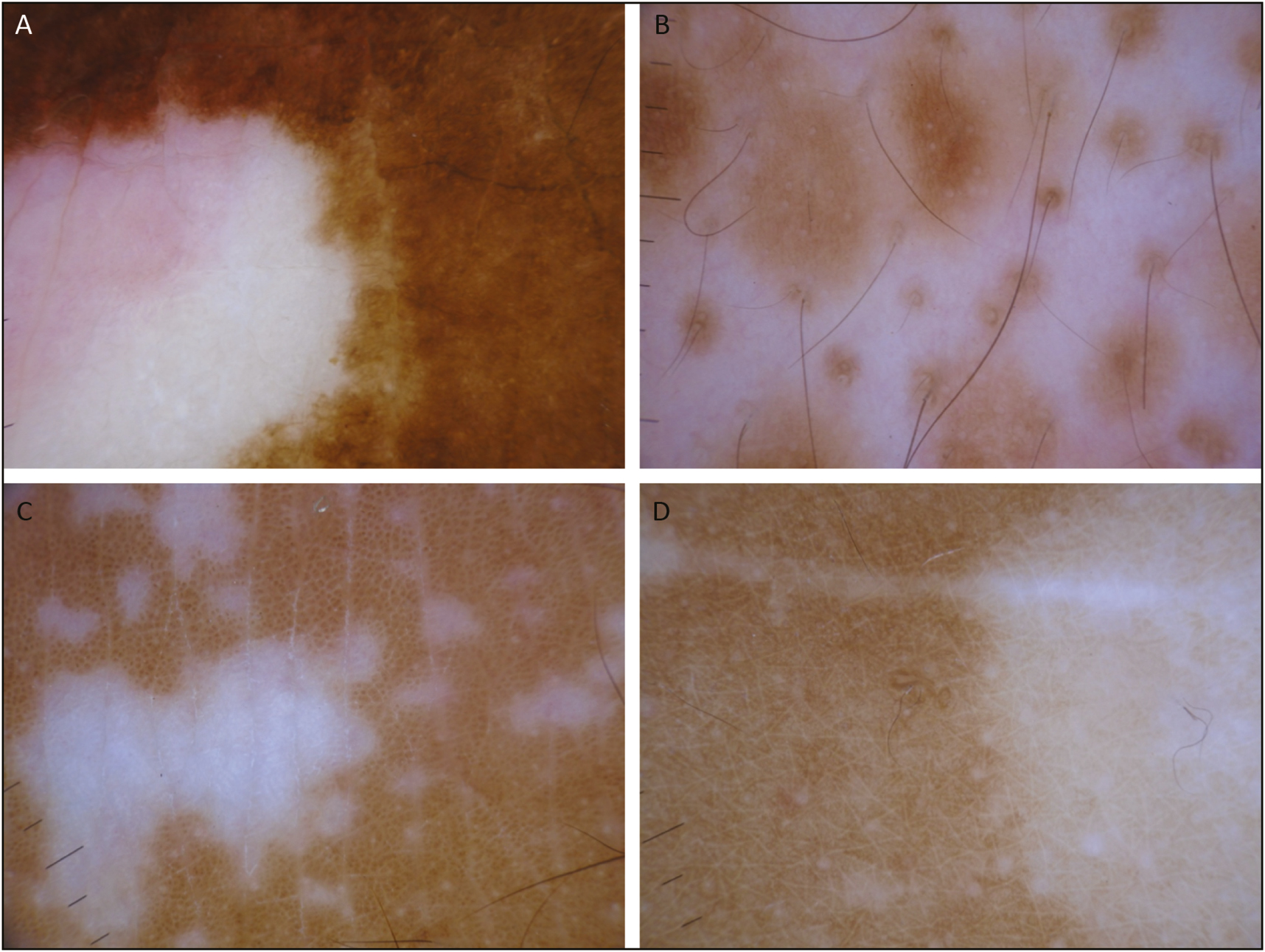
- (A) Perilesional hyperpigmentation. (B) Perifollicular pigmentation. (C) Satellite lesions. (D) Micro-Koebner phenomenon
Statistical analysis
Categorical data were summarized as counts and percentages. Numerical variables were summarized as mean and standard deviation, if normally distributed and median with range or interquartile range, if non-normally distributed. Chi-square test was used to test association between categorical variables. Sensitivity and specificity were calculated with 95% confidence interval (CI). A subjective score was assigned to each of the six dermatoscopic parameters as shown in Table 1, and the final score was computed for the stability of the vitiligo. To predict the quantitative assessment of stability of the six dermatoscopic parameters score against the Wood’s lamp, a receiver operating characteristic (ROC) curve was plotted and the area under the receiver operating characteristic curve (AUROC) and its 95% CI were calculated The statistical analysis was performed using STATA software, version 13.0 (StataCorp, College Station, Texas).
| No. | Dermatoscopic parameters | Score |
|---|---|---|
| 1. | Border (sharp) | +1 |
| 2. | Pigment network (absent/reticulate) | +1 |
| 3. | Perilesional hyperpigmentation | +1 |
| 4. | Perifollicular pigmentation | +1 |
| 5. | Satellite lesion | –1.5 |
| 6. | Micro-Koebner phenomenon | –2 |
RESULTS
Patient demographics
A total of 85 patients with a clinical diagnosis of vitiligo participated in the study comprising 45 males (52.9%) and 40 females (47.1%). They belonged to the age group of 16–64 years. One hundred and thirty-one lesions were analyzed in these 85 patients. A total of 52 lesions had a stable vitiligo disease activity (VIDA) score of –1 or 0, whereas the rest 79 lesions had unstable VIDA score of 1+ to 4+.
Wood’s lamp findings
Sixty lesions were stable under Wood’s lamp, having achromic with sharply defined borders. A total of 71 lesions were unstable under evaluation with Wood’s lamp, which had hypopigmented with poorly defined borders and trichrome in 66 and 5 lesions, respectively.
Dermatoscopic parameters evaluation
Absence of satellite lesions and absence of micro-Koebner phenomenon are the most sensitive markers of stable vitiligo with a sensitivity of 99.6% and 100%, respectively. Presence of sharp border and absent/reticulate pigment network within the vitiligo patch are the most specific markers with a specificity of 100% and 96.8%, respectively [Table 2].
| No. | Dermatoscopic parameters | Sensitivity | Specificity | PPV | NPV | LR+ | LR– | LR+/LR– |
|---|---|---|---|---|---|---|---|---|
| 1. | Border (sharp) | 94.1% | 100% | 100% | 95.5% | - | 0.254 | - |
| 2. | Pigment network (absent/reticulate) | 92.9% | 96.8% | 96% | 94.3% | 21.8 | 0.3 | 181 |
| 3. | Perilesional hyperpigmentation | 89.2% | 85.4% | 84% | 90.2% | 5.15 | 0.443 | 29.1 |
| 4. | Perifollicular pigmentation | 66.5% | 81.4% | 73.6% | 75.6% | 2.63 | 1.13 | 5.01 |
| 5. | Absence of satellite lesion | 99.6% | 34% | 60.8% | 98.6% | 1.43 | 0.618 | - |
| 6. | Absence of micro-Koebner | 100% | 11.9% | 55.9% | 100% | 1.1 | - | - |
PPV = positive predictive value, NPV = negative predictive value, LR = likelihood ratio
LR value of 1 indicates that the tests provide no additional information and LR above or below 1 increases or decrease the likelihood of stable vitiligo, respectively.
Scoring for stability in vitiligo and its prediction against Wood’s lamp
A subjective score of +1 was ascertained to each of the four positive predictors of stability, namely, border (sharp), pigment network (absent/reticulate), perilesional pigmentation, and perifollicular pigmentation. The negative predictors of stability, namely, satellite lesions and micro-Koebner phenomenon were given a score of –1.5 and –2, respectively [Table 1]. The AUROC of stability in vitiligo [Figure 4] had a better discrimination against the Wood’s lamp assessment (AUROC, 0.95; 95% CI: 0.90–0.99). Using a cutoff more than or equal to a total score of 1.5 in the stability score of vitiligo had a sensitivity of 90% and a specificity of 94.4% against the Wood’s lamp assessment [Table 3].
| Cutoff point | Sensitivity | Specificity | Correctly classified |
|---|---|---|---|
| ≥ –3.5 | 100.00% | 0.00% | 45.80% |
| ≥ –1.5 | 100.00% | 4.23% | 48.09% |
| ≥ –0.5 | 100.00% | 11.27% | 51.91% |
| ≥0 | 98.33% | 19.72% | 55.73% |
| ≥0.5 | 93.33% | 66.20% | 78.63% |
| ≥1 | 93.33% | 69.01% | 80.15% |
| ≥1.5 | 90.00% | 94.37% | 92.37% |
| ≥2 | 88.33% | 94.37% | 91.60% |
| ≥3 | 75.00% | 100.00% | 88.55% |
| ≥4 | 16.67% | 100.00% | 61.83% |
| >4 | 0.00% | 100.00% | 54.20% |
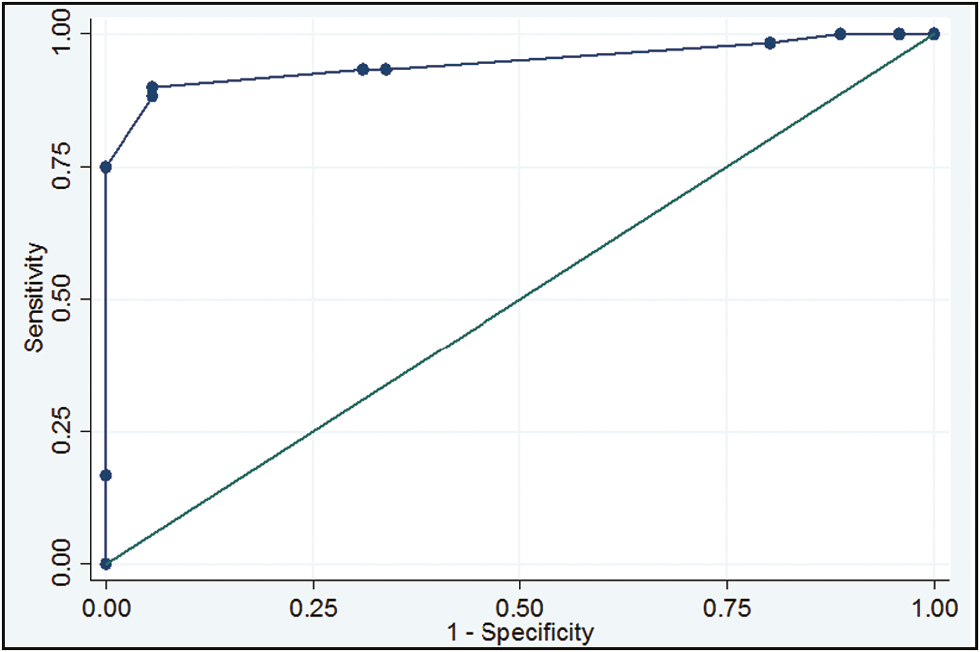
- Receiver operating characteristic (ROC) curve: Area under ROC curve = 0.95 (95% CI = 0.90–0.99)
DISCUSSION
The diagnosis of vitiligo is primarily clinical. Dermatoscopy in vitiligo is useful to highlight subtle features invisible to naked eye. Very few studies of dermatoscopy in vitiligo are available. Dermatoscopy was found useful in differentiating vitiligo from other hypopigmentary disorders and in the diagnosis of early vitiligo, blue vitiligo, and trichrome vitiligo.[678910] As far as dermatoscopy of stability of the disease before vitiligo surgery is concerned, perifollicular hyperpigmentation, marginal hyperpigmentation, and marginal reticular pigmentation were the findings associated with stability. Trichrome, star burst, polka dot, salt and pepper, and comet tail appearance were seen in active disease. Chandrashekhar[11] cited the need for standardization and further validation of these findings concerning stability of vitiligo.
Benzekri et al.[12] proposed that Wood’s lamp examination allowed reliable evaluation of activity of vitiligo correlating in both histology and immunohistology. Achromic with sharply defined borders was considered stable showing lesser CD8 T cells in the epidermis. Lesions with inflammatory raised border, trichrome, and hypopigmented with poorly defined border showed CD8 T cells in clusters close to the melanocytes, indicating disease activity. Wood’s lamp is a simple validated bedside examination to ascertain the activity of vitiligo.[13] Dermatoscopy allows for further qualification of the vitiligo lesions. The six dermatoscopic parameters analyzed in our study include border, pigment network, perilesional hyperpigmentation, perifollicular pigmentation, satellite lesion, and micro-Koebner phenomenon.
Sharply defined border denoting stable vitiligo had the highest specificity in our study followed by absent or reticulate pigment network within the vitiligo patch. Reverse pigment network earlier described in melanoma, Spitz nevus and melanocytic nevi,[14] is a very useful dermatoscopic finding to detect early unstable vitiligo.[15] Melanocytes are present in higher number per unit area in the slope of rete ridges as compared to the tip of rete ridges, which contribute to the reticular pattern seen with the dermatoscope in normal skin, with netlike pattern corresponding to the slope and pale areas corresponding to the tips of rete ridges. In rapidly evolving vitiligo, the loss of melanocytes results in the lightening of the pigment network more than the pale areas, resulting in negative pigment network. It was seen in only 2.3% of our cases, which is lesser than that described by Thatte et al.[16] Perilesional hyperpigmentation had high sensitivity (89.2%) and specificity (85.4%) for stability, which is in line with previous studies.[1718] Retention of perifollicular pigmentation, which was considered characteristic of stable vitiligo by Chuh and Zawar,[19] did not show significant correlation with stability in our study (P = 0.251) with lower sensitivity (66.5%). However, perifollicular pigmentation had a relatively higher specificity of 81.4% pointing out that absence of which indicates unstable vitiligo. This is similar to a case report[20] where perifollicular depigmentation under dermatoscopy was found to be a sign of impending vitiligo. Satellite lesions are small white blotches around the main patch of vitiligo, which give a “tapioca sago” appearance.[21] Micro-Koebner phenomenon is the occurrence of isomorphic depigmented streaks along the line of trauma around the main vitiligo patch, showing “comet tail” appearance.[22] Absence of satellite lesions and absence of micro-Koebner phenomenon were the most sensitive dermatoscopic parameters indicating stability with a sensitivity of 99.6% and 100%, respectively.
Limitation of our study is that histopathology was not performed. Considering the fact that Wood’s lamp findings were already validated against histopathological and immunohistochemical findings,[1223] it was taken as gold standard and dermatoscopic findings were validated against it in our study.
CONCLUSION
Dermatoscope is a useful handheld tool to evaluate the activity of vitiligo and to detect subtle changes. A vitiligo patch is considered stable in the presence of sharp border, absent pigment network, reticulate pigment network, perilesional hyperpigmentation, and perifollicular pigmentation and in the absence of satellite lesions and micro-Koebner phenomenon. A cutoff score of more than or equal to 1.5 using the “BPLeFoSK criteria” indicates stability of a lesion of vitiligo.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Possible patterns of epidermal melanocyte disappearance in nonsegmental vitiligo: a clinicopathological study. Br j Dermatol. 2015;172:331-6.
- [Google Scholar]
- Psychiatric morbidity in vitiligo: prevalence and correlates in India. j Eur Acad Dermatol Venereol. 2002;16:573-8.
- [Google Scholar]
- Surgical treatment of vitiligo: why, when and how. j Eur Acad Dermatol Venereol. 2003;17:518-20.
- [Google Scholar]
- How unstable is the concept of stability in surgical repigmentation of vitiligo? Dermatology. 2000;201:182-3.
- [Google Scholar]
- Is lesional stability in vitiligo more important than disease stability for performing surgical interventions? Results from a multicentric study. j Cutan Aesthet Surg. 2016;9:13-9.
- [Google Scholar]
- Dermoscopy in the differentiation of idiopathic guttate hypomelanosis (IGH) In: Khopkar U, ed. Dermoscopy and trichoscopy in diseases of the brown skin: atlas and short text. New Delhi, India: Jaypee Brothers Medical Publishers; 2012. p. :97-103.
- [Google Scholar]
- Dermoscopy: differentiating evolving vitiligo from a hypopigmented patch of leprosy. In: Khopkar U, ed. Dermoscopy and trichoscopy in diseases of the brown skin: atlas and short text. New Delhi, India: Jaypee Brothers Medical Publishers; 2012. p. :112-3.
- [Google Scholar]
- Dermoscopy in general dermatology: a practical overview. Dermatol Ther (Heidelb). 2016;6:471-507.
- [Google Scholar]
- Nail trichrome vitiligo: case report and literature review. Br j Dermatol. 2013;168:668-9.
- [Google Scholar]
- Dermoscopy: a tool to assess stability in vitiligo. In: Khopkar U, ed. Dermoscopy and trichoscopy in diseases of the brown skin: atlas and short text. New Delhi, India: Jaypee Brothers Medical Publishers; 2012. p. :112-3.
- [Google Scholar]
- Clinical features and histological findings are potential indicators of activity in lesions of common vitiligo. Br j Dermatol. 2013;168:265-71.
- [Google Scholar]
- Three cases of reverse pigment network on dermatoscopy with three distinctive histopathologic diagnoses. Dermatol Surg. 2013;39: 818-20.
- [Google Scholar]
- “Reversed pigmentary network pattern” in evolving lesions of vitiligo. Indian Dermatol Online j. 2015;6:222-3.
- [Google Scholar]
- The utility of dermoscopy in the diagnosis of evolving lesions of vitiligo. Indian j Dermatol Venereol Leprol. 2014;80:505-8.
- [Google Scholar]
- Application of polarized light dermoscopy in the early diagnosis of vitiligo and its differential diagnosis from other depigmented diseases. Chin J Dermatol. 2009;42:810-3.
- [Google Scholar]
- A panoramic study of dermascopic patterns in vitiligo. Medpulse—Int Med J. 2016;3:436-9.
- [Google Scholar]
- Demonstration of residual perifollicular pigmentation in localized vitiligo—a reverse and novel application of digital epiluminescence dermoscopy. Comput Med Imaging Graph. 2004;28:213-7.
- [Google Scholar]
- Novel dermoscopic findings of perifollicular depigmentation and evolving leukotrichia in areas of clinically unaltered pigmentation: an early predictive sign of impending vitiligo! Pigment Int. 2014;1:28-30.
- [Google Scholar]
- Dermoscopy—a tool to assess stability in vitiligo. Int J Contemp Med Res. 2017;4:2066-8.
- [Google Scholar]




