
Translate this page into:
Facial Blanching after Local Anesthesia Injection: Clinico-anatomical Correlation—Review of Literature
Address for correspondence: Dr. Saeedeh Khajehahmadi, Dental Research Center, Mashhad University of Medical Sciences, Vakilabad Boulevard, Mashhad, Iran. E-mail: khajehahmadis@mums.ac.ir
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Facial blanching as a complication of local anesthesia is reported in dentistry. Inadvertent arterial penetration and subsequent vasospasm has been accepted as the mechanism of this phenomenon. Most cases occur after inferior alveolar nerve block injection. In this article, five cases are reported after Gow-Gates injection, maxillary nerve block via greater palatine foramen, inferior alveolar nerve block, and maxillary buccal infiltration. It is the largest case series in this topic. Also, clinico-anatomical correlation between facial–mucosal blanching and the site of intra-arterial injection is explained. To the best of our knowledge, partial blanching of the face subsequent to buccal infiltration is reported for the first time in this article. Cutaneous surgeon should be aware of this complication and should not carry out unnecessary treatment.
Keywords
Blanching
local anesthesia
vasospasm

INTRODUCTION
Inadvertent intra-arterial injection of local anesthesia in maxillofacial region has subjective and objective symptoms: dizziness, light-headedness, palpitation, vision alternation, diplopia, burning sensation, and facial blanching.[123] Most of these complications are reported during inferior alveolar nerve block, but they can occur in every intraoral injection, when the local anesthesia is injected into the lumen of artery.[45] The blanching follows certain principles:
CASE PRESENTATION
Case 1
The patient was a 28-year-old woman without any systemic disease. She attended for the removal of mandibular right wisdom tooth. On the basis of palpitation report, plain mepivacaine had been used. Gow-Gates injection was used for this purpose, and immediately after injection, blanching occurred in the infraorbital, buccal, and palatal regions [Figure 1].

- Facial, buccal, and palatal blanching after Gow-Gates injection
Case 2
The patient was a 25-year-old man and ASA class I [Figure 2]. Mandibular inferior alveolar nerve block (Halsted’s technique) and long buccal nerve were used for dental implant insertion in the mandibular right quadrant. Facial blanching and palatal–buccal mucosa whitening occurred.

- Facial blanching and palatal whitening after inferior alveolar nerve block injection
Case 3
The patient was a 63-year-old man who attended for right maxillary sinus lift procedure. On the basis of previous heart problems, epinephrine was not used in the local anesthetic cartridge. Maxillary block injection from greater palatine canal approach was used for obtaining profound anesthesia. Facial and palatal blanching occurred immediately after the injection, and the patient felt burning and itching sensation on the face [Figure 3].
- (A) Facial blanching and (B) palatal ischemia after maxillary nerve block via greater palatine canal
Case 4
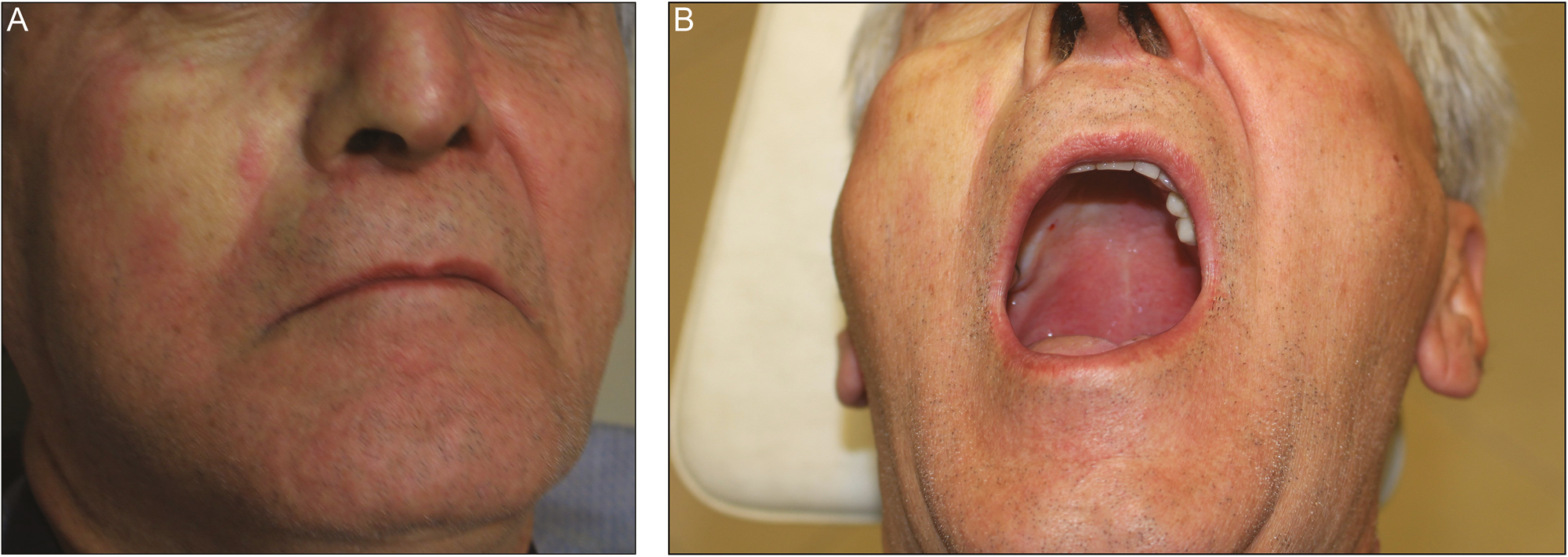
The patient was a 22-year-old woman who referred for mandibular right wisdom tooth removal. Lidocaine 2% and epinephrine 1:80,000 were used for inferior alveolar nerve block. Facial, buccal, and palatal blanching occurred on the side of injection. She felt numbness in the periorbital and lower lip. The color of the face returned to preinjection condition after 10minutes [Figure 4].
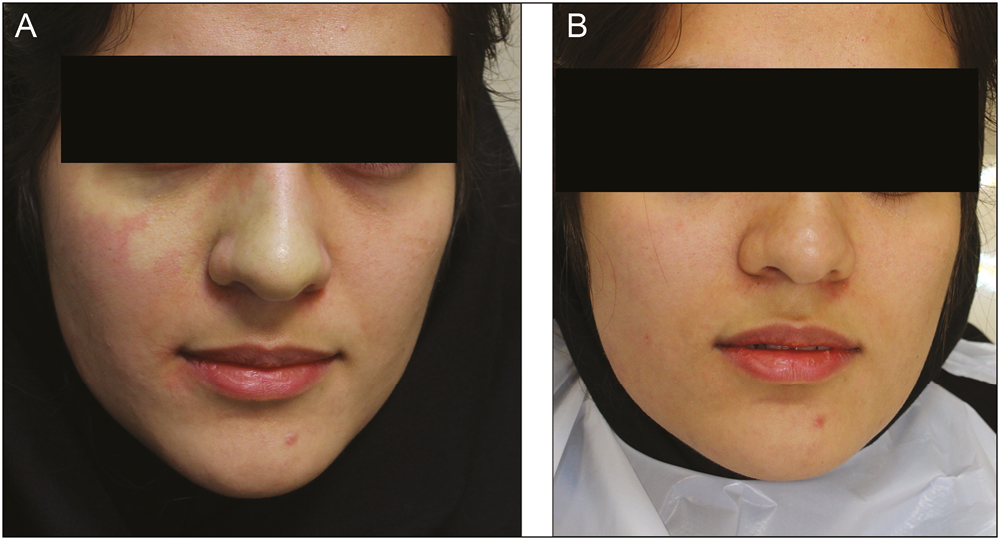
- (A) Facial blanching immediately after inferior alveolar nerve block injection and (B) 10 minutes later
Case 5
A 32-year-old female patient in healthy conditions attended for extraction of second maxillary right premolar. Immediately after buccal infiltration, a white patch appeared lateral to the nasolabial fold [Figure 5].
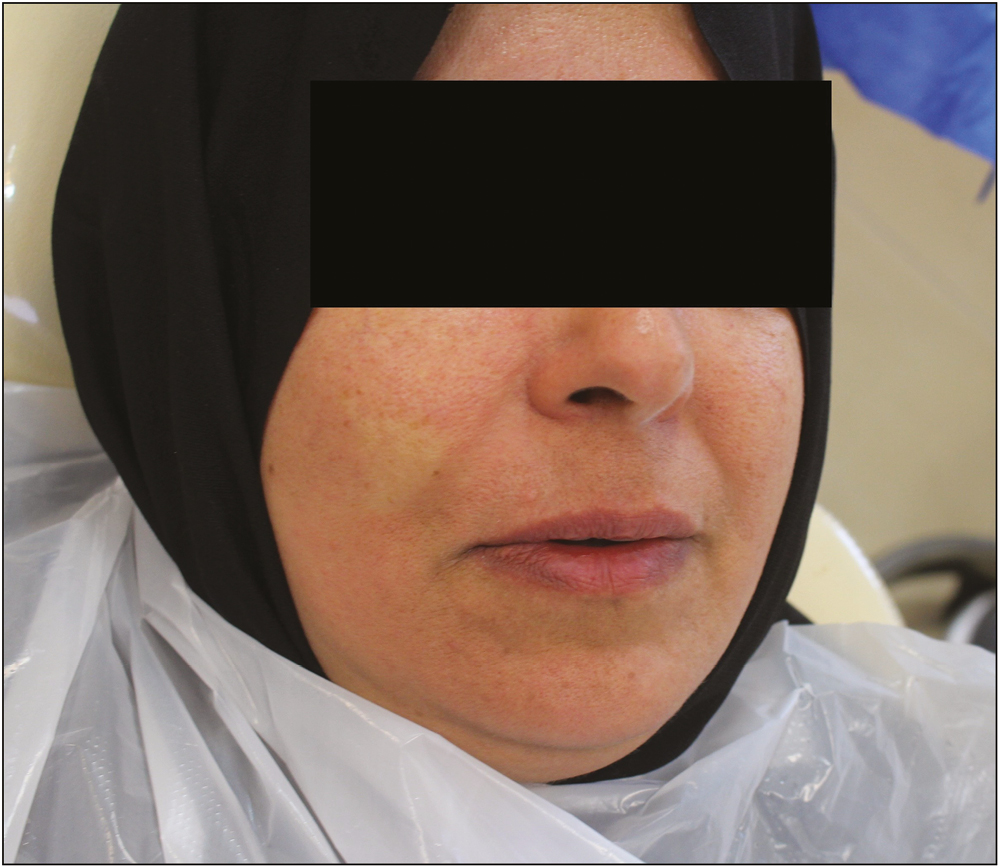
- Partial blanching of the face subsequent to buccal infiltration for extraction of maxillary second premolar
DISCUSSION
Intra-arterial injection of local anesthesia in dentistry occurs most commonly in inferior alveolar nerve block injection.[10] In this article, five cases have been reported, where in two cases, other injections caused reversible facial–mucosal blanching. Other causes of facial blanching include neurotoxin (botulinum toxin) injection, intravascular injection of cosmetic fillers, and superpotent topical corticosteroids.[111213]
In oral cavity, every artery is at the risk of intra-arterial injection. Maxillary artery (proximal segment) is penetrated in Gow-Gates injection, especially if the loop variant of proximal segment is present.[14] Greater palatine artery injection was the reason for facial and palatal blanching in the third case [Figure 6].
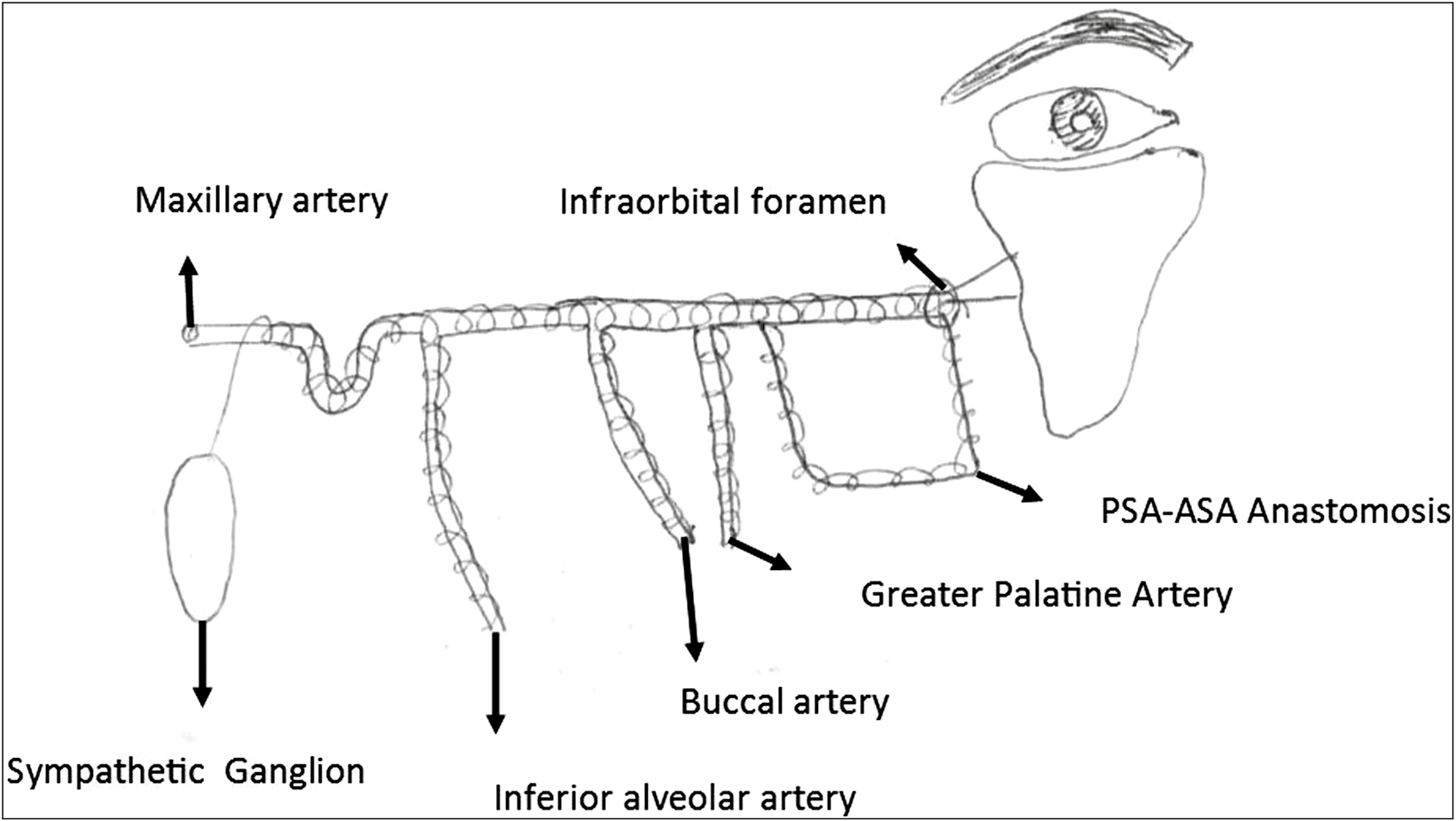
- Diagram of maxillary artery and its branches, sympathetic nerve, and facial blanching in infraorbital area (PSA, Posterior Superior Alveolar artery; ASA, Anterior Superior Alveolar artery)
Lower frequency of administering maxillary nerve block and inherent low incidence of positive aspiration in Gow-Gates conduction nerve block are the reasons for low reported facial blanching after these injections.[1516]
Vasoconstrictors are not necessary for facial blanching. In two cases (1 and 3), plain mepivacaine had been used.
Mucosal blanching occurs in the distribution of buccal, greater palatine, and soft tissue posterior superior alveolar artery but not in the arterial distribution of inferior alveolar artery. Inferior alveolar artery terminates to the mental artery and nourishes the lower lip chin and alveolar mucosa.[17] Anastomosing branches between submental and inferior alveolar artery within the mandible may compensate for the hypoxic effect of inferior alveolar artery spasm. Thus, lower lip blanching did not occur in the case where maxillary artery proximal segment or inferior alveolar artery was penetrated.[18] The size of the blanching area on the face depends on the presence and percentage of infraorbital artery terminal branches (zygomaticomalar, nasal, and superior vestibular arteries). Existence of anastomosis with angular and transverse facial arteries is the other important factor.[1920]
In PubMed search for local anesthesia and blanching, the majority of reported cases were young individuals. In our report, 1 of 5 cases had an age past the third decade of life. This may be attributed to the impaired sympathetic control of the peripheral cutaneous vascular system.[21]
Facial blanching is not always accompanied by positive aspiration. This and the fact that local anesthesia failure was not observed in reported cases in this article suggest that the contact of the needle with the perivascular sympathetic plexus or bypass of the artery by the needle is sufficient for triggering facial blanching. In the case of positive aspiration in the inferior alveolar nerve block and numbness in skin pallor area, other theories should be considered.
With selection of local anesthetic techniques in less vascular regions, risk of this complication can be reduced.
Cutaneous surgeon should be aware of this complication of local anesthesia because this phenomenon also occurs after extraoral injection of local anesthesia. Transient nature of facial blanching after local anesthesia injection differentiates it from facial blanching after injection of cosmetic fillers. The latter needs prompt treatment with hyaluronidase, topical nitro pastes, and warm compress.[22]
Anxiety for the patient and physician and unnecessary treatments may occur if the surgeon is not familiar with this complication.
CONCLUSION
Periorbital and palatal whitening is the constant feature of the blanching subsequent to inadvertent arterial penetration in intraoral local anesthetic block techniques. Mucosal blanching in the distribution of buccal artery occurs in Gow-Gates mandibular nerve block as well as inferior alveolar nerve block injections.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Complications of local dental anesthesia and anatomical causes. Ann Anat. 1999;181:105-6.
- [Google Scholar]
- Complications of an intra-arterial injection from an inferior alveolar nerve block. J Am Dent Assoc. 2001;132:1702-4.
- [Google Scholar]
- Intense, instantaneous, and shooting pain during local anesthesia for implant surgery. J Craniofac Surg. 2018;29:2287-90.
- [Google Scholar]
- Facial blanching after inferior alveolar nerve block anesthesia: an unusual complication. J Dent Anesth Pain Med. 2017;17:317-21.
- [Google Scholar]
- Blanching of facial skin after infiltration of local anaesthetic: an unusual complication of inadvertent intra-arterial injection. Br J Oral Maxillofac Surg. 2016;54:1051-2.
- [Google Scholar]
- An unusual complication of an inferior dental nerve block: a case report. Br Dent J. 2009;206:9-10.
- [Google Scholar]
- Avoiding complications in local anesthesia induction: anatomical considerations. J Am Dent Assoc. 2003;134:888-93.
- [Google Scholar]
- Reflex vasoconstriction following dental injections. Oral Surg Oral Med Oral Pathol. 1987;63:542-4.
- [Google Scholar]
- Topographic anatomy of the infraorbital artery and its clinical implications for nasolabial fold augmentation. Plast Reconstr Surg. 2018;142:273e-80e.
- [Google Scholar]
- Skin and mucosal ischemia as a complication after inferior alveolar nerve block. Dent Res J (Isfahan). 2016;13:560-3.
- [Google Scholar]
- Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34:584-600.
- [Google Scholar]
- Facial blanching due to neurotoxins: proposed mechanisms. Dermatol Surg. 2013;39:24-9.
- [Google Scholar]
- Proximity of the maxillary artery to the mandibular ramus: an anatomic study using three-dimensional reconstruction of computer tomography. Clin Anat. 2014;27:691-7.
- [Google Scholar]
- Maxillary nerve block—a new approach using a computer-controlled anesthetic delivery system for maxillary sinus elevation procedure. A prospective study. Quintessence Int. 2004;35:477-80.
- [Google Scholar]
- Incidence of positive aspiration in the Gow-Gates mandibular block. Anesth Pain Control Dent. 1992;1:73-6.
- [Google Scholar]
- Age changes in the human inferior alveolar artery—a histological study. Br J Oral Maxillofac Surg. 1989;27:371-4.
- [Google Scholar]
- Anastomosis between the inferior alveolar artery branches and submental artery in human mandible. Surg Radiol Anat. 2006;28:308-10.
- [Google Scholar]
- The infraorbital artery: from descriptive anatomy to mucosal perforator flap design. Head Neck. 2019;41:2065-73.
- [Google Scholar]
- Sympathetic control of reflex cutaneous vasoconstriction in human aging. J Appl Physiol (1985). 2015;119:771-82.
- [Google Scholar]
- Facial blanching after cutaneous injections: cannulation of branches of the ophthalmic artery. Case series and review of the literature. Dermatol Surg. 2011;37:530-5.
- [Google Scholar]




