
Translate this page into:
Botulinum Toxin for Paramedian Interpolated Forehead Flaps
Address for correspondence: Dr. Matthew James Lin, 234 East 85th Street, 5th Floor, New York, NY 10028, USA. E-mail: matthew.lin@mountsinai.org
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
The forehead skin closely resembles the texture and color of the midface region. As such, the use of a paramedian forehead flap to repair a midface defect provides optimal cosmesis; however, the donor forehead site may be left with an undesirable scar in a highly visible region of the face. Cutaneous surgeons possess a variety of traditional techniques intended to minimize scarring. We have found that the addition of 50 units of botulinum toxin at the time of wound closure has improved scar outcomes for patients undergoing reconstruction with paramedian interpolated flaps. Possible mechanisms for the efficacy of botulinum toxin lie in its ability to chemically paralyze the frontalis muscle and glabella complex. This immobilization leads to a reduction in unwanted wound tension during the most vulnerable first few days of healing.
Keywords
Botulinum toxin
interpolated flap
Mohs micrographic surgery
neuromodulators
paramedian forehead flap
reconstructive surgery
scar

INTRODUCTION
The interpolated paramedian forehead flap is one of the most dependable flaps for midface reconstruction.[1] The forehead provides a source of skin that is an excellent color and texture match to the nasal skin. The forehead skin is also extremely versatile, as removal of muscle and subcutaneous fat from the distal portion of the flap renders it thin and pliable. The skin can then be easily contoured to fit any defect of the mid or lower nose area. The pedicle of the flap centers on the supratrochlear artery, which supplies the flap with an abundant and reliable blood supply even in patients with vascular disease. This vigorous blood supply can also help revascularize underlying cartilage grafts.
The advantages of the forehead flap are somewhat offset by the large linear vertical scar left at the donor site. These scars are cosmetically challenging, as the forehead is a highly visible convex location and is composed of thick, dynamic, and sebaceous skin. The inferior portion of the forehead flap is under less tension due to the narrow pedicle at this site, but the superior portion of the forehead flap may span several centimeters. Most donor-site forehead scars are satisfactory; however, with the increase in patient demand for scar minimization, other methods to further reduce scarring should be considered.
INNOVATION
Excessive wound tension is a key factor in the development of less-favorable forehead scars because it promotes inflammation, prolongs erythema, and contributes to scar widening. Forehead scars in particular are constantly under stress, as the muscles of facial expression pull and stretch the overlying skin throughout the course of the day. The frontalis muscle and glabella complex are particularly strong and expressive muscle groups that may contribute to suboptimal forehead donor-site scars.
Given the impact of tension on wound healing, cutaneous surgeons seek to minimize tensile distracting forces that can pull and distort the immature scar. Undermining, suture method, layered closure, adhesive tape, and physical immobilization are a few of the techniques used to reduce this undesirable tension.
Botulinum toxin also has the potential to reduce unwanted force on forehead wounds by chemically paralyzing the underlying frontalis and glabella complex muscles. This has led us to routinely use botulinum toxin off-label at the donor site on the forehead to reduce wound tension and, ultimately, improve scar cosmesis. After appropriate oncologic clearance and obtaining patient consent, we perform flap reconstruction under local anesthesia. The pedicle base is designed to be less than 1.5cm in all cases to allow for a favorable closure of the lower forehead. The temporalis muscle is then undermined bilaterally and releasing incisions are made in the galea to reduce wound tension. The wound then undergoes a primary three-layer closure with 3-0 poliglycaprone 25, 4-0 poliglycaprone 25, and 5-0 nylon.
After placement of the cutaneous sutures, we inject onabotulinumtoxinA (1 mL = 50 units) in a standardized grid pattern consisting of 14 injections to the forehead (30 units of botulinum toxin or 0.6 mL) and 3 injections to the glabella complex (20 units of botulinum toxin or 0.4 mL) [Figures 1 and 2]. We prefer onabotulinumtoxinA to abobotulinumtoxinA due to the reduced risk of ptosis. We prefer to use doses at the higher end of the spectrum with an aim of maximal chemoimmobilization of the forehead and glabella. The delayed onset of effect of onabotulinumtoxinA may prevent us taking full advantage of the scar improvement capabilities of the neurotoxin, considering that time to immobilization of the muscle is a key factor in the improvement of wound healing with this technique. Injection of botulinum toxin days to weeks prior to elective surgery may allow more optimal muscle paralysis. Newer neurotoxins such as abobotulinumtoxinA and the type E serotype, which may have more rapid onset of action, may also provide more effective chemoimmobilization of scars.
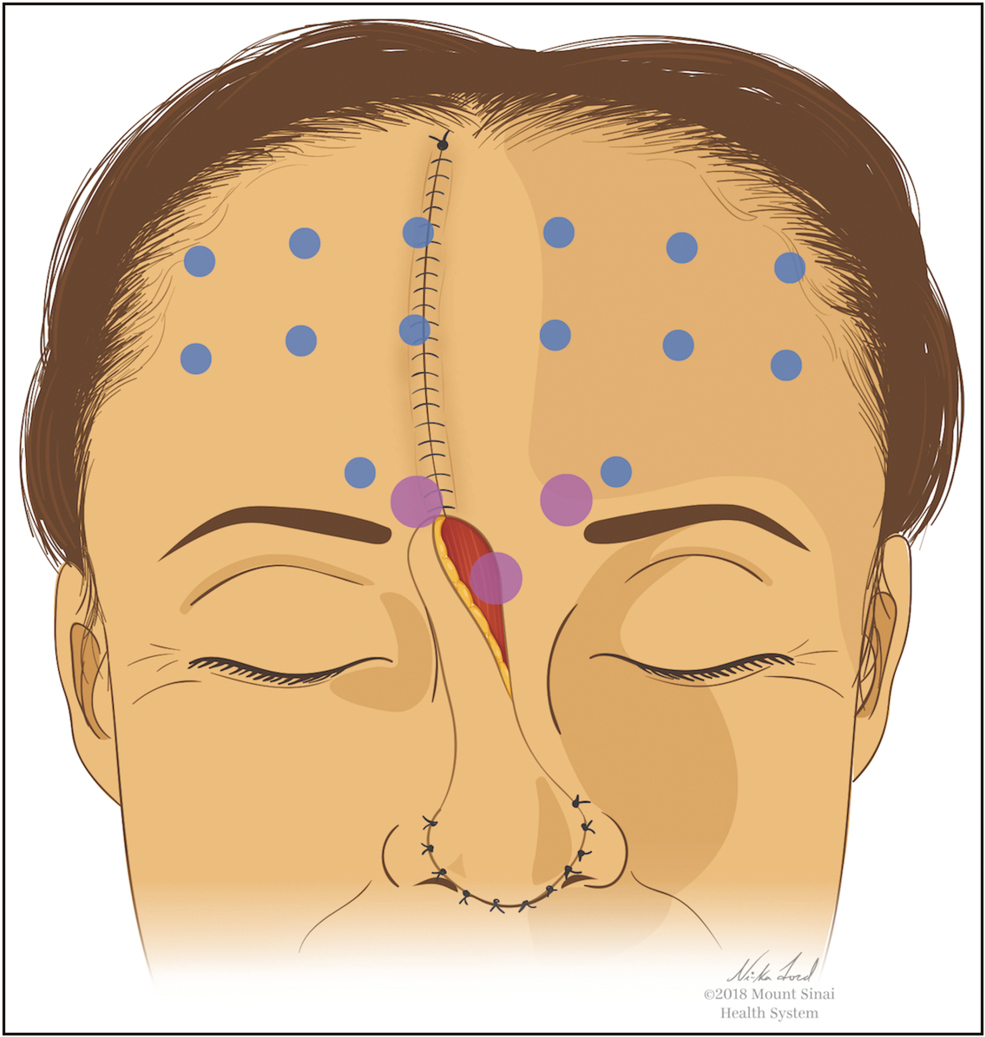
- Standardized forehead and glabella complex injection pattern for paramedian forehead flap donor scars. Reprinted with permission from Mount Sinai Health System
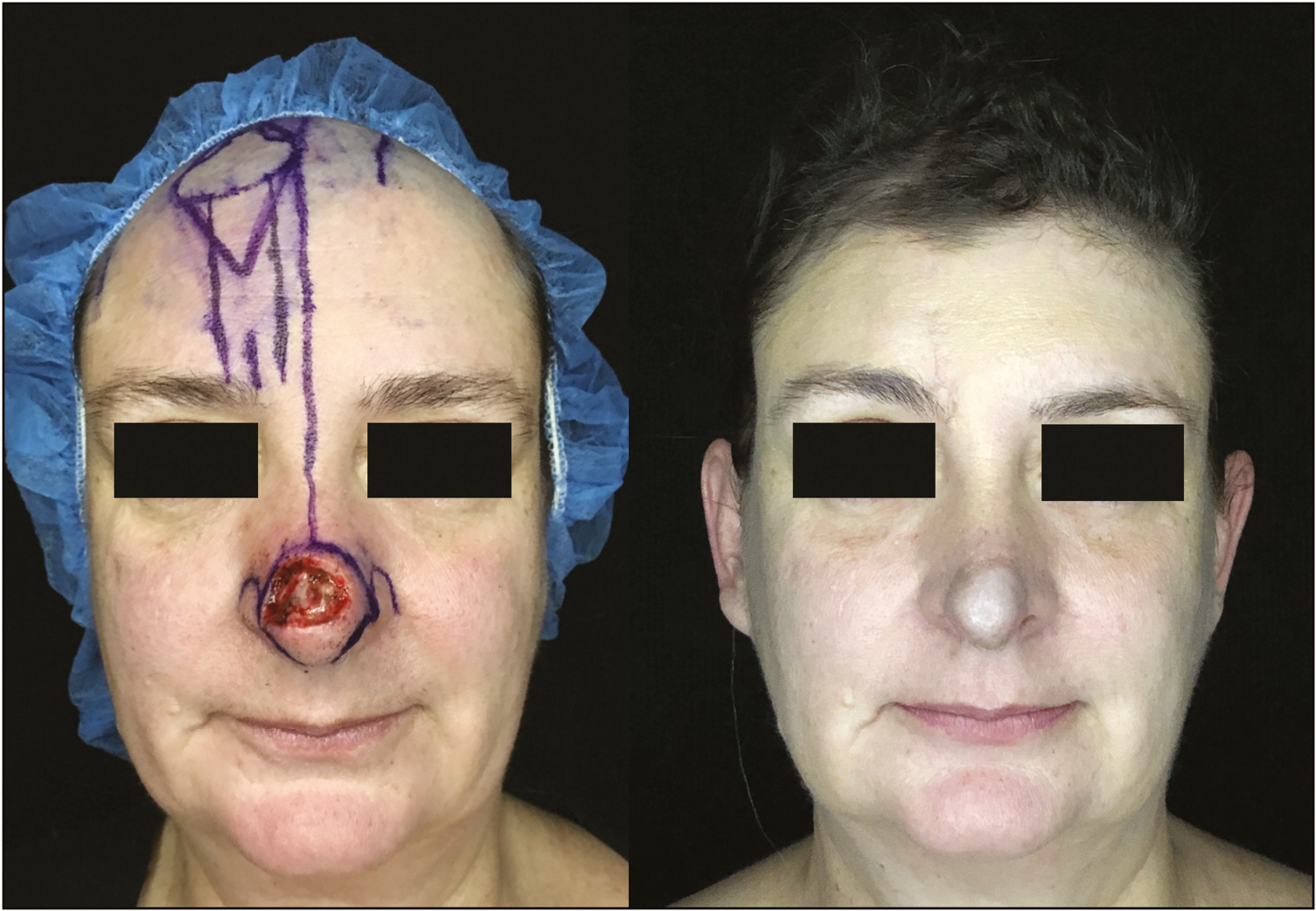
- Example of patient with large nasal tip defect reconstructed with paramedian forehead flap (left). After placement of the cutaneous sutures, onabotulinumtoxinA was injected to forehead and glabella complex according to the template shown in Figure 1. Forehead scar shown 2 months after suture removal (right)
DISCUSSION
The addition of botulinum toxin to interpolated paramedian forehead flaps has improved our scar outcomes, a finding consistent with research supporting the role of neuromodulators in improving forehead scars.[2] The excellent safety, availability, and tolerability of botulinum toxin combined with the potential to improve cosmetic outcomes render this intervention a useful adjunct to traditional scar minimization techniques.
Ethical policy and institutional review board statement
No IRB status to disclose.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We thank Ni-ka Ford, MS, Academic Medical Illustrator, Instructional Technology Group, Icahn School of Medicine at Mount Sinai, for the support in this study.
REFERENCES
- The paramedian forehead flap for nasal reconstruction: from antiquity to present. J Craniofac Surg. 2019;30:330-3.
- [Google Scholar]
- Use of intraoperative botulinum toxin in facial reconstruction. Dermatol Surg. 2009;35:182-8.
- [Google Scholar]




