
Translate this page into:
Keloid Scars Arising after Follicular Unit Extraction Hair Transplantation
Address for correspondence: Dr. Nabeel Kadhim Alhamzawi, Department of Dermatology, Al Diwaniyah Teaching Hospital, Diwaniyah, Iraq. E-mail: alhamzawi_n@yahoo.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Hair transplantation is considered safe compared to other cosmetic procedures. However, scarring is still an inevitable potential complication. Keloid scarring is a rare complication of hair transplantation and usually associated with strip harvesting rather than follicular unit extraction (FUE). A case of keloids at the donor site following FUE hair transplantation is presented. Hair transplant practitioners should be aware of the risks of the procedure when considering hair restoration to ensure safer outcomes.
Keywords
Donor area
follicular unit extraction
hair transplantation
keloids

INTRODUCTION
Hair transplantation is an aesthetic surgery procedure that has developed considerably but is not free of risks and potential complications. The two popular modern hair transplantation techniques are follicular unit transplant (FUT) or strip harvesting and follicular unit extraction (FUE). The development of FUE represented a significant advance in this procedure.[1] Several complications have been reported after hair transplantation, with severity depending on the degree of trauma and surgical invasion. Although FUE is minimally invasive, complications, such as ecchymosis, infection, and edema, may occur in the acute postoperative stage. Other complications, such as donor site depletion, pinpoint scarring, buried graft, and overharvesting, may develop later.[2] Keloid scarring is rare following hair transplantation and more often associated with strip harvesting than FUE. Two published reports of keloids following hair transplantation describe the predicting factors and how to avoid them.[34] Keloids that developed after FUE are usually present in the form of dot-like, not linear, as in the current case. This is the second case that is reported following FUE, the first one was reported in 2017. Keloids develop due to exaggerated immune response to healing, which may be provoked by faulty surgical technique or poor patient compliance. This report presents keloids developed after FUE and discusses preventive measures.
CASE HISTORY
A 35-year-old man presented with multiple red raised lesions on the posterior aspect of the scalp of 8-month duration. The lesions were associated with pain, especially on sleeping, scalp washing, and combing. The patient reported a history of hair transplantation of FUE type 1 year prior, after which inflammation and itching developed at the donor areas. A few weeks later, hypertrophic red lesions arose at the same sites.
On examination, seven linear scars ranging from 2 to 4 cm in length were located on the posterior aspect of the scalp behind the right ear [Figure 1]. An additional three linear scars in the occipital region ranged from 3 to 4 cm [Figure 2]. The lesions had a pink color and firm consistency, and their thickness measured approximately 0.5 cm (using a caliper). On palpation, tenderness was highly significant. The recipient site showed no folliculitis or cobblestoning. The clinical examination showed that there were no previous similar lesions on his body, and no signs of Ehlers–Danlos syndrome found.

- Extensive keloids developed on the donor area after follicular unit extraction hair transplantation
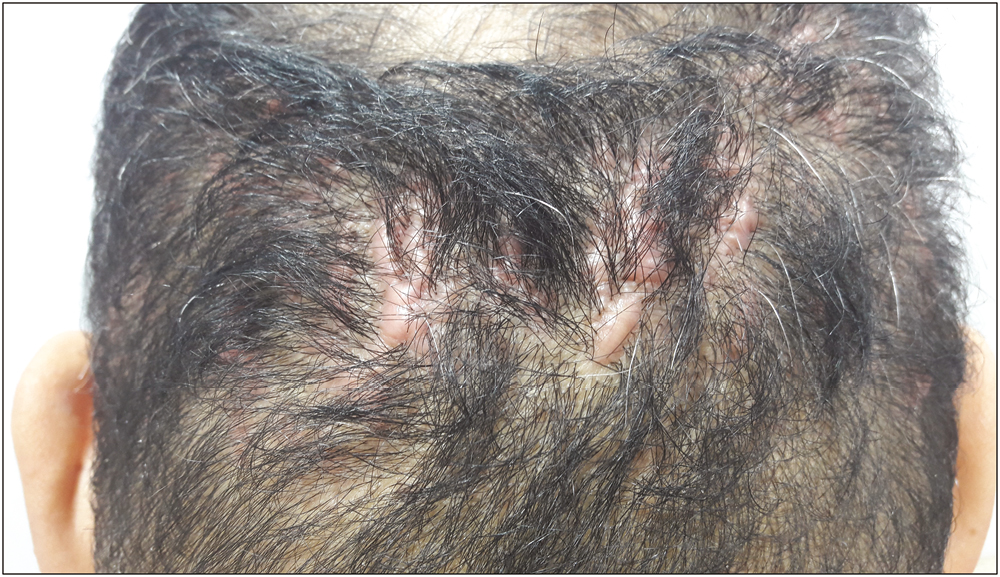
- Same patient with keloids on the occipital region
On the basis of the clinical appearance of the lesions and history of trauma at the same sites, the diagnosis of keloids developed after FUE hair transplantation was determined. The patient was prescribed topical silicone gel sheeting with an intralesional corticosteroid. Each keloid was injected with triamcinolone acetonide (TAC) 40 mg/mL at a dose of 0.1 mL/cm per lesion. The treatment was repeated every 3 weeks. An acceptable regression in the size of keloid was noticed after four sessions.
DISCUSSION
A keloid is an exuberant scar that extends beyond the boundaries of the traumatic or surgical wound. It may even form spontaneously on the mid-chest in the absence of any injury. Keloids, unlike hypertrophic scars, persist for an extended time and do not regress spontaneously. They appear as mildly tender or pruritic, firm, and pink to purple, with a well-demarcated outline plaque.[5] Keloids develop as a result of abnormal cellular response to trauma. Patients with multiple keloids are more likely to have a positive family history, suggesting the possibility of genetic predisposition.[6] The chest, upper back, shoulders, and earlobes are common sites of keloid formation. Certain ethnicities are considered at higher risk, particularly African–American, Latino, and Asian individuals.[7] The rarity, in this case, is the appearance of keloids on the scalp after minimally invasive FUE hair transplant in a patient with no previous history of keloid formation, which confirms the difficulty of predicting keloid occurrence.
Hair transplantation is considered a permanent solution for the bald areas of androgen alopecia. For best results, strip harvesting and hair implantation should be performed by qualified, well-trained practitioners. Further, the risk of keloids should be addressed in considering hair restoration, as it is difficult to anticipate keloid formation after FUE, even in people without risk. A test transplant may be beneficial. Arocha described a process of taking a few follicles from a hidden donor site and waiting up to 9 months to be sure that keloids do not develop, before proceeding with the hair transplant.[8]
FUE has some advantages over FUT or strips excision. The minimal dermal injury created by FUE makes it less likely to induce keloid formation. However, it requires excellent hand-eye coordination, physical stamina, and a longer learning curve.[9]
FUE harvests follicular units with a small punch, usually 0.8–1.1 mm in diameter. This modality creates round scars, which are often hypopigmented and more prominent than the original punch size.[10] Accordingly, this case may result from the use of a hefty punch to harvest many follicular units in a short time.
The use of platelet-rich plasma (PRP) with or without extracellular matrix material, especially that derived from the porcine bladder, can assist in rapid wound healing and reduce scar formation.[1011] However, keloids remain challenging to treat, despite advanced therapeutic strategies. It is thus preferable to prevent keloids by minimizing risk factors as much as possible. To achieve the best results, the surgeon must do the following:
Select candidates without susceptibility to keloids (no personal or family history)
Remember that people with dark skin are at higher risk than those with fair skin
Have basic knowledge of the anatomy of skin and hair, and wound healing
Minimize injury by using a micro-punch tool for harvesting individual follicles
Inject PRP or Fibrin Rich Plasma at the wound area to help promote rapid healing and minimize scarring
Diagnose and treat keloids early
Administer postoperative steroid injections in suspected cases
Keep the wound moisturized to prevent the scar from desiccation that may induce itching
Instruct the patient to avoid sunlight exposure and use sunscreen when needed. Sunscreens protect the injured skin from ultraviolet rays, which induce more inflammation that interferes with the natural healing process and create further thickening and darkening of scar
CONCLUSION
Keloid formation after hair transplant surgery is unpredictable. Hence, preventive measures are preferable to minimize the risks. Hair transplant practitioners should be aware of the potential complications of the procedure when considering hair restoration to ensure safer outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Extensive keloids following hair transplantation. J Dermatol Surg Oncol. 1990;16:867-9.
- [Google Scholar]
- Extensive donor site keloids in follicular unit extraction hair transplantation. Int J Trichology. 2017;9:127-9.
- [Google Scholar]
- Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 2011;17:113-25.
- [Google Scholar]
- Keloids and scars: a review of keloids and scars, their pathogenesis, risk factors, and management. Curr Opin Pediatr. 2006;18:396-402.
- [Google Scholar]
- How do keloids factor into hair restoration? Available from: https://arochahairrestoration.com/hair-restoration/how-do-keloids-factor-into-hair-restoration/.
- [Google Scholar]
- Hair restoration surgery: challenges and solutions. Clin Cosmet Investig Dermatol. 2015;8:361-70.
- [Google Scholar]
- The basement membrane component of biologic scaffolds derived from extracellular matrix. Tissue Eng. 2006;12:519-26.
- [Google Scholar]




