
Translate this page into:
Acquired Periungual Fibrokeratoma Looks like a Supernumerary Digit: An Uncommon Soft Tissue Tumor
Address for correspondence: Dr. Mohd Altaf Mir, Department of Burns and Plastic Surgery, All India Institute of Medical Sciences, Rishikesh 249203, Uttarakhand, India. E-mail: draltafmir@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Acquired digital fibrokeratoma is an uncommon, benign fibrous tumor that usually occurs in adults as a solitary lesion with a typical size of less than 1 cm. We present a case with periungual growth and nail plate deformity. The growth was completely excised after raising the epinychial flap and the fold was reconstructed. The histological results confirmed the digital fibrokeratoma. The rarity of digital fibrokeratoma and its unique morphological appearance of the tumor makes it interesting. Acquired periungual fibrokeratoma, an uncommon benign fibrous tumor of an unknown etiology, typically found at the distal end of the digits, may present with nail plate deformation due to chronic pressure, and in order not to damage the matrix, the tumor should be excised carefully, which can cause permanent nail dystrophy. In addition, we emphasize the importance of ruling out other causes of abnormal growths and of considering fibrokeratoma during differential diagnoses.
Keywords
Periungual fibrokeratoma
soft tissue tumor
supernumerary digit

INTRODUCTION
Nail is an anatomical region of aesthetic significance and conditions affecting the nail are often social embarrassment especially for the females. Acquired periungual fibrokeratoma is a benign and uncommon soft tissue tumor,[12] mostly of unknown etiology. However, trauma is considered a cause in few cases.[3] The lesion is usually 3–5 mm in size.[4] However, when more than 1 cm, it is called giant fibrokeratoma.[14,5] The histopathological features are consistent with fibrokeratoma.[6] There are only few cases reported in plastic and reconstructive surgery literature. Here we report one such case of periungual fibrokeratoma.
CASE REPORT
A 32-year-old lady presented to the outpatient office room of the first author at his previous institution with a painless 12-mm small fingerlike growth arising under the epinychium deforming the nail plate of right ring finger [Figure 1]. She had been aware of the lesion for 2 years, and she was having difficulty in wearing the ornament (ring) in the same digit and was feeling embarrassed at social gatherings. She had not been aware of any trauma in the digit. Formal informed consent for the procedure, clinical photography, and publication for academic purposes was taken from the patient. The epinychial flap is marked and raised. The lesion is excised completely without damage to the nail matrix. The epinychial flap is repositioned back. The histopathology confirmed the diagnosis of fibrokeratoma evidenced by fibroepithelial lesion with collagenous stroma containing fibroblasts arranged in parallel to the axis of the lesion and ectatic vessels, and the tumor cells consist of monomorphic spindled fibroblast with bipolar mitosis in the center arranged in a storiform pattern extending into the epidermis, which is attenuated and has subcutaneous fat [Figure 2]. The patient nail and epinychial fold appeared normal after 9 months [Figure 3], and now she has no problem in wearing the ornament (ring) and she attends social gatherings without any embarrassment.

- Fingerlike growth (12 mm) of right ring finger and tourniquet application and marking for epinychial flap raising
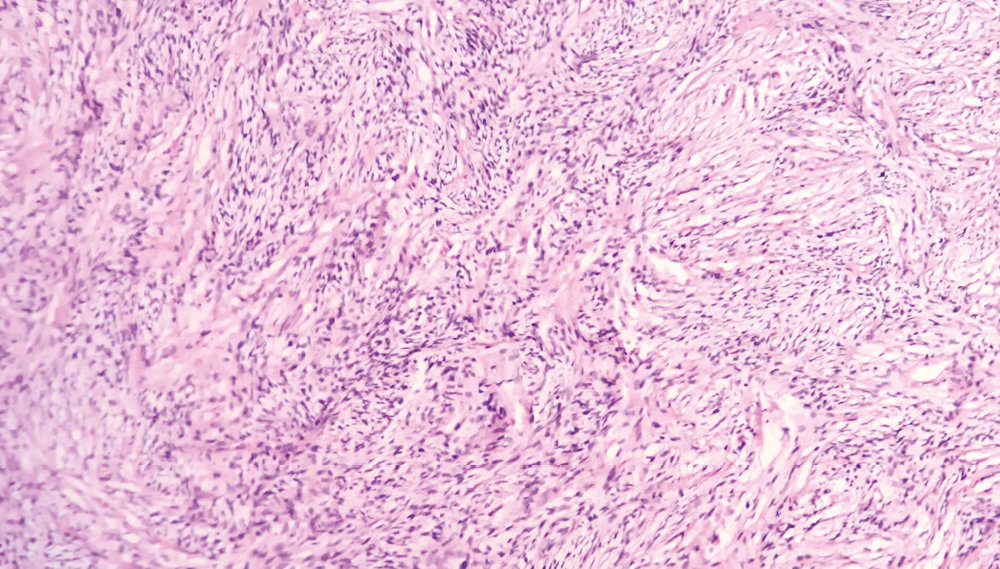
- Low power view microphotograph showing tumor composed of plump spindle cells arranged in a storiform pattern (×100, hematoxylin and eosin)

- Final outcome of nail and its folds after 9 months of follow-up
DISCUSSION
The rarity of digital fibrokeratoma and its unique morphological appearance of the tumor makes it interesting. The acral fibrokeratoma is an uncommon benign tumor of fibrous tissue as described by Bart et al.,[6] in 1968, however, periungual fibrokeratoma is rare.[7] The most accepted hypothesis is the trauma suggested by the acral localization. Koenen tumors are a type of digital fibrokeratoma occurring in tuberous sclerosis. The lesion is usually 3–5 mm in size.[4] However, when more than 1 cm, it is called giant fibrokeratoma,[14,5] a fingerlike projection, which arises at around the nail folds, partially overlapping the nail plate. They are rarely large to the extent that they can destroy the nail. The histopathology diagnosis of fibrokeratoma is characterized by fibroepithelial lesion with collagenous stroma containing fibroblasts arranged in parallel to the axis of the lesion and ectatic vessels. The tumor cells consist of monomorphic spindled fibroblast with bipolar mitosis in the center arranged in a storiform pattern. The treatment of choice is the complete excision because local recurrence after partial excision or curettage may occur. In order not to damage the matrix, the tumor should be excised carefully, which can cause permanent nail dystrophy.
The dermatosurgeon should perform the digital nerve block with lignocaine 2%, exsanguinate finger using glove cut, and roll proximally from tip to base of the digit, which acts as digit tourniquet and prevents bleeding and provides clean field. While raising the epinychial flap and excising the tumor, utmost care should be taken not to damage the nail matrix to prevent deformed new nail.
Here we report one case of periungual fibrokeratoma, which is very rare, as we could find only one such similar case reported so far in the literature of plastic surgery.[8] This condition should never be ignored while considering differential diagnoses of soft tissue tumors around the nail.[7]
CONCLUSION
Acral periungual fibrokeratoma is an uncommon benign fibrous tumor of an unknown etiology, typically found at the distal end of the digits, which may present with nail plate deformation due to chronic pressure, and in order not to damage the matrix, the tumor should be excised carefully, which can cause permanent nail dystrophy. In addition, we emphasize the importance of ruling out other causes of abnormal growths and considering fibrokeratoma during differential diagnoses.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
I acknowledge Dr. Anureet Kour, MD Pathology and Associate Professor, at the institution where this case was presented. She has provided the pathological confirmation report and micropathological photographs.
REFERENCES
- Giant acquired digital fibrokeratoma occurring on the left great toe. Ann Dermatol. 2011;23:64-6.
- [Google Scholar]
- An unknown mass: The differential diagnosis of digit tumors. Int J Dermatol. 2015;54:1214-25.
- [Google Scholar]




