
Translate this page into:
The Dermoscopy of Pigmented Basal Cell Carcinoma
Address for correspondence: Dr. Boina Kinnera, PG Hostel, Opposite Government General Hospital, Kakinada 533001, Andhra Pradesh, India. E-mail: kinneraboina@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor
The pigmented basal cell carcinoma (BCC) is not uncommon in brown skin, and dermatoscopy has been shown to enhance BCC detection, by facilitating its discrimination from other skin tumors and inflammatory skin diseases. Pigmentation is present in more than 50% of the BCC in skin of color, whereas less than 10% of BCCs in fair-skinned individuals are pigmented.[1]
A 50-year-old woman presented with single asymptomatic dark-colored lesion over left cheek since 2 years. The lesion started as small pinhead-sized lesion, which gradually progressed to attain present size. Examination revealed single, well-defined, hyperpigmented, and firm plaque of size 4 cm × 2 cm with ulceration [Figure 1]. Dermoscopy (DermLite DL4, magnification ×10, and polarized light) revealed absence of pigmentary network, peripheral maple leaf–like structures, blue-gray structureless areas, multiple spoke wheel–like structures, blue-white veil, adherent fabric fibers, brown dots, erosions, and adherent and shiny white chrysalis-like structures [Figure 2]. Histopathology showed multiple islands of basaloid cells with peripheral palisading and melanin clumps [Figures 3 and 4]. The diagnosis of pigmented BCC was made on clinical, dermoscopic, and histopathological findings.

- Asymptomatic plaque on left cheek
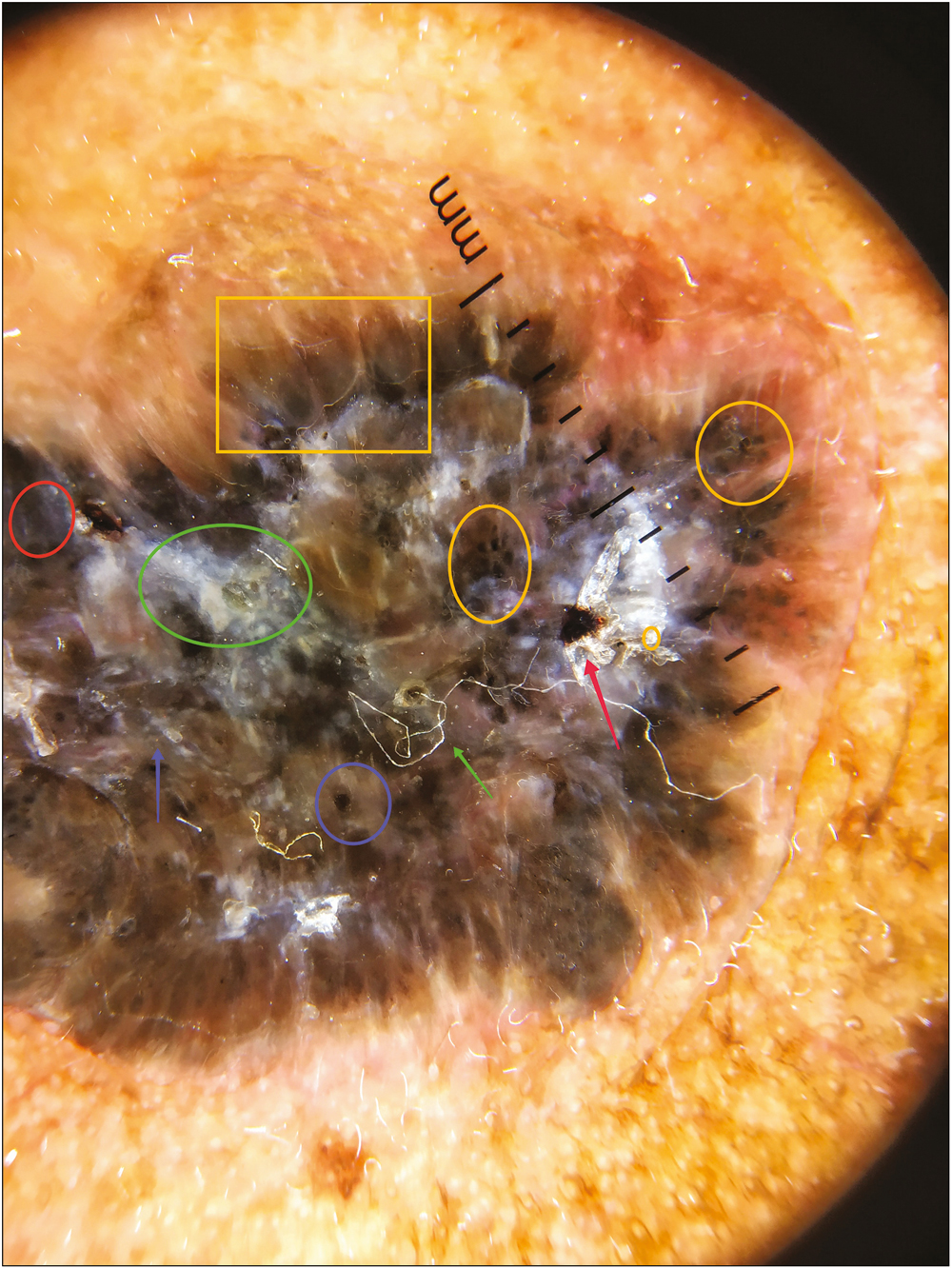
- Dermoscopy showing the absence of pigmentary network, peripheral maple leaf–like structures (yellow square), blue-gray structureless areas (red circle), multiple spoke wheel–like structures (yellow circles), blue-white veil (green circle), adherent fabric fibers (green arrow), brown dots (purple circle), erosions (red arrow), and adherent and shiny white chrysalis-like structures (purple arrow)
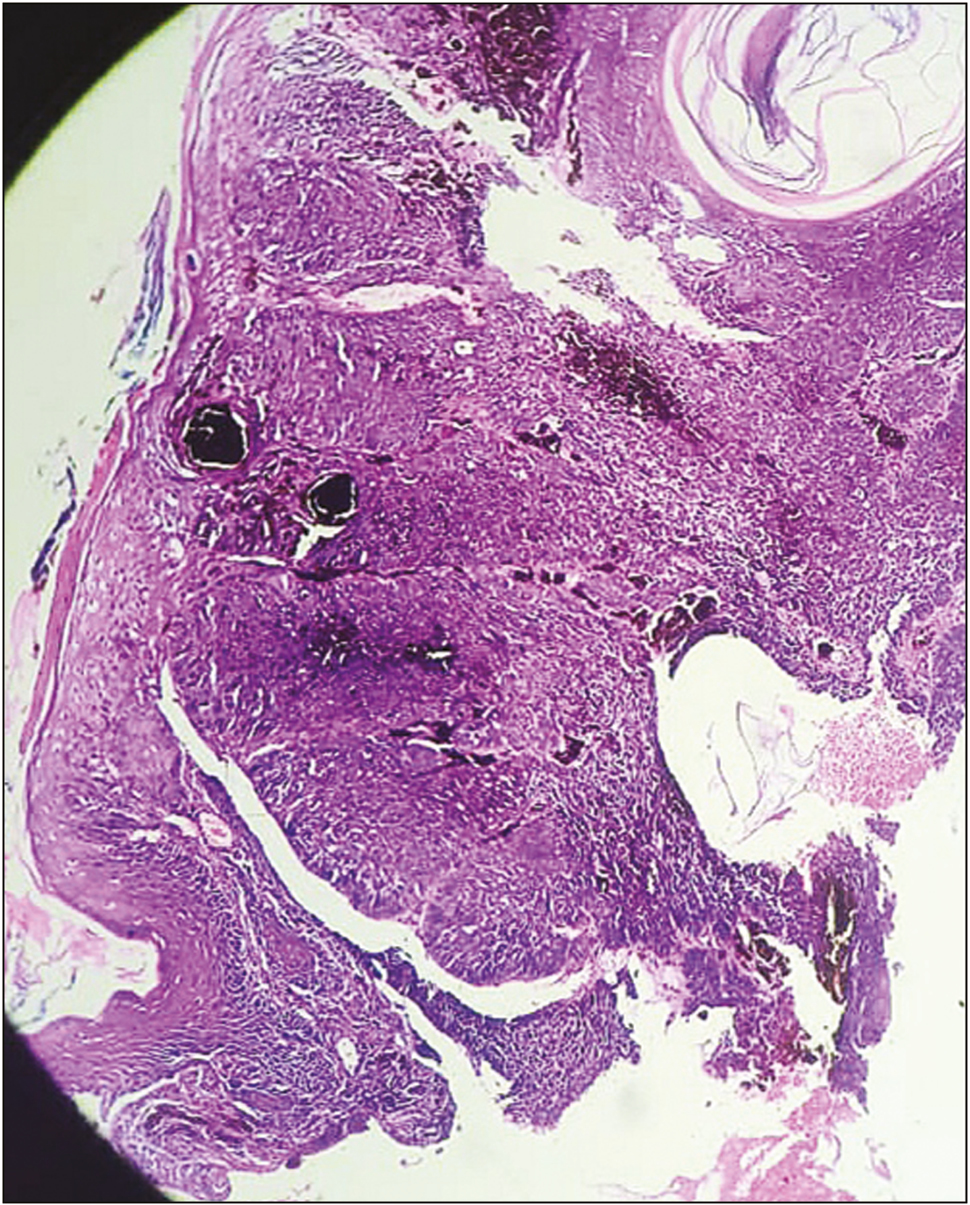
- Histopathology showing basaloid islands in dermis and retraction clefts
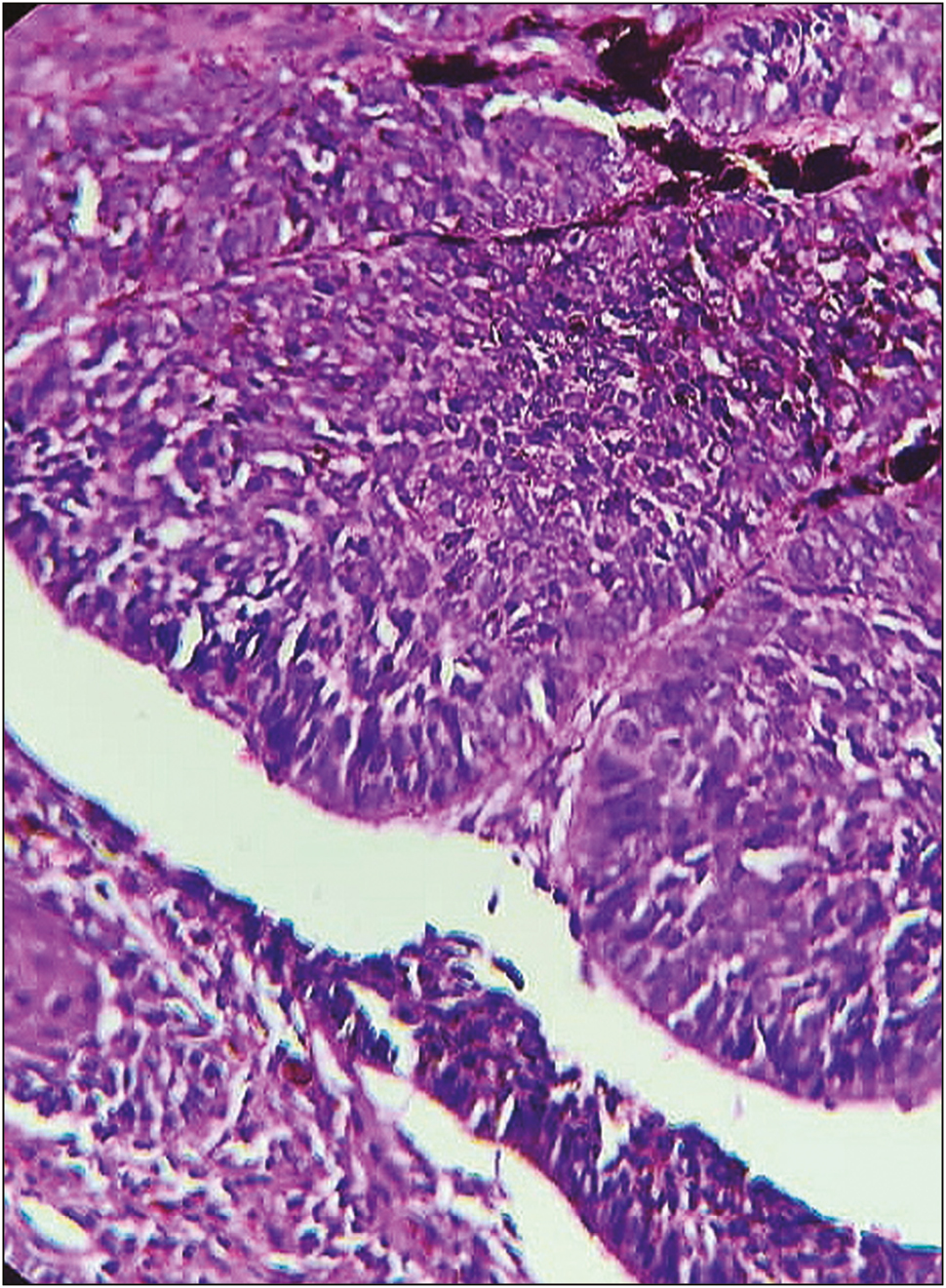
- Histopathology showing palisading basaloid cells and retraction clefts
BCC is the most common type of skin cancer in the world. Although mortality related to BCC is negligible, BCCs can be associated with significant morbidity, especially if left untreated and/or if discovered when they have attained relatively large diameters. Clinically, BCC can present with a variety of morphologies, ranging from erythematous patches to ulcerated nodules. There are multiple histopathologic subtypes of BCC. It has been shown that dermoscopy improves the diagnostic accuracy of BCC, with a sensitivity of 98.6% and diagnostic probability of 99%.[2]
According to the model designed by Altamura et al.,[3] the diagnosis of pigmented BCC by dermoscopy is based on the absence of pigment network and the detection of one of the six positive criteria: arborizing vessels, ulceration, large blue-gray ovoid nests, maple leaf–like areas, spoke wheel areas, or multiple blue-gray dots/globules.
Maple leaf–like areas correspond to multifocal tumor nests containing pigment aggregates, connected to each other by lobular extensions. Blue-gray globules correspond to small basal cell tumor islands in the dermis. Spoke wheel areas are due to tumor nests arising and connected to the epidermis.[2] Chrysalis-like structures are shiny, white, orthogonal linear streaks, which are prominent under polarized dermoscopy.[4] White streaks are formed due to the presence of collagenous stroma and fibrosis in the dermis.[3] The vascular structures such as arborizing vessels and short fine telangiectasias are less common in pigmented BCCs than those in nonpigmented BCCs. The brown dots correspond to free pigment deposition along the dermoepidermal junction and/or melanophages and/or small aggregates of pigmented neoplastic cells in the papillary and reticular dermis.[2]
The diagnosis of BCC should not be based on a single feature but on a set of dermoscopic features in combination with the clinical context. Histopathology is often essential, and produces the final and decisive diagnosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The dermatoscopic universe of basal cell carcinoma. Dermatol Pract Concept. 2014;4:11-24.
- [Google Scholar]
- Dermatoscopy of basal cell carcinoma: morphologic variability of global and local features and accuracy of diagnosis. J Am Acad Dermatol. 2010;62:67-75.
- [Google Scholar]
- Observation of chrysalis structures with polarized dermoscopy. Arch Dermatol. 2009;145:618.
- [Google Scholar]




