
Translate this page into:
Autologous Fat Grafting with or without Processing: A Study in an Indian Clinical Context
Address for correspondence: Dr Harsha Vardhan, Post Graduate Department of Plastic Surgery, King George's Medical University, Napier Road Colony-2, Lucknow, Uttar Pradesh, India. E-mail: harshaok@yahoo.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Although fat grafting has become an attractive method of correction of soft tissue deficiencies, variability in results exists. As the understanding of mechanism of survival of graft improves, the concepts regarding fat grafting change. There are many ways to process the aspirated fat with no clear method superior.
Aim:
The aim of this study was to evaluate the role of processing during autologous fat transfer.
Materials and Methods:
The patients were serially divided into two groups, namely, A and B. Harvesting of lipoaspirate and injection of fat were same in both the groups. In group A, no processing was done. In group B, the fat was processed by sedimentation and injected. Patient satisfaction was assessed following the procedure and statistical analysis was done using the Mann–Whitney U-test.
Results:
Young females between 21 and 30 years formed the majority of patients who opted for fat grafting procedure. Most of the procedures were performed for defects in the face (93.3%). The most common indication of fat grafting was contour deformities, with abdomen being the most preferred donor site. The mean patients’ satisfaction following fat grafting without processing is 2.2 ± 0.68. The mean patients’ satisfaction following fat grafting with processing is 2.53 ± 0.99.
Conclusion:
There was not a statistically significant difference in patient outcomes following fat grafting, with or without processing, in terms of patient satisfaction. Autologous fat grafting was found to be a safe procedure with no significant complications.
Keywords
Autologous fat grafting
oleman
decantation
no processing
Romberg disease
For small volume soft tissue depressions
autologous fat can be transferred without processing

INTRODUCTION
The search for the ideal method to correct soft tissue defects has always been a concern for plastic surgeons. Different materials have been used as fillers.[1] A catalog of synthetic fillers is available for soft tissue correction.[2] Fat, being autologous, non-immunogenic, non-allergic, cheap, and stable, is an attractive alternative to these fillers.[3] Fat grafting although reported early in the twentieth century failed to attain widespread acceptance due to its inconsistent results.[4] In the last two decades, with new advances in techniques and instrumentation, fat transplants have become one of the most common aesthetic procedures performed in the west.[5] Despite this, there is confusion regarding the best technique of harvesting, processing, and injecting fat which has led to unpredictable and inconsistent results.[6] This study was done with the aim of studying the effects of processing on grafting in an Indian clinical context.
MATERIALS AND METHODS
This was an interventional study, performed after approval by the Institute Ethics Committee. The study was performed between June 2013 and June 2016, in a period of 3 years. The patients were explained about the study, informed consent was taken, and data were collected in preprepared proformas. Preoperative photographs were taken as per standards described by the American Association of Plastic Surgeons.[7] The patients were sequentially divided into two groups A and B. The technique of harvesting and injecting the fat grafts was identical in both the two groups.
Harvesting of fat
The commonly used donor areas were flank or lower abdomen, depending on availability of fat. The donor area was marked and infiltrated with 1% lignocaine with 1:400,000 adrenaline. Aspiration was done using a 10 cc syringe with a two-hole Coleman aspiration cannula, via a stab incision. Gentle suction was given, corresponding to 2 cc of displacement of the plunger, and fat was aspirated using a gentle to-and-fro motion. Once syringe was filled, the syringe was placed in a rack and a fresh syringe was used for further aspiration. This was done till adequate graft was harvested. Aspiration ports were allowed to heal by secondary intention. Once adequate graft was harvested, the processing was done depending on the group of the patient [Figure 1].
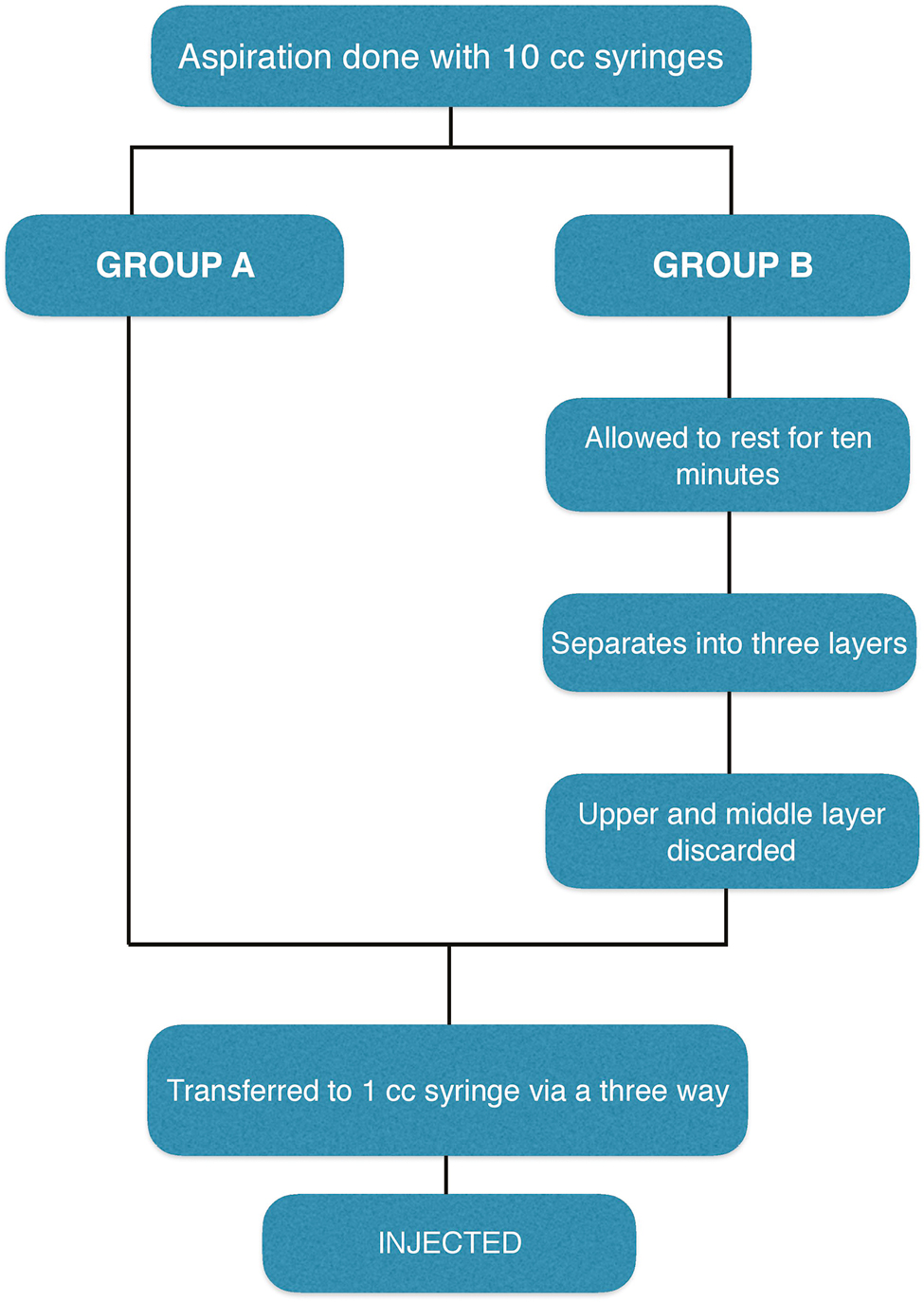
- Algorithm to denote the methodology of the study
In group A patients, fat was aspirated as described before. The aspirate was then immediately transferred into a 2 cc syringe and injected [Figure 2].
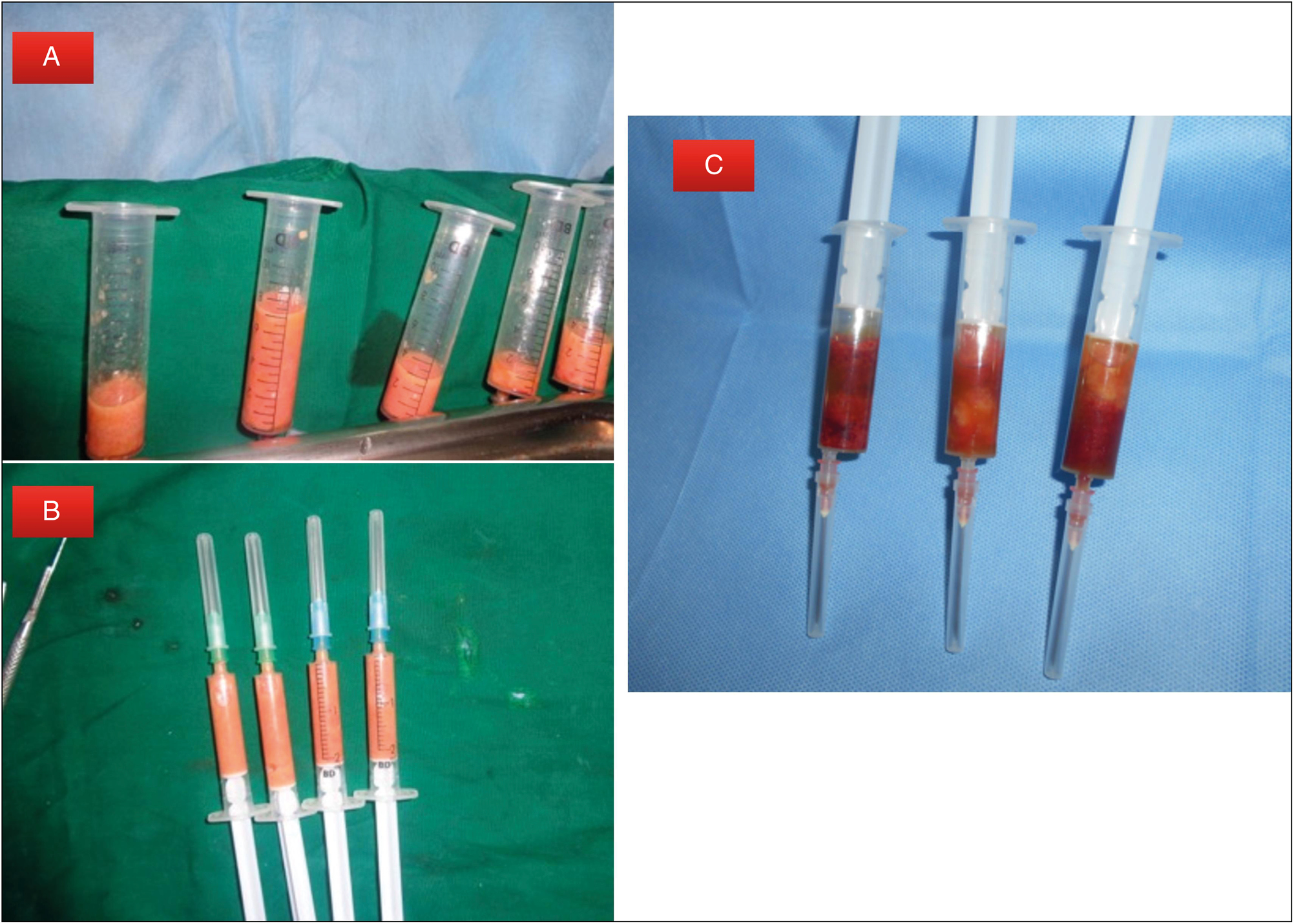
- A. Fat grafts after decantation and removal of the upper and lower layers. B. Processed graft transferred to the syringe. C. Appearance of unprocessed fat
For group B patients, the fat that was aspirated was allowed to stand for 20 min, undisturbed. After 20 min, it was noted that the aspirate differentiated into three gross layers:
top most oily layer;
middle layer containing the fat cells;
lower most layer containing blood, infiltrates.
The top most oily layer was removed with a cotton wick. The lowermost layer was drained out, and the middle layer was used for grafting. The graft was transferred to 2 cc syringes and was injected.
For injection, nerve blocks were given at the recipient site; 2 mm port was made at a nearby well-hidden area. Coleman injection cannulas were used for injections. The cannula fitted to a 2 cc syringe containing the graft was introduced through the port. The cannula was gently advanced through the subcutaneous tissue, reaching the distal end of the area to be grafted. Graft was injected in small packets, as the cannula was withdrawn. This was then repeated in different directions and in different planes. The aim of this maneuver was to have a uniform deposition of fat.
Postoperatively, a compressive dressing was applied on the donor area. Recipient area was left open with topical antibiotics applied at port sites. The patients were asked to avoid undue pressure on the recipient site in the form of pressure or massage. Oral antibiotics were prescribed for 1 week and analgesics for 3 days after surgery.
Patients were followed up weekly for 1 month and then two monthly up to 1 year. At the follow-up, photographs were taken and information was collected as per the proforma. Complications were looked for and noted. Patient satisfaction was noted at the end of 1 year, with one being poor, two for fair, three for good, and four for an excellent result.
The data were tabulated in Microsoft Excel. Data were compiled in the form of charts and diagrams. Statistical analysis of data was done. Patient satisfaction was assessed by the Mann–Whitney U-test. Comparison of proportions was by χ2 test. Statistical analysis was done using SPSS 17 software.
RESULTS
A total of 51 fat grafting procedures were performed in 30 patients. Twenty-six belonged to group A and 25 belonged to group B [Figures 3 and 4].

- Representative photograph. A 19-year-old female with hemifacial microsomia undergone autologous fat grafting (group A). A, B—preoperatively; C, D—1-year postoperatively

- Representative photograph. A 19-year-old female with hemifacial microsomia undergone autologous fat grafting (group B). A, B—preoperatively; C, D—1-year postoperatively
The age of patients ranged between 12 and 44 years. The mean age was 29.5 ± 8.3 years. Five (16.67%) patients were between 11 and 20 years of age, 15 (50%) patients were between 21 and 30 years of age, seven (23.33%) were between 31 and 40 years of age, and three (10%) patients were between 41 and 50 years age group. Seventeen patients were female and 13 patients in the study were male. Taking the total procedures into account, 30 procedures were done in females and 21 procedures were done in males. Among the 30 patients, 28 (93.33%) patients had grafting done to the face, 1 (3.33%) to the breast, and 1 (3.33%) to the hand.
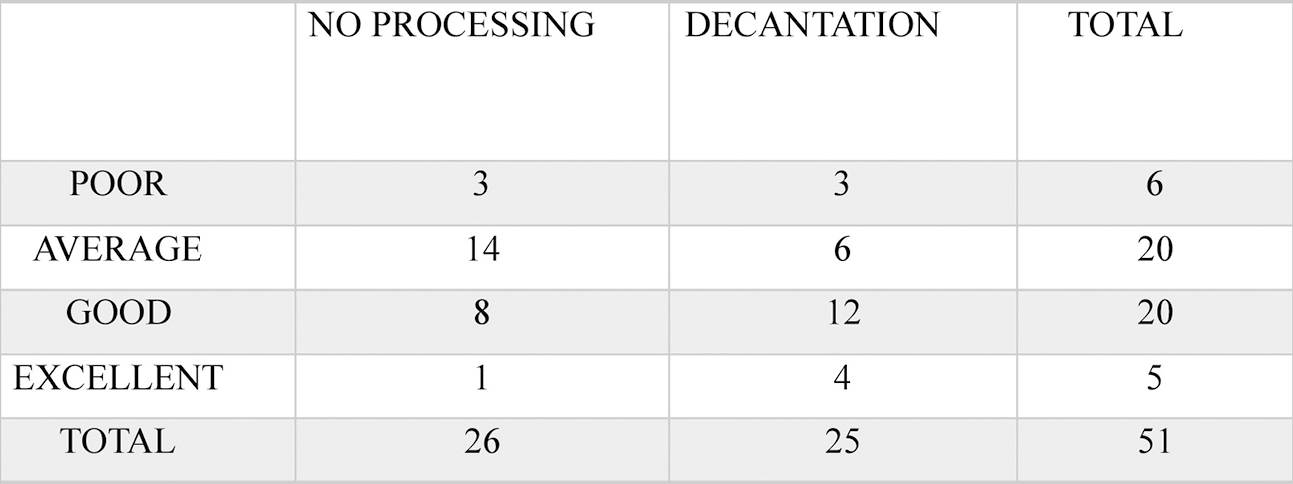
Most of the patients underwent the surgery for depressed scars on the face (60%). Others indications were hemifacial atrophy (16.67%), scar rejuvenation (10%), post ulnar nerve palsy hand wasting (3.33%), breast hypoplasia (3.33%), and lip augmentation (6.67%). The most common donor was left flank in 20 (39.2%) patients, right flank in 18 (35.3%) patients, and abdomen in 13 (25.5%) patients. Average of 10.2 ± 9.8 cc was injected, ranging from a minimum of 1 cc to a maximum of 40 cc in a sitting. Patient satisfaction was noted at the end of 1 year following the procedure [Tables 1 and 2]. Using the Mann–Whitney U-test, the p-value was 0.08012.
 |
 |
The complications seen in the study were pigmentation changes, bruising, and edema. Major complications such as fat embolism, blindness, etc. were not seen in our patients.
DISCUSSION
The “replace like with like” principle underlies much of the rationale behind the clinical use of autologous fat transplantation. Neuber first described the free autologous fat graft for soft tissue augmentation [Table 3]. In 1912, Hollander reported natural appearing changes after fat injections in patients with facial fat atrophy. The process of fat grafting was unpredictable, with surgeons unable to provide consistent results. By 1980s, fat transplant had fallen into disrepute, with prominent plastic surgeons denouncing the concept of fat transplant based on the early negative results. The American Society of Plastic and Reconstructive Surgeons Ad-Hoc Committee on New Procedures in 1985 stated: “The committee is unanimous in deploring the use of autologous fat injection.....”[4] Over the last three decades of the twentieth century, Dr Sydney Coleman[8] popularized fat grafting with his technique.
 |
Dr Sydney Coleman first described his technique of fat grafting in 1994 for facial rejuvenation.[9] The technique involves harvesting fat using specially designed cannulae, gentle handling, processing by centrifugation, and injecting as “packets” in multiple planes. Coleman’s technique laid down the principles of fat grafting, but more importantly showed that fat grafting can produce consistent and reproducible results. The techniques described for harvesting and injecting fat have stood the test of time.
Experimental and clinical studies have shown the effects of fat grafting using a myriad of processing techniques. Boschert et al.[10] compared different centrifugation speeds for processing of fat grafting. They noted decreased survival of the grafts with greater centrifugation speeds. Dangers of centrifugation were further delineated leading to a search for better techniques. Different processing techniques such as simple decantation, washing,[1112] and rolling[13] were investigated. In a review of literature, Gir et al.[14] concluded that there is no evidence to support one mode of processing over the other. Extracorporeal anoxia is a consideration during transfer and fat has to be grafted to the recipient site as soon as possible. Time efficiency improves the effectiveness of the technique.[15] The techniques which allow rapid processing would benefit from this advantage. Smith et al.[16] examined the effects of various types of processing on the viability of fat grafts. They used the XTT (2,3-bis-(2-methoxy-4-nitro-5-sulfophenyl)-2H-tetrazolium-5-carboxanilide) assay to determine viable adipocytes post grafting. Their data did not support the use of processing the graft, as unprepared samples showed higher cell viability than washed or centrifuged samples. They concluded that “the less one manipulates the fat graft and the more quickly it is reinjected, the higher are the chances of survival.”
The paradigm shift in the understanding of fat grafting has led to more extensive research on the stromal cell vascular fraction, where the stem cells lie. They have been considered to play the key role and may explain for the inconsistent outcomes.[17] Following this principle, a lower stromal vascular fraction isolation yield would result in lower graft volume and vice versa. Lee et al. described fat grafting as a regenerative, cell-directed therapy rather than simply as a means of filling soft tissue.[18]
In this prospective study, a total of 30 patients underwent 51 grafting procedures. In the follow-up, data were collected regarding patient satisfaction and complications, which was compiled and the study was done. The mean age of patients was 29.5 ± 8.3 years. Xie et al.[18] in their study had a mean age of 35.16 years and Martinez et al.[19] reported a mean age of 38.12 years.[20] Patients with Romberg’s disease present at a younger age for treatment and may be the reason for having a younger age group in our sample population. Fat grafting was more common in females which was also seen in the literature. Xie et al. had 19 males and 64 females in their group, Martinez et al. had two males and seven females, and Pinsolle et al. had only one male among eight subjects in their study.
The most common donor was left flank in 20 (39.2%) patients. In literatures, the abdomen is the usual choice. It has ample amount of fat, the harvest is easy, with the patient in supine position, where it is easy to prepare and infiltrate the wetting solution.
Cheng et al.[21] performed a questionnaire-based survey of members of the American Society of Plastic Surgeons. The surgeons reported their outcomes in terms of subjective assessment of survival, grouped as 0–25%, 25–50%, 50–75%, and 75–100%. According to their survey, 7.9% surgeons believed fat survival was 75–100%. Majority (56.4%) believed that the survival was between 50% and 75%. In our study, we had 50% of patients reporting good satisfaction and 6.7% reported excellent satisfaction which was similar to that seen in the survey.
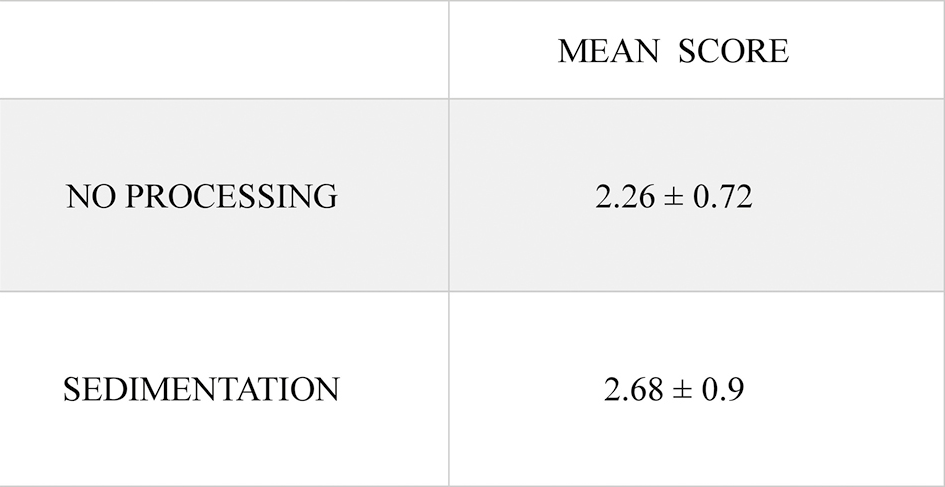
The patient satisfaction was noted at the end of 1 year. The mean score in the no-processing group was 2.2 ± 0.68 and the mean score in the processing group was 2.53 ± 0.99. Data analysis was done using the Mann–Whitney U-test. The U-value was 86.5. The critical value of U at P ≤ 0.05 was 64. This suggests that there is not a statistically significant difference in patient satisfaction following fat grafting, with or without processing. So although processing gives a higher proportion of favorable outcomes, it is not statistically different. For the patients included in this study, routine processing of harvested fat is not warranted. This makes the procedure much more simpler and faster, reducing the need of expensive machinery and theater time. For larger volumes of fat, however, processing may play a more important role.
There has been a paradigm shift in the understanding of fat survival, with stem cells being at the center of further studies. Survival of aspirated fat cell grafts depends mainly on the anatomic site, the mobility and vascularity of the recipient tissue, or underlying causes and diseases and less on harvesting and reinjection methods, provided that basic principles of gentle handling are kept in mind.
CONCLUSION
Fat grafting is a commonly done procedure, for a wide variety of indications. There is controversy regarding the ideal method of fat grafting. In this study, a statistically significant difference was not found between patients who underwent fat grafting with processing by sedimentation or without processing. Autologous fat grafting was found to be a safe procedure with no significant complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- [The first “fillers”, vaseline and paraffin. From miracle to disaster] Ann Chir Plast Esthet. 2007;52:157-61.
- [Google Scholar]
- ASPRS Ad-Hoc Committee on new procedures, September 30, 1987. Plast Surg Nurs. 1987;7:140-1.
- [Google Scholar]
- 2001–2015. National Plastic Surgery Statistics: Cosmetic and reconstructive procedure trends. Available at: http://www.plasticsurgery.org/news/plastic-surgery-statistics.html
- Roll, spin, wash, or filter? Processing of lipoaspirate for autologous fat grafting: An updated, evidence-based review of the literature. Plast Reconstr Surg. 2015;136:706-13.
- [Google Scholar]
- Photographic standards for facial plastic surgery. Arch Facial Plast Surg. 2005;7:331-3.
- [Google Scholar]
- Long-term survival of fat transplants: Controlled demonstrations. Aesthetic Plast Surg. 1995;19:421-5.
- [Google Scholar]
- The technique of periorbital lipo-infiltration. Oper Tech Plast Reconstr Surg. 1994;1:20-6.
- [Google Scholar]
- Analysis of lipocyte viability after liposuction. Plast Reconstr Surg. 2002;109:761-5; discussion 766-767.
- [Google Scholar]
- Lipo layering of autologous fat: An improved technique with promising results. Plast Reconstr Surg. 1998;101:820-6.
- [Google Scholar]
- Comparative analysis of processing methods in fat grafting plast. Reconstr Surg. 2014;134:675.
- [Google Scholar]
- Fat grafting: Evidence-based review on autologous fat harvesting, processing, reinjection, and storag. Plast Reconstr Surg. 2012;130:249.
- [Google Scholar]
- Classification of clinical fat grafting: Different problems, different solutions plast. Reconstr Surg. 2012;130:511.
- [Google Scholar]
- Autologous human fat grafting: Effect of harvesting and preparation techniques on adipocyte graft survival. Plast Reconstr Surg. 2006;117:1836-44.
- [Google Scholar]
- The key to long-term success in liposuction: A guide for plastic surgeons and patients. Plast Reconstr Surg. 2004;114:1945-52; discussion 1953.
- [Google Scholar]
- An integrated fat grafting technique for cosmetic facial contouring. J Plast Reconstr Aesthet Surg. 2010;63:270-6.
- [Google Scholar]
- Autologous fat transfer to the Cranio-maxillofacial region: Updates and controversies. J CrainoMaxillofac Surg. 2011;39:359-63.
- [Google Scholar]
- Breast augmentation with autologous fat injection: A report of 105 cases. Ann Plast Surg. 2014;73:S37-42. 10.1097/SAP.0000000000000271
- [Google Scholar]
- Current concepts of fat graft survival: Histology of aspirated adipose tissue and review of the literature. Dermatol Surg. 2000;26:1159-66.
- [Google Scholar]




