
Translate this page into:
Giant eccrine acrospiroma of the scalp
Address for correspondence: Prof. Gabriel Rodrigues, Department of General Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Manipal 576104, Karnataka, India. E-mail: gabyrodricks@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Eccrine acrospiroma is a benign skin tumor that arises from the ducts of sweat glands, presents as small solid or cystic lesions that rarely can undergo malignant transformation, and leads to a diagnostic dilemma. We report a 32-year-old woman who presented with a large pedunculated tumor of the scalp that was excised and histopathologically proven to be a giant eccrine acrospiroma. This case is being presented because of its infrequent occurrence and the unusual large size of the lesion on the scalp that has been not reported in the literature so far.
Keywords
Acrospiroma
benign
eccrine
excision
hidradenoma
scalp

INTRODUCTION
Eccrine acrospiroma, also known as hidradenoma, is a neoplastic tumor of sweat glands arising from the distal excretory duct.[1] Other synonyms of eccrine acrospiroma are clear cell, nodular, superficial or solid-cystic hidradenoma; clear cell papillary carcinoma; clear cell myoepithelioma; porosyringoma; large cell sweat gland adenoma; or basal cell carcinoma of sweat gland origin.[2] It commonly presents as a small, solitary, solid, or cystic lesion measuring about 1–2 cm in size, with common sites being trunk, scalp, axilla, and extremities and can occur after a minor cutaneous trauma.[23] It is usually benign in nature with only a few reported cases of malignant transformation.[4] They can lead to a clinical diagnostic difficulty and can be proven to be acrospiromas only histopathologically.[5] Surgical excision is the treatment of choice for benign acrospiromas.[6] This patient presented here had a chronic scalp swelling that was insidious on onset with no complications and was adequately surgically excised. A detailed literature review did not reveal such a large eccrine acrospiroma of the scalp and hence the purpose of presentation.
Case History
A 32-year-old woman, with no comorbidities presented to the Department of General Surgery with an asymptomatic swelling on the left side of scalp of 4 years duration that was insidious in onset. On examination, a 9 cm × 6 cm soft, cystic, nontender, bilobed, pedunculated, smooth swelling was present on the left side of scalp [Figure 1A]. Skin over and around the swelling was normal. Fluctuation was positive and the swelling was brilliantly transilluminant [Figure 1B]. Regional lymph nodal and systemic examination was unremarkable. A probable differential clinical diagnosis of epidermoid inclusion cyst, dermoid cyst, or clear cell carcinoma was made. Hematological investigations were unremarkable. Skull X-ray was normal and hence a CT head was done that showed a well-defined pedunculated extra-calvarial soft tissue density overlying the left parietal bone adjacent to coronal suture with interspersed heterogeneously hyperdense areas within [Figure 2]. Patient underwent a surgical excision of the lesion with a 1 cm margin all around with primary closure of the defect. Histopathology revealed a well-circumscribed encapsulated tumor in the dermis with overlying normal epidermis composed of polygonal cells with round to oval nuclei with grooving nucleoli and a moderate amount of clear to eosinophilic cytoplasm with no atypia or necrosis (as shown by arrow). Focal squamous eddies and cystic degeneration was observed, features suggestive of a benign eccrine acrospiroma [Figure 3]. The patient had an uneventful postoperative recovery. At follow-up after 8 months, she is asymptomatic with no local recurrence and is doing well.
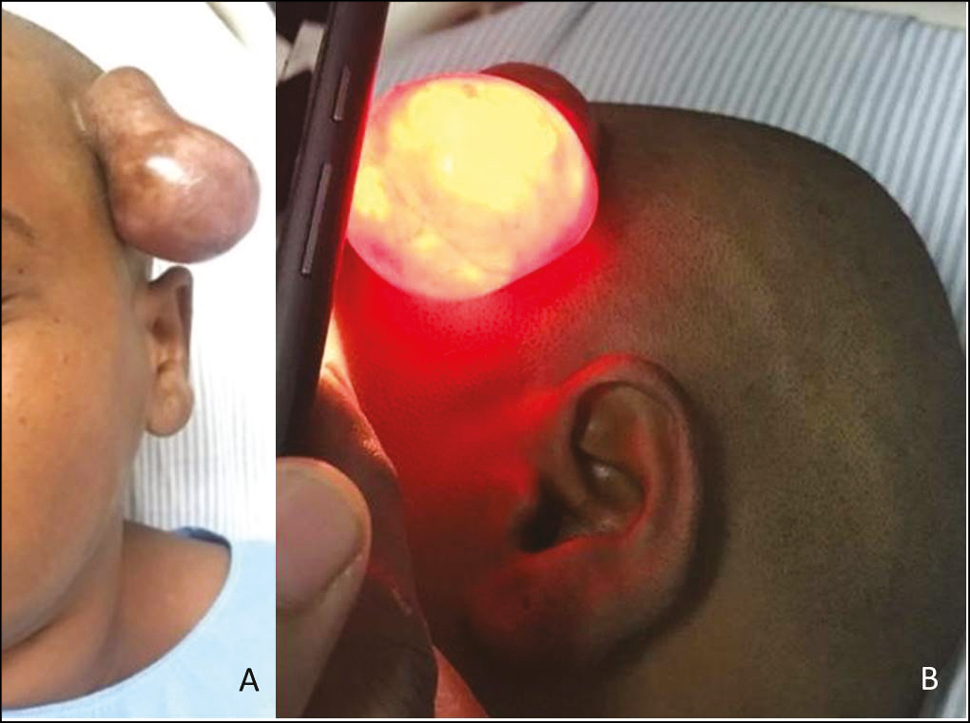
- (A) Left-side scalp swelling. (B) Brilliantly transilluminant
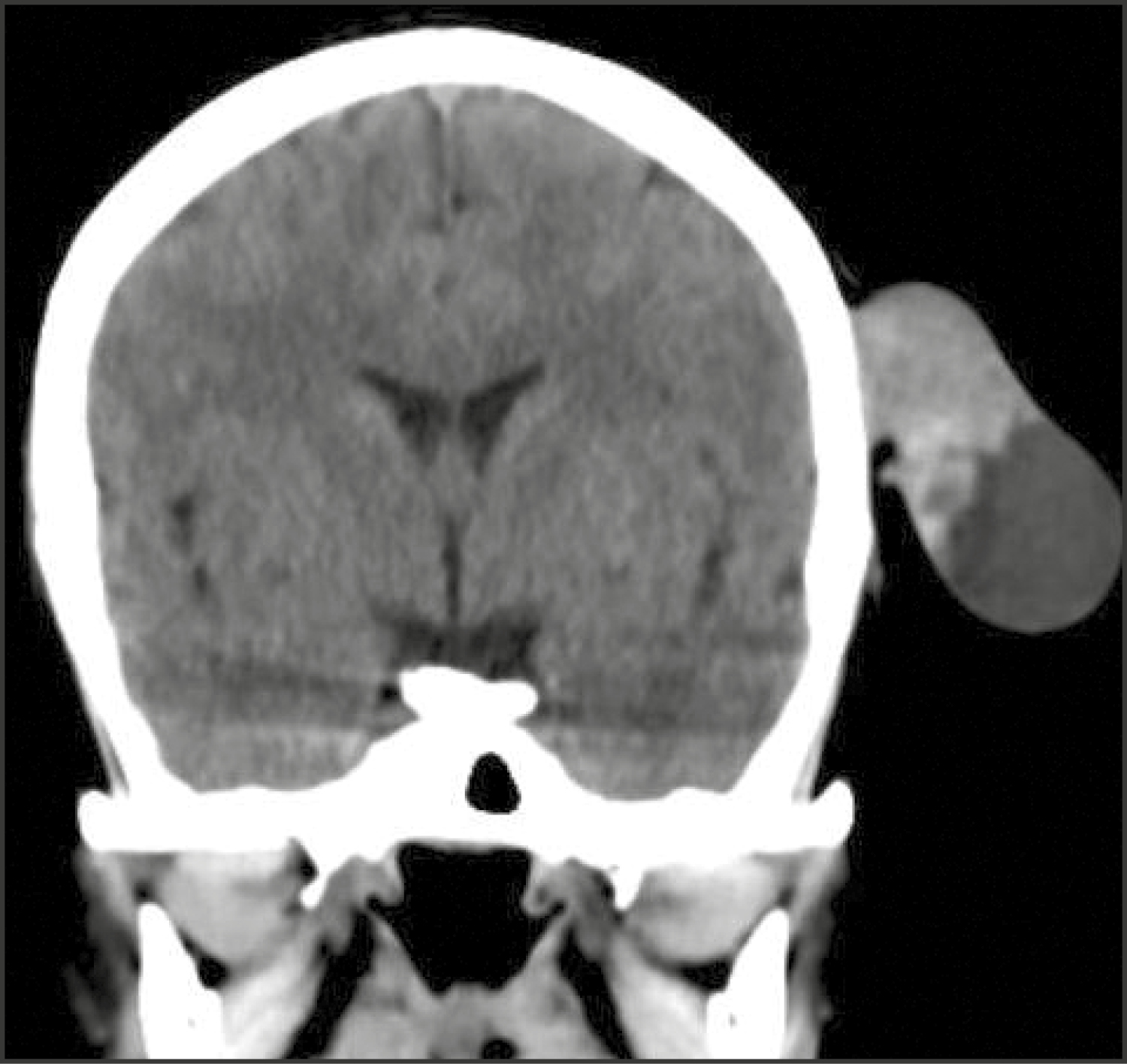
- CT head showing tumor arising from skin overlying the scalp
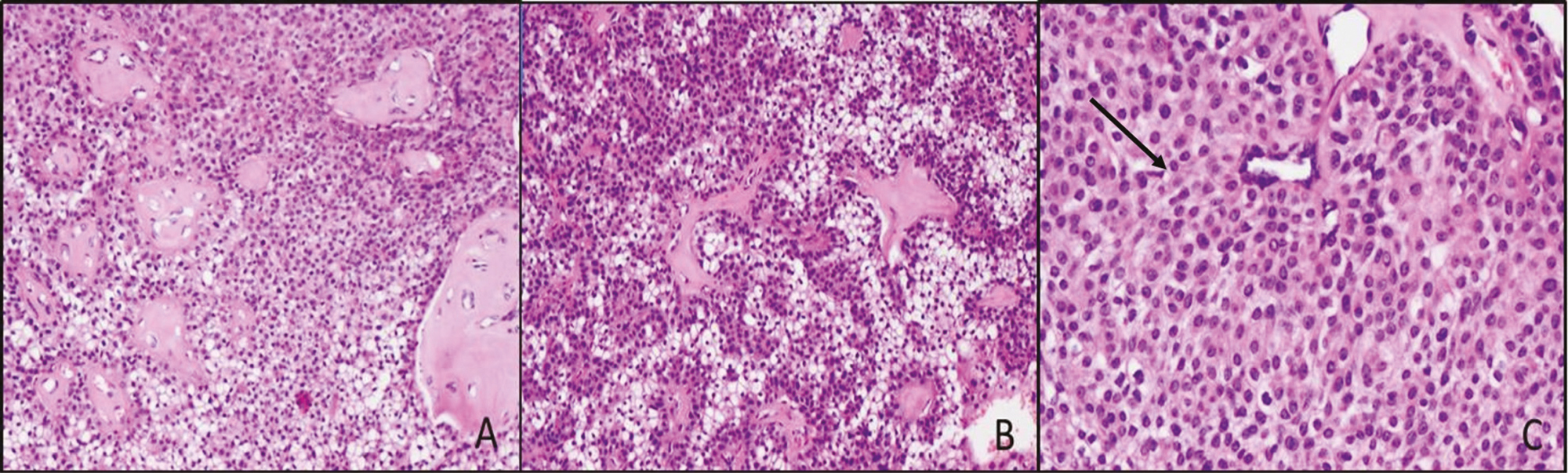
- (A) Stromal hyalinization (HandE, 100x). (B) Cells with clear cytoplasm (HandE, 100x). (C) Polygonal cells with round to oval nuclei and eosinophilic cytoplasm and ducts (arrow) (HandE, 200x)
DISCUSSION
First described by Johnson and Helwig in 1969, eccrine acrospiroma is a nonmelanocytic adnexal lesion arising from epithelial cells of the excretory duct of sweat glands and are largely being but rarely may show the malignant transformation.[12] They are solitary, solid or cystic lesions presenting as nodules, plaques, or papules.[23]
Eccrine acrospiromas occur in all age groups, but are more common in middle-aged and elderly individuals. There is a slight female bias with F:M ratio being 2:1.[4] It varies in size from being as tiny as 0.5 cm to as giant as 10 cm, but most measure less than 2 cm. Few cases of giant eccrine acrospiroma have been reported with the largest one was being 9.5 cm in size.[5] Large eccrine acrospiromas may raise the suspicion of malignancy, but size in never criteria for differentiating benign from malignant acrospiromas. Malignant ones are usually of moderate size with dimensions ranging between 4–10 cm, but rare.[56] They can occur anywhere on the body, but the highest incidence is on the trunk (40%), followed by head (30%) and extremities (30%); are usually painless and dry, but around 20% of them can be tender and around 20% may show some discharge.[2] Occasionally, these lesions may be associated with pruritus (7%).[3]
The etiopathogenesis of these lesions is unclear however some reports have shown an association between minor trauma and appearance of the lesion.[3] Histologically, they are classified as epidermal and dermal acrospiroma based on their location. Differential diagnosis includes squamous cell carcinoma, melanoma, metastatic tumors, and other adnexal tumors. However, careful histological examination helps us to arrive at the diagnosis.[5]
The only definitive treatment for acrospiromas is surgical excision and inadequate excision may lead to recurrence. Malignant ones require wide local excision with regional lymph node dissection, even in clinically node-negative cases. Eccrine acrospiroma has got a good prognosis with negligible recurrence after adequate excision.[7]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Giant eccrine acrospiroma: A case report and review of the literature. Can J Plast Surg. 2003;11:43-6.
- [Google Scholar]
- Malignant acrospiroma: A case report in the era of next generation sequencing. BMC Cancer. 2017;17:221.
- [Google Scholar]
- Stump the experts. Eccrine acrospiroma, clear cell type. Dermatol Surg. 1996;22:998, 1069.
- [Google Scholar]




