
Translate this page into:
Repair of Gauged Earlobes: Case Series and Review of Two Techniques According to Size
Address for correspondence: Dr. Michael M. Kim, Facial Plastic Surgery, 2525 NW Lovejoy St. Suite 402, Portland, OR 97210, USA. E-mail: Michael.Kim.MD@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Earlobe stretching is a common body modification typically performed in individuals under 30 years old. Individuals may later desire restoration of a natural earlobe contour. There is a paucity of literature regarding technique and outcomes for repair of the gauged earlobe defect.
Aims and Objectives:
The primary aim of this study was to provide a strategy to assess stretched earlobe defects and choose between the repair techniques of de-epithelialization and closure or excision and rotation. The secondary aim of this study was to evaluate complication rates of the two techniques.
Materials and Methods:
Retrospective review of all patients who underwent repair of stretched (gauged) earlobes at a single institution from 2012 to 2019. Patient demographics, maximum earlobe size, motivation for seeking repair, surgical technique, and complication rate were recorded.
Results:
Fifty-three patients underwent stretched earlobe repair. The average age was 25.9 years old; 60.0% of the patients were male. Defects repaired with de-epithelialization and closure had been stretched to an average of 12.4 (SD = 3.2) mm compared to 29.3 (SD = 10.9) mm for excision and rotation. The minor complication rate was 12.5% with de-epithelialization and 10.8% for excision and rotation. Motivations for seeking repair included a desire to look more professional for work (34.0%), personal preference (30.0%), and joining the military (23.0%).
Conclusion:
Smaller earlobe defects (<15 mm) with nonptotic lobules can be repaired with de-epithelialization and primary closure, whereas larger earlobes (>15.0 mm) with ptotic lobules require excision and rotation. Stretched earlobe repair is a well-tolerated procedure, although a significant number of patients will require minor revisions.
Keywords
Earlobe repair
gauged earlobes
ptotic earlobes
stretched earlobes

INTRODUCTION
Earlobe stretching is a popular body modification that uses progressively larger (gauged) jewelry to slowly enlarge an earlobe piercing. Over time, many patients with stretched earlobes desire to return their earlobes to the original, prestretched shape. A myriad of potential reasons for seeking repair exist including professional dress requirements, incompatibility with military service dress codes, or simply an evolution in personal aesthetic preference. Individuals with stretched ear lobes may also experience social stigma such as perceptions that they are less approachable and successful.[1]
Prior reports on the repair of stretched earlobes have consisted of small case series and have not provided a simple strategy to assess and classify earlobe gauge defects and decide on the optimal repair strategy. In addition, there is a gap in the literature about patient motivations for seeking earlobe repair and complication rates.[234567]
In this article, we provide our institution’s experience with earlobe repair over a 7-year period. We provide a simple classification system based on defect size. Earlobe defects that are small (<15 mm) and nonptotic can be repaired in a simple fashion by de-epithelizing the piercing tract and suturing the defect closed. We describe our surgical technique which includes the novel use of a chalazion clamp to facilitate excision. Larger ptotic lobules require a technique that addresses tissue redundancy. Our approach is a slight modification of previously reported techniques that removes the medial lobule and rotates the lateral earlobe to restore a natural earlobe contour.
MATERIALS AND METHODS
The study was approved by an institutional review board. Using billing (CPT) codes, all patients who underwent earlobe reconstruction between August 2012 and August 2019 at a large academic medical center were considered for inclusion. The medical records of these patients were reviewed. Patients were excluded if they underwent earlobe reconstruction for reasons other than for gauged earlobes (cancer, trauma, and torn earlobes). Patients were also excluded if earlobe defect size or operative details were incompletely documented in the medical record.
From the medical record, clinical and demographic information was recorded, including age, gender, and size of the stretched lobes. Follow-up rates were recorded. Complications were noted including infection, earlobe notching, unfavorable scar appearance, or asymmetry of earlobe contour. Preoperative and postoperative pictures were reviewed.
Statistics were performed with Microsoft Excel 2010. Comparisons were made between patients who underwent de-epithelialization and those who underwent excision and rotation. A descriptive statistics analysis was performed to determine means, standard deviations, kurtosis, and skew. From this, the data were determined to be normally distributed. An F-test for variance was performed with α set at 0.05. As the data were determined to have unequal variance, a two-sample t test assuming unequal variances was performed with α set at 0.05. To compare complication rates between the two groups, a fisher’s exact test was performed.
Preoperative evaluation and counseling
In our experience, gauged earlobes do not close without surgical intervention unless the maximum size of the jewelry worn was smaller than 10 mm (00 gauge). This is attributable to biological creep, a process by which a constant stretch load on the skin beyond its intrinsic viscoelastic property results in mitotic activity and generation of new skin cells.[8] Therefore, we generally recommend surgical restoration of an earlobe that was stretched beyond 10 mm. Patients are advised to remove all ear jewelry for at least one month before we proceed with repair to allow for tissue contraction and minimize the defect that must be repaired. Patients are instructed to wait at least 6 weeks after the repair before piercing the earlobe again, should they desire to wear conventional jewelry in the future.
The natural configuration of the earlobe attachment to the face should be assessed to determine if it is attached (inserts on the face at a right or obtuse angle) or unattached (inserts on the face at an acute angle). The ideal earlobe measures less than 15 mm from the tragal notch to the inferior attachment of the earlobe to the face (otobasion inferius), and less than 10 mm from the otobasian inferius to the lowest part of the lobule (subaurale).[910] The earlobe should be examined to determine if it is ptotic beyond the natural contour of the earlobe’s insertion into the facial sulcus [Figure 1, left]. If the earlobe is ptotic, skin resection and rotation will be necessary. If the earlobe retains a natural-appearing insertion, the tract can be de-epithelialized and closed in layers [Figure 1, right]

- Left: Photo of a 22-year-old male with an unattached caudal segment that stretches below the natural contour of insertion. Right: Photo of a 19-year-old male with an unattached caudal segment that retains normal lobe contour
Repair of small (nonptotic) stretched earlobes
If the stretched earlobe has not become ptotic, the tract can be excised and the earlobe closed primarily. The procedure begins by cleaning the ear and injecting local anesthetic (1% lidocaine with epinephrine 1:100,000). A chalazion clamp is placed around the piercing hole. This stabilizes the earlobe and improves hemostasis via compression of the surrounding tissue. In addition, one side of the chalazion clamp is a solid metal disc, which serves as a backstop onto which a cutting instrument can be evenly pressured. A 4 mm or 6 mm skin biopsy punch is used to core and excise the epithelized tract. The skin is undermined from the underlying fibro-fatty tissue to allow for tissue eversion. The deep fibro-fatty tissue is re-approximated first with absorbable suture. Sutures are then placed to close the skin on the front and backside of the earlobe. Standing cone deformities are excised as needed [Figures 2 and 3].
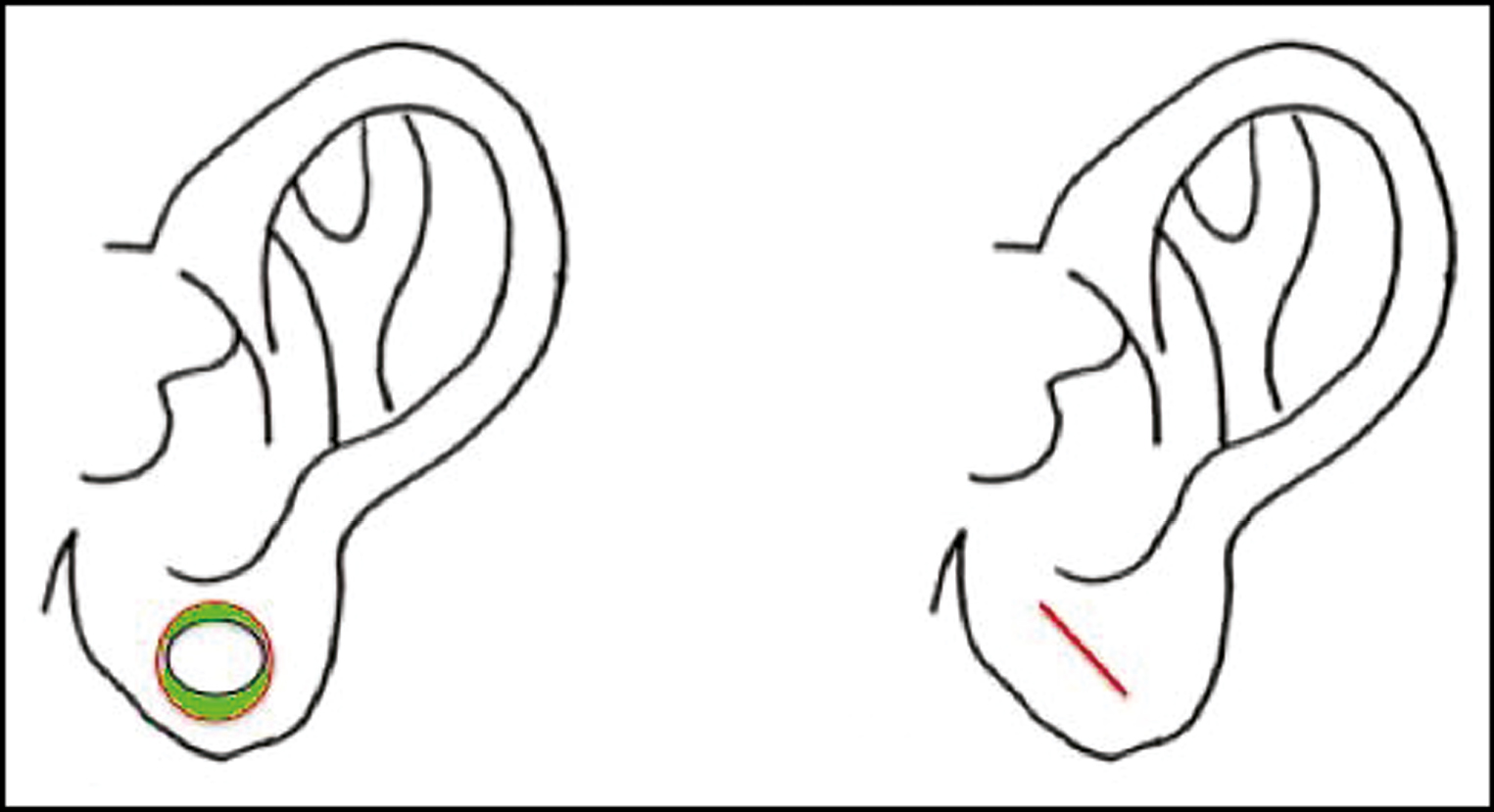
- Drawing of ear. Green outlines the tissue excised and the solid red line shows incision placement on the left and scar orientation on the right

- Top: Photos of a 33-year-old male before (left) and 14 days after (right) repair. Bottom: Photos of a 19-year-old male before (left) and 14 days after repair (right)
Repair of large ptotic stretched earlobes
If the earlobe has become ptotic, skin excision and rotation is necessary to restore the natural shape of the earlobe. The skin is cleansed and local anesthetic is injected (1% lidocaine with epinephrine 1:100,000). The inferior portion of the caudal earlobe defect is divided. The incision is generally placed around the midpoint of the ptotic segment, but should be adjusted as needed to create the appropriate length flap to reach the face and create the desired earlobe shape. Excess skin is removed from the medial portion of the lobe and the superior edge of the flap is de-epithelialized. A small portion of skin at the superolateral corner of the flap is removed to prevent a standing cone deformity as the flap is rotated medially. Absorbable sutures are placed to secure the fibrofatty deep layer of the rotated segment. Anterior and posterior cutaneous stitches are then placed [Figures 4 and 5].
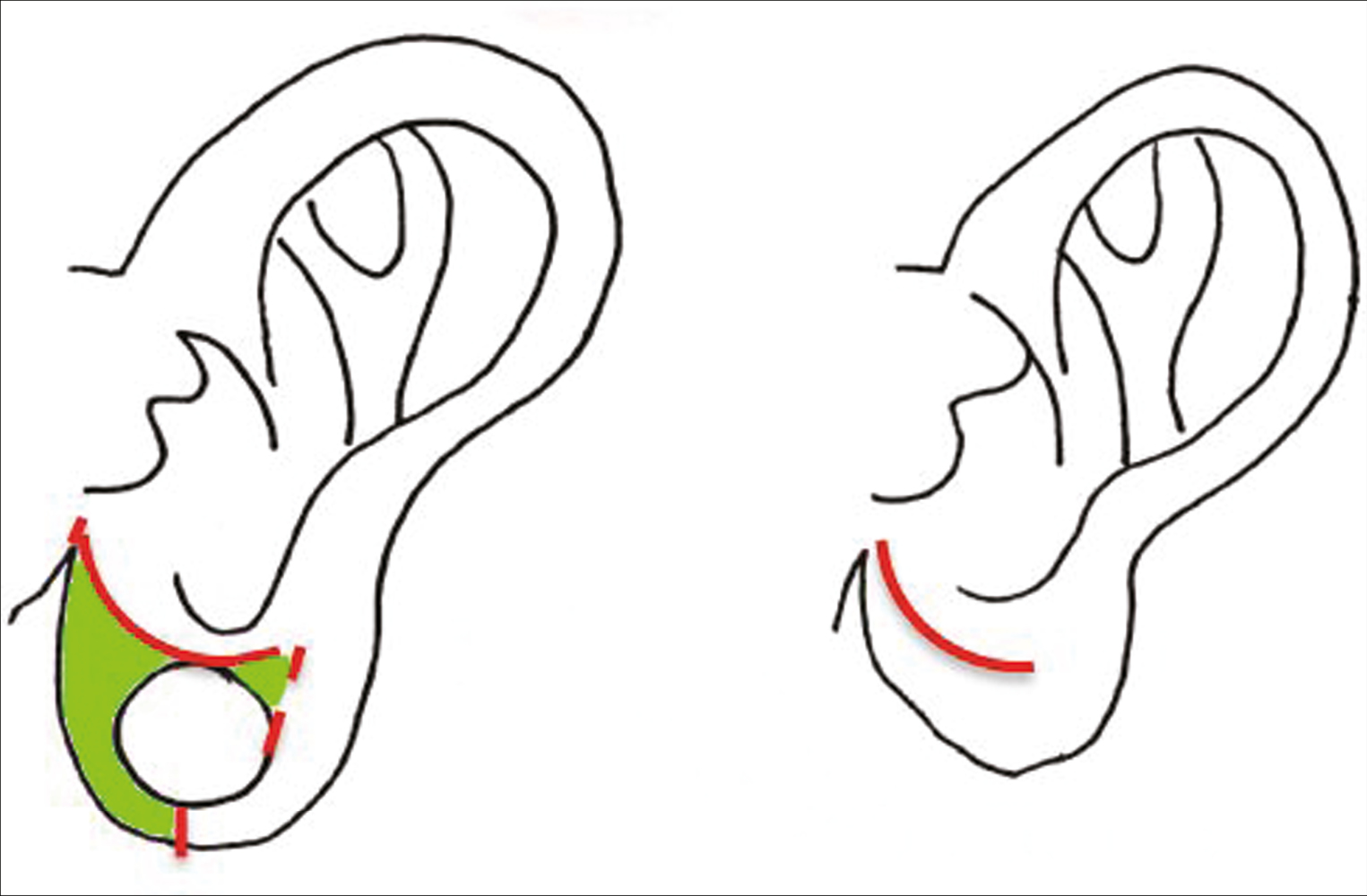
- Drawing of ear. Green outlines the tissue excised and solid red lines show incision placement on the left and scar orientation on the right. The dotted red line shows the cut to prevent a standing cone deformity

- Top: Photo of a 25-year-old female before (left) and 19 days after (right) repair. Bottom: Photo of a 27-year-old-male before (left) and 48 days after (right) repair
RESULTS
Sixty-three patients underwent stretched earlobe reconstruction during the study period. Ten patients were excluded due to undergoing repair of a torn stretched earlobe or incomplete documentation of earlobe defect size or operative details. The final sample size was 53 patients. The average patient was 25.9 (SD = 4.9) years old, 60.0% of the patients were male. The average length of time with gauges in place was 8.2 (SD = 4.9) years. The most common reasons for seeking repair were to look more professional for work (34.0%), followed by personal preference (30.0%), and joining the military (23.0%). Of the total cohort, 15 patients (28.0%) were current or former smokers.
Sixteen patients underwent repair using the de-epithelialization and closure (punch) technique, with an average maximal earlobe piercing (gauge) size of 12.4 mm (SD = 3.2 mm). Thirty-seven patients underwent repair using the excision and rotation technique, with an average maximal earlobe piercing (gauge) size of 29.3 mm (SD = 10.9 mm). There was a statistically significant (P < 0.001) difference between these means.
Two (12.5%) of the patients who underwent de-epithelialization required scar revision, compared to four (10.8%) of the patients who underwent excision and rotation. These differences were not statistically different. One patient required a revision after the repaired earlobe snagged on an article of clothing leading to a dehiscence. Size of the earlobe defect and patient history of smoking were not significantly associated with complication rate. The mean follow-up length was 51 (SD = 86) days, although 25.0% of patients did not return for any follow-up appointments.
DISCUSSION
The ideal repair of a stretched earlobe results in a natural rounded earlobe with minimal scarring and is amenable to conventional piercing in the future. The literature on this topic is sparse and consists of case reports of one to two patients with a focus on describing the author’s preferred surgical technique. We present a robust description of our institution’s experience and outcomes with earlobe repair in 53 patients over a 7-year time span.
Our technique for repairing nonptotic gauged earlobes uses a punch biopsy to remove the epithelialized piercing tract. Use of a punch biopsy for repair of gauged earlobes was first described by Tan et al.[2] In his report, the punch biopsy technique was not recommended for defects larger than 4 mm. In our experience, excellent results can be obtained for larger defects (up to 6 mm) as long as the earlobe has not become ptotic. Our method also differs from the original report in that we use a chalazion clamp to improve tissue handling and provide a backstop for the punch. To the best of our knowledge, use of a chalazion clamp to assist with earlobe repair has not been reported previously.
To repair a ptotic earlobe, a technique which addresses tissue redundancy and restores a natural earlobe contour must be used. We use an excision and rotation method that is similar to the technique described in case reports of a single patient by Hunter et al.[6] and in three patients by Henderson et al.[7] Our approach is a subtle modification in that we remove the superolateral portion of the earlobe defect to prevent a standing cone deformity. Removing this tissue does narrow the flap base width and therefore provides a theoretical risk of leading to vascular compromise of the distal portion of the flap. However, in our series, no incidents of vascular compromise were encountered. Our comparatively robust series of 37 patients provides greatly needed additional evidence that this technique has excellent cosmetic outcomes and a low complication rate.
In our series, 6/53 (11.0%) patients required minor revisions for subtle asymmetry between ears or an unfavorable scar. Though these minor complications were easily corrected with in-office procedures, the potential need for a revision procedure should be discussed with the patient preoperatively. Given the small number of patients in prior case reports describing earlobe repair, there is insufficient data to make a meaningful comparison of how our complication rate compares to other authors.
Our study is limited by the relatively small sample size, which makes comparing the complication rate between the punch biopsy and the excision and rotation techniques challenging. We did not find a difference in complication rate between the two repair techniques or between smokers and nonsmokers. However, we acknowledge that a difference might not have been detected due to a lack of power. In our series, around 25.0% of patients did not return for follow-up appointments, so it is also possible that some of these patients might have had complications that were not identified. In addition, our study was limited by the retrospective nature of the data acquisition, which does not allow for the assessment of patient satisfaction, which would be an interesting outcome metric.
We conclude that for patients with nonptotic stretched earlobes, de-epithelialization, and closure using the punch biopsy technique is an excellent method of repair. In general, earlobes that were stretched up to maximum of about 15 mm will retain a normal earlobe contour and will contract sufficiently once the jewelry is removed to allow for an aesthetic repair using the punch biopsy technique. Earlobes that are stretched beyond 15 mm will have generally lost a normal earlobe contour and will require tissue excision and rotation. Both techniques are simple and well-tolerated procedures with excellent cosmetic outcomes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Stretched earlobe piercings negatively impact casual observer perceptions. Facial Plast Surg. 2019;35:299-305.
- [Google Scholar]
- Punch technique—an alternative approach to the repair of pierced earlobe deformities. J DermatolSurg Oncol. 1989;15:270-2.
- [Google Scholar]
- Earlobe reconstruction following plug and tunnel piercing. J Plast Reconstr Aesthet Surg. 2010;63:e294-5.
- [Google Scholar]
- Double opposing perpendicular linear repair of gauge ear-piercing deformity: A new technique and literature review. Eplasty. 2014;14:e31.
- [Google Scholar]
- Repair of Massive Earlobe Piercing and Plugs (Gauging) Plast Reconst Surg. 2014;2:e225.
- [Google Scholar]
- Surgical correction of the expanded earlobe after ear gauging. Aesthetic Plast Surg. 2010;34:632-3.
- [Google Scholar]
- Creep vs. Stretch: A review of the viscoelastic properties of skin. Ann Plast Surg. 1998;41:215-9.
- [Google Scholar]
- Earlobe morphology: A simple classification of normal earlobes. J Plast Reconstr Aesthet Surg. 2009;62:277-80.
- [Google Scholar]
- The aesthetic earlobe: Classification of lobule ptosis on the basis of a survey of North American caucasians. Plast Reconstr Surg. 2003;112:266-72; discussion 273-4.
- [Google Scholar]




