
Translate this page into:
Atrophic Dermatofibroma in a Young Female: A Rare Entity
Address for correspondence: Dr Neerja Puri, Department of Dermatology, G. G. S. Medical College, Faridkot, Punjab, India. E-mail: neerjaashu@rediffmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Introduction:
Atrophic dermatofibroma is a rare variant of dermatofibroma which is many times underdiagnosed.
Case Report:
We report a case report of a 29-year-old female who came to the dermatology department with black-colored lesions on the lower leg for the past 7 years. Histopathological examination revealed a non-encapsulated dermal tumor involving upper to deep reticular dermis and extending to superficial subcutis. There was epidermal hyperplasia, and at the center of the lesion a slight epidermal atrophy was present.
Discussion:
It is a commonly underdiagnosed variant of dermatofibroma. Histopathologically, this disorder presents as a decrease in at least 50% of the thickness of the dermis relative to the adjacent dermis. The case is rare and hence reported.
Keywords
Atrophic
dermal
dermatofibroma
dimpling
fibrous histiocytoma

INTRODUCTION
Dermatofibroma is a benign fibrohistiocytic tumor, but sometimes with a rare variant like atrophic dermatofibroma, the diagnosis becomes difficult. Dermatofibroma commonly presents with a skin colored or brown-colored nodule and it can be single or multiple and is seen most commonly on the lower legs and has a female predisposition.[1] An important diagnostic feature of dermatofibroma is the elicitation of dimple sign, which is elicited by two fingers resulting in dimple production, due to tethering of overlying epidermis to the underlying lesion. Atrophic dermatofibroma is a variant of dermatofibroma which is often misdiagnosed. This rare variant is most often misdiagnosed. A slight dermal atrophy is a component of all variants of dermatofibroma and more so pronounced in the atrophic variant, in which the dermal atrophy exceeds 50%.[2] Atrophic variant represents 2% of all dermatofibromas. Dermal atrophy is a phenomenon which is normally seen in dermatofibromas as shown by the dimpling on lateral pressure. But, this feature is exaggerated in the atrophic variant of dermatofibroma. This occurs due to loss of elastic fibers due to “elastophagocytosis” by the dermatofibroma cells.[3]
CASE REPORT
We report a case report of a 29-year-old female who came to the dermatology department with black-colored lesions on the lower leg for the past 7 years which progressively increased in size over the years. There was no history of trauma and her family history was negative. No associated disease including epidermolysis bullosa was seen in our case. There was no itching over the lesions. On examination, blackish to brownish indurated plaque was present over left lower leg of size 0.5–1 cm. In fact, it is a commonly underdiagnosed variant of dermatofibroma. Histopathologically, this disorder presents as a decrease in at least 50% of the thickness of the dermis relative to the adjacent dermis. There was no discharge or bleeding on touching the lesion. Dimple sign was elicited and was positive [Figure 1]. Dermoscopy of the lesions showed white scar-like patches along with peripheral pigmented network [Figure 2]. A differential diagnosis of Bowen’s disease and lichen sclerosus atrophicus, melanocytic tumor, and dermatofibroma was made. A biopsy was done and histopathological examination revealed a non-encapsulated dermal tumor involving upper to deep reticular dermis and extending to superficial subcutis. There was epidermal hyperplasia and at the center of the lesion a slight epidermal atrophy was present. The tumor was composed of intertwined and interwoven spindle cells in a collageneous stroma with collagen trapping of collagen bundles along the edges [Figure 3]. The cells had bland fusiform nuclei without cytological atypia or significant mitosis. Uninvolved papillary dermis containing mild perivascular lymphocytic infiltrate with few melanophages separated the tumor from epidermis showing irregular psoriasiform hyperplasia with elongated rete ridges with overlying mildly hyperkeratotic stratum corneum. Von Gieson’s stain was used for staining elastic fibers. Immunohistochemistry was positive for Factor XIIIa and negative for CD34. After the biopsy report was obtained, complete surgical excision of the lesion was done. Hence, we report a typical case of atrophic dermatofibroma, an uncommon and probably underdiagnosed variant of a frequent lesion.

- Atrophic dermatofibroma in a 29-year-old female eliciting dimple sign
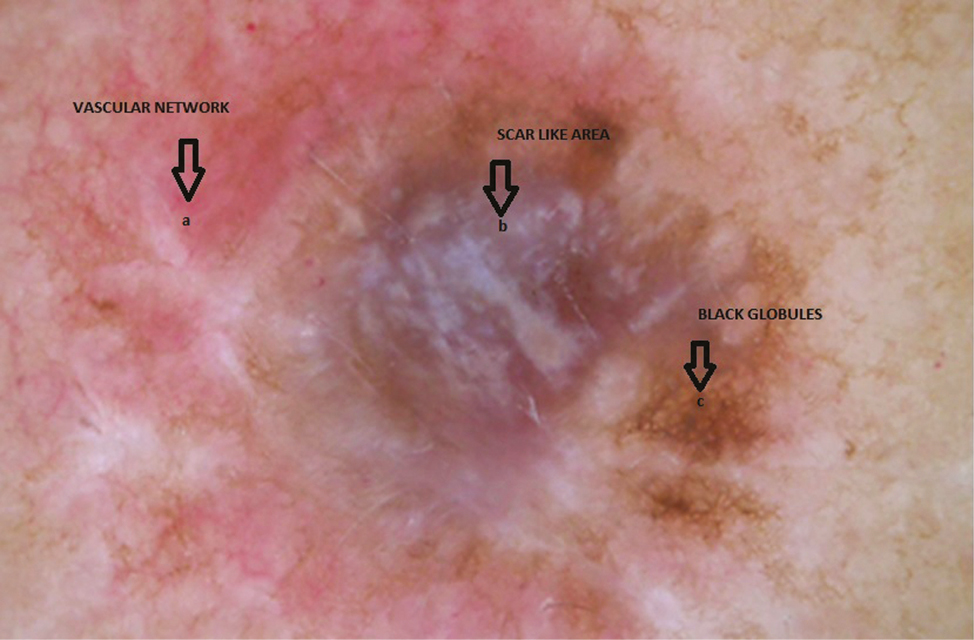
- Dermoscopy of the lesion showing white patches surrounded by a pigment network
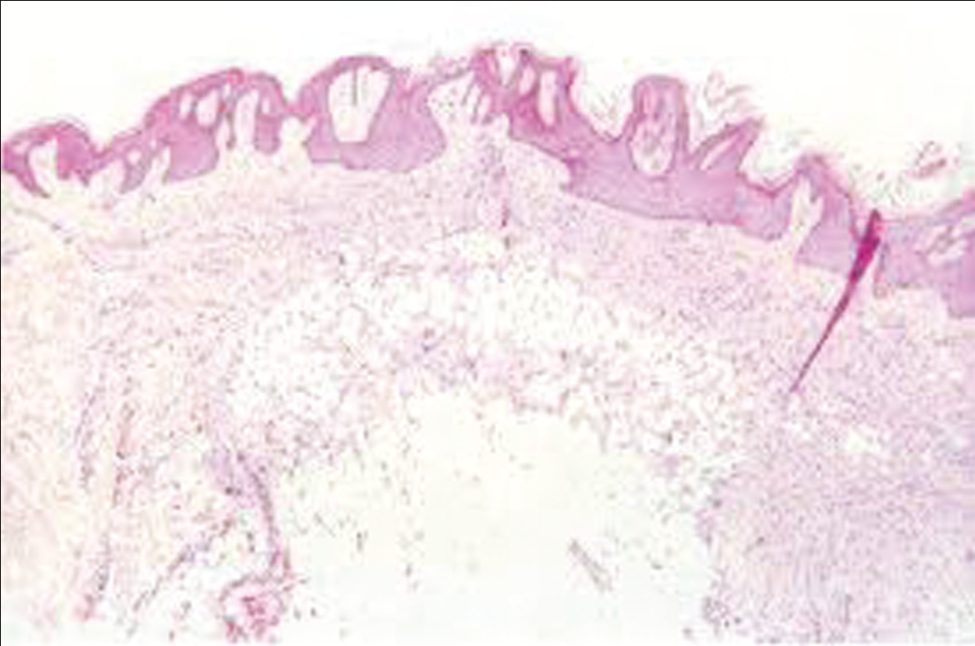
- Histopathology of the lesion showing intertwined and interwoven spindle cells in a collageneous stroma with collagen
DISCUSSION
Dermatofibroma is also known as benign fibrous histiocytoma and there is not much difficulty in diagnosis in most of the cases except for a few uncommon variants. These are characterized by firm, elongated, asymptomatic papules measuring few millimeters to 1–2 cm in diameter and are compressible on palpation.[4] Most of the patients have single lesions, but multiple lesions can be seen in few patients. Since our lesion was hyperpigmented, dermoscopy is an important evaluation tool, to differentiate it from melanocytic tumors. Dermoscopy of atrophic dermatofibroma shows white scar-like patches, a central plate, and a fine, regular, and pigmented network on the periphery, a patchy pigment network which classifies it as a non-melanocytic lesion.[5] It also shows arborizing vessels arising from a bluish homogeneous area resembling a flame pattern. There are various variants of dermatofibroma such as atrophic, atypical polypoidal, giant, subungual, erosive, lichenoid, ulcerated, dermatofibroma, and grouped palmoplantar histiocytoma.[6]
There are various atypical presentations of dermatofibroma.[7]The variant which we have reported is the atrophic variant of dermatofibroma, which is of uncertain origin. This variant is characterized by a flat, atrophic, or depressed surface. The pathology of an atrophic dermatofibroma has the same features that can be observed in a common fibrous dermatofibroma; there is acanthosis, basal layer hyperpigmentation, and induction of basal cell carcinoma-like features, hair follicle formation or sebaceous hyperplasia in the epidermis, and a proliferation of spindle-shaped fibroblasts in the dermis.[8] However, atrophic dermatofibromas also demonstrate depression of the central surface and thinning of the dermis; in many cases, the dermal atrophy is at least 50%. Elastic fibers are either decreased or absent. Histopathology of this variant shows a decrease in the thickness of dermis and elastic fibers by 50%. Specific staining for elastic fibers like van Gieson’s stain shows a reduction in these fibers. It is important to differentiate dermatofibromas from pigmented melanocytic lesions, atrophic scarring, and dermatofibrosarcoma protuberans.[910]
CONCLUSION
The atrophic variant of dermatofibroma is a rare and underdiagnosed variant, and one needs to be fully aware about its diagnosis. Since atrophic dermatofibroma is a frequently misdiagnosed variant, we stress upon the importance of considering this diagnosis if atrophic or sclerotic lesions are seen, especially in the middle-aged women. It is important to recognize this variant because it has high potential for local recurrence and metastasis and so, a complete surgical excision and regular follow-up are recommended in all cases after the final diagnosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Dermal and subcutaneous tumors. In: Andrews’ diseases of the skin, clinical dermatology (10th ed.). Philadelphia: Saunder; 2006. p. :611-2.
- [Google Scholar]
- Atrophic dermatofibroma: A case report and review of the literature. Dermatol Surg. 2002;28:1085-7.
- [Google Scholar]
- Typical and atypical dermoscopic presentations of dermatofibroma. J Eur Acad Dermatol Venereol. 2013;27:1375-80.
- [Google Scholar]
- Atrophic dermatofibroma accompanied by aneurysmatic characteristics. J Eur Acad Dermatol Venereol. 2006;20:331-3.
- [Google Scholar]
- Fibrous histiocytomas: Histopathologic review of 95 cases. An Bras Dermatol. 2010;85:211-5.
- [Google Scholar]
- Atrophic dermatofibroma and dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1987;17:947-50.
- [Google Scholar]
- Atrophic variants of dermatofibroma and dermatofibrosarcoma protuberans. Histopathology. 1995;26:519-27.
- [Google Scholar]




