
Translate this page into:
Midface Rejuvenation Using Juvederm Fillers in Male Patients
Address for correspondence: Dr. Kritika Rai, Berkowits Hair and Skin Clinic, J-1, Kailash Colony, New Delhi 110048, India. E-mail: kritika.rai16@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
In the recent years, there has been a significant rise in the number of men seeking rejuvenating procedures. The development of minimally invasive, non-surgical, office-based procedures without minimal downtime has stimulated a fresh interest among men who may seek cosmetic treatment to increase competitiveness and appear youthful in the workplace. It is important to understanding the differences in facial features in men and women to achieve more natural results and to reduce the risk of feminizing the male’s face.
Aim:
The purpose of this study was to present our experience of midface rejuvenation using hyaluronic acid (HA) fillers in men.
Materials and Methods:
The authors discuss the anatomical considerations, pathophysiology of aging, gender considerations, and their injection technique for midface rejuvenation in male patients.
Results:
Midface rejuvenation was successful in male patients using HA dermal fillers while maintaining the masculine features. The treatment was well tolerated and resulted in high level of satisfaction.
Conclusion:
Use of injectable HA dermal fillers is a safe, effective, and well-tolerated non-surgical treatment modality for midface rejuvenation in men. A thorough knowledge of the midface anatomy, injection techniques, and properties of individual fillers along with an understanding of the considerations in facial features of men can make injectable dermal fillers a rewarding treatment even in male patients.
Keywords
Dermal fillers
hyaluronic acid fillers
malar augmentation
male midface rejuvenation
midface rejuvenation

INTRODUCTION
The midface consists of important hallmarks of facial features.[1] A youthful male and female midface has some common characteristics, but they differ considerably in structure and proportion.[2] In the recent years, the understanding of the pathophysiology of midface aging has evolved, with greater emphasis on revolumizing the face rather than lifting alone.[3] Injectable fillers offer a versatile, safe, and effective means for rejuvenation of the midface by replacing the volume loss, contouring, and providing structural support.[13] They can give patients a youthful look with a relatively quick painless lunchtime procedure, with regular maintenance treatments.[4]
Though men have been more reluctant to undergo cosmetic procedures than women, the past few years has seen a significant rise in the number of rejuvenation procedures performed in men.[2] The development of minimally invasive, non-surgical, office-based procedures without any downtime has stimulated a fresh interest among men who are unwilling to undergo invasive surgical treatment due to their morbidity and downtime.[2]
In the recent times, both men and women seek cosmetic treatment for the same issues and concerns. Both want to look better at their workplace because of competition. Even men want to look less tired and appear youthful for more social acceptance. The knowledge of differences in facial features in men and women enables in achieving a more natural result and reduces the risk to feminize the male’s face. Women have more prominent upper facial characteristics, with a gradual upper to lower taper in facial silhouette, whereas men have squarer faces with larger jaws.[5]
Midface rejuvenation in men and women needs to be done taking into consideration the gender differences in facial anatomy as well as the concern and reason for which they seek treatment. In this study, we present our experience of midface rejuvenation using fillers in men based on anatomy, pathophysiology of aging, gender considerations, and injection technique.
ANATOMIC CONSIDERATIONS
Midface is the central third of the face extending from the glabella to the subnasale.[6] The zygomaticus major represents the lateral border and the nasolabial fold demarcates the medial border of the midface.[78]
The appearance of midface as well the subsequent changes that occur with aging are largely dependent on the shape and degree of projection of the underlying skeleton [Table 1]. Midface skeleton is mainly formed by the zygoma, anterior surface of the maxilla, and, to a minor degree, by the lacrimal bone.[7]
| Skeletal changes with age | Associated soft tissue changes | |
|---|---|---|
| Periorbital region | Orbital aperture increases. Recession occurs in inferolateral orbital rim by middle age, whereas in the superomedial aspect, it may be noted only in old age. Inferomedial quadrant has a tendency to recede in old age, especially in men | Development of eye bags Appearance of brow descent and lateral orbital hooding Lower lid lad, formation of crow’s feet, and prominence of lower lid fat pockets |
| Midface | Maxillary retrusion Decrease in maxillary angle Canine fossa becomes more concave |
Volume loss in the cheek area Loss of skeletal support for the malar fat pad leads to deep nasolabial folds |
| Perinasal changes | Resorption at the piriform aperture Decrease in the piriform angle |
Decreased nasal support and projection |
The soft tissues of the face are arranged in five basic layers, similar to the scalp: skin, subcutaneous layer, musculoaponeurotic layer, loose areolar tissue, and the deep fascia and periosteum. An understanding of the fourth layer plays a key role in understanding the midface. Within this layer are the facial ligaments (orbicularis retaining and zygomatic and upper masseteric ligaments) that fix the overlying soft tissue to the facial skeleton.[7]
Neurovasculature: Midface consists of important vessels and nerves. It is important to understand the course and depth at which these are situated to prevent any injury during filler injection. While treating the midface, the injector must be wary of the infraorbital vessels, zygomaticofacial artery, facial artery as well as the branches of the facial nerve.
AGING OF MIDFACE
The optimal use of dermal fillers requires a thorough understanding of the aging face.[11] The effects of midcheek aging are the result of the interplay of factors including skeletal remodeling, soft tissue maturation, gravity, muscular activity, and environmental changes.[710] These changes occur in all five anatomical layers of the soft tissue as well as in the bone[7] [Table 1]. The skeletal foundation sets the framework for the overlying muscles and soft tissues, which add volume and a youthful appearance to the face.[8]
As a person ages, the subcutaneous fat undergoes atrophy which leads to loss of skin elasticity and tone. As a result, the skin may appear loose and saggy. These changes cause a downward displacement of the malar soft tissue. This movement is resisted by the zygomatico-cutaneous ligament, which connects the skin to the deeper skeleton. The soft tissue descent thus forms a mound also known as the “malar mound” or “malar bag” above a midcheek crease. Similarly, the orbicularis retaining ligament, which connects the inferior orbital rim to the skin, resists the downward descent of the soft tissue to form a preseptal ptosis or bulging above an “orbitomalar crease.” A tear trough deformity may be present alone or along with the midcheek and/or orbitomalar crease.[12]
Furthermore, ptosis of tissues of the cheek accentuates the nasolabial folds with downward orientation of the commissures.[8] The skeletal volume loss occurs largely due to resorption of the maxilla.[78]
PATIENT EVALUATION
Prior to treatment, it is mandatory to conduct a proper aesthetic evaluation of the patient to obtain natural-looking results. The specific areas of interest in the midface include malar projection, nasolabial folds, and the tear trough area. A thorough knowledge of important neurovascular and anatomical structures near the injection sites is mandatory. Patients were examined in an upright position, and photographs were taken at baseline and after treatment in the anteroposterior and right and left oblique and lateral views.
The aim of midface rejuvenation in men is to provide structural support to the cheeks, to correct and lift the nasolabial folds, and to address the volume deficit in the tear trough region. While treating the midface, it is also important to take into consideration the upper and lower face in order to maintain balance and harmony among the facial features. However, gender differences must be taken into account. Understanding the differences in facial features of men and women helps in achieving a more natural result and reduces the chances of feminizing a male face.[5] The aesthetic endpoint in men differs from that in women, in that the male cheek is less prominent. Men also have a bizygomatic to bigonial distance of approximately 1:1 [Figure 1], whereas a youthful woman’s face is characterized by the inverted “triangle of youth,” with a wider bizygomatic distance to that of the bigonial distance.[13] Another distinction is the shape of the ogee curve, which is an S-shaped curve from the cheekbone to the mid-cheek hollow. In men, the curve is flatter in its lower S curve (concave portion).[14]

- Bizygomatic to bigonial distance is approximately 1:1 in men
Midface augmentation is mainly done for corrective reasons in men, whereas in women it is for addressing signs of aging and enhancing attractiveness.[5] In our experience, however, now even men get treatments done to enhance their attractiveness. It is important to assess patients’ expectations and motivations pre-operatively. Counseling patients regarding the importance of facial proportions can help set realistic expectations of treatment.[15]
TECHNIQUE
In this study, we share our experience of using hyaluronic acid (HA) dermal fillers for midface augmentation in men. Choosing the appropriate filler for each area is important for natural results. Treatment was done on the basis of MD Codes as proposed by de Maio.[16] Areas of treatment included the cheeks, nasolabial folds, and tear troughs. Additionally, temples in the upper face were also addressed if it was required. Local anesthesia cream (PRILOX) was applied for 40 min. After removing the cream, the area was disinfected with chlorhexidine solution.
Before starting midface rejuvenation, it is necessary to see if the temples require fillers for face lift. Injection of fillers in temples significantly lifts not just the midface but also the lower face. When this is followed by injection of filler in the zygomatic arch, the result further improves. The first step is to inject filler in Ck1 or zygomatic arch for lifting the face. Next is to add filler in Ck2 to restore malar projection. The Ck2 point, i.e., zygomatic eminence, is more medial and inferior in men when compared with women.[14] This is followed by final correction of nasolabial fold and tear troughs.
While treating male patients, over projection, excessive height, and fullness of the cheeks must be avoided to prevent feminization.[5] In men, the apex of the cheeks is lower, more medial, and very subtly defined.[14]
The malar eminence was located using Hinderer’s method. The method defines two lines: the first from lateral commissure to the ipsilateral lateral canthus and second line from the ala to the tragus. The intersection point of these two lines represents the apex of the malar eminence[17] [Figure 2]. Another method, known as the Wilkinson method, makes use of a vertical line drawn from the lateral canthus of the eye to the angle of the mandible. The malar eminence is located at about one-third distance down this line[18] [Figure 2].

- (A) Hinderer’s method and (B) Wilkinson’s method
We used Juvederm Voluma (20 mg/mL) for providing structural support and volume to the cheeks. Administration of the filler was done by using supraperiosteal small-bolus injections using a 27G × 8 mm needle. It is mandatory to aspirate before each injection.
The choice of the filler to be used for the nasolabial folds is dependent on the nature of the fold, which may be superficial, moderate, deep, or severe along with redundant skin.[2] While addressing the nasolabial folds, the filler must be injected medially to prevent further deepening of the folds due to ptosis of the cheek.[2] We used Voluma (20 mg/mL) for NL1 and Juvederm Ultra Plus (24 mg/mL) for NL2 and NL3. Injection was done using a retrograde linear thread technique using a 27G × 8 mm needle. Care should be taken not to inject in the deep subcutaneous plane to avoid the angular artery.
In the tear trough region, filler injections should be placed deep along the bony orbital rim. Superficial injections have an increased risk of bruising and chances of the Tyndall effect. JUP (24 mg/mL) was used for the tear troughs. As JUP causes more swelling, small aliquots were injected in the tear troughs in a supraperiosteal plane and massaged gently into place.
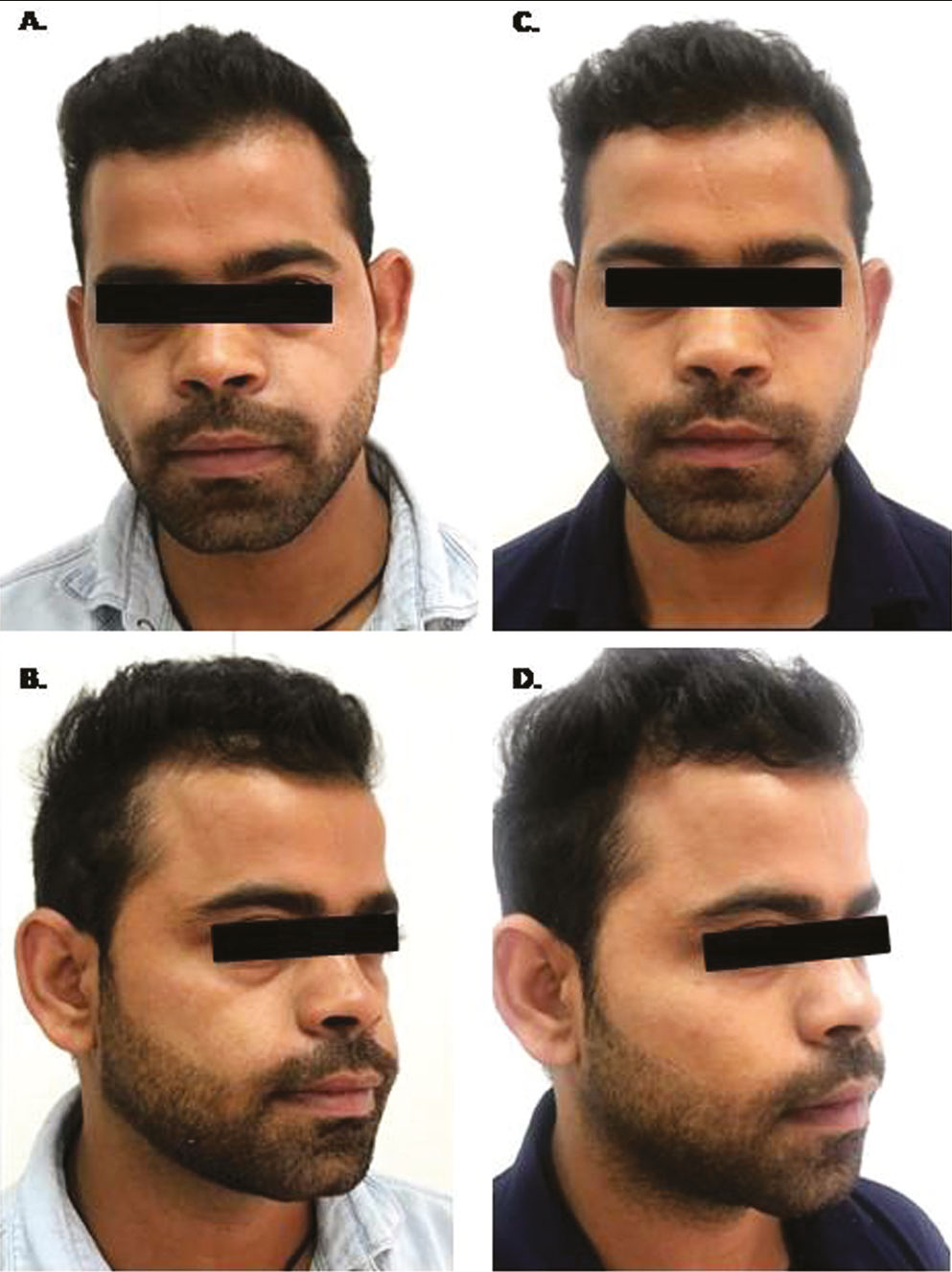
Case 1
A 35-year-old patient wanted to look less tired and more attractive. The treatment plan of the patient was formulated to correct his under-eye hollows and midface to make his face more aesthetically appealing [Table 2 and Figure 3].
| MD Code | Injection area | Product injected | Volume injected (mL) | |
|---|---|---|---|---|
| Right side | Left side | |||
| Ck1 | Zygomatic arch | Voluma | 0.5 | 0.5 |
| Ck2 | Zygomatic eminence | Voluma | 0.3 | 0.3 |
| Nl1 | Upper nasolabial fold | Voluma | 0.2 | 0.2 |
| Tt1, Tt2, Tt3 | Tear trough (central, lateral, medial) | JUP | 0.5 | 0.5 |
| T | Temple | Voluma | 0.5 | 0.5 |

- Case 1: (A) and (B): pre-treatment; (C) and (D): post-treatment
Case 2
A 31-year-old patient wanted to look less tired and more attractive. The treatment plan of the patient was formulated to correct his under-eye hollows and midface to make his face more aesthetically appealing [Table 3 and Figure 4].
| MD Code | Injection area | Product injected | Volume injected (mL) | |
|---|---|---|---|---|
| Right side | Left side | |||
| Ck1 | Zygomatic arch | Voluma | 0.3 | 0.3 |
| Ck2 | Zygomatic eminence | Voluma | 0.2 | 0.2 |
| Tt1, Tt2, Tt3 | Tear trough (central, lateral, medial) | JUP | 0.5 | 0.5 |
| T | Temple | Voluma | 0.5 | 0.5 |
- Case 2: (A) and (B): pre-treatment; (C) and (D): post-treatment
Case 3
A 59-year-old patient wanted to look smarter, less tired, and more youthful. He was looking for a treatment with minimal downtime and subtle results, which would lead to positive aging. Treatment was done focussing on lifting sagging superficial fat pads and correcting hollowness in deep fat pads to lift and re-volumize his face [Table 4 and Figure 5].
| MD Code |
Injection area | Product Injected | Volume Injected (ml) | |
|---|---|---|---|---|
| Right side | Left Side | |||
| Ck1 | Zygomatic arch | Voluma | 0.3 | 0.3 |
| Ck2 | Zygomatic eminence + medial hollowness | Voluma | 0.2 + 0.5 | 0.2 + 0.5 |
| Ck4 | Lateral lower cheek area | Voluma | 0.5 | 0.5 |
| Nl1 | Upper Nasolabial Fold | JUP | 0.2 | 0.2 |
| Nl2, 3 | Central and Lower Nasolabial Fold | JUP | 0.3 | 0.3 |
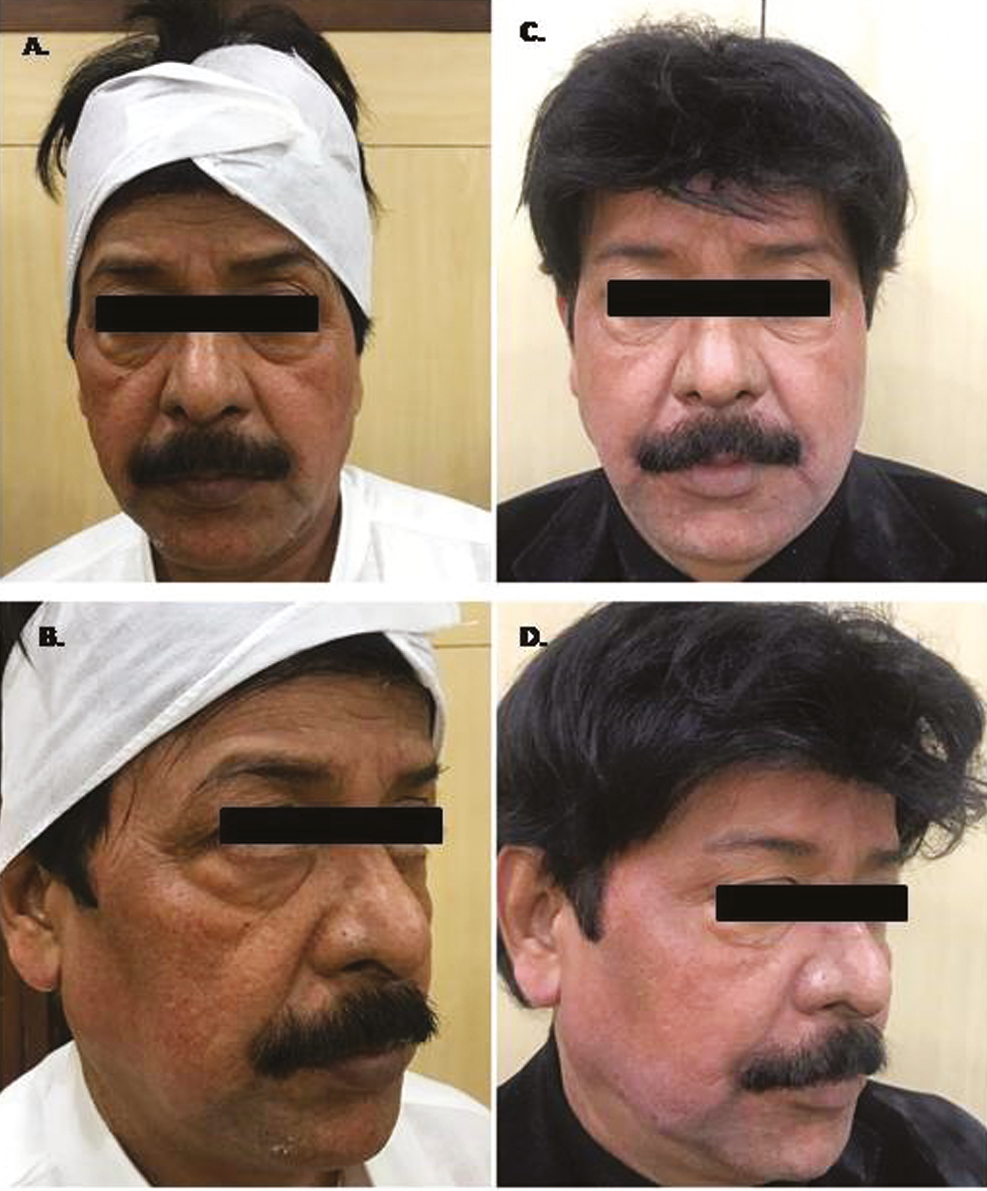
- Case 3: (A) and (B): pre-treatment; (C) and (D): post-treatment
Case 4
A 31-year-old patient wanted to look less tired and smarter. He had concern for under-eye hollowness and deep nasolabial folds. He was suggested midface correction for his concerns [Table 5 and Figure 6].
| MD Code | Injection area | Product injected | Volume injected (mL) | |
|---|---|---|---|---|
| Right side | Left side | |||
| Ck1 | Zygomatic arch | Voluma | 0.3 | 0.3 |
| Nl2 | Central nasolabial fold | Voluma | 0.2 | 0.2 |
| Tt1, Tt2, Tt3 | Tear trough (central, lateral, medial) | JUP | 0.5 | 0.5 |

- Case 4: (A) and (B): pre-treatment; (C) and (D): post-treatment
DISCUSSION
Various studies have taken place in approaches to facial rejuvenation because of increased understanding of facial aging, increase in the types of products available. and refinements in aesthetic goals to provide a balanced, harmonious, and natural look.[19] The development of non-surgical, minimally invasive, office-based procedures with minimal or no downtime has led to more number of men seeking rejuvenating treatments.[2]
The characteristics and features of a male face differ considerably from those of women [Table 6]. As a whole, a male face is squarer in shape compared with the heart-shaped or slightly tapering face seen in females. In the upper third, male facial features are characterized by greater forehead height and width, a prominent supraorbital ridge which slopes backward, giving them a more angled and sharper upper face.[18] In the midface, male cheeks are less projected compared with the fuller, projected round cheeks in a female face.[518] Width of the nasal bridge is greater in men. Lower third of the face in men is characterized by wider mandible, sharper well-defined mandibular angle, well-defined jaw line, and a larger chin with a more forward projection.[518]
| Male | Female | |
|---|---|---|
| Face shape | Square | Heart-shaped |
| Upper face | Greater forehead height and width with prominent supraorbital ridge that slopes backward Eyebrows are flat and straight |
Smaller and smoother forehead Eyebrows are arched Orbit is smaller and more oval but bigger in proportion in relation to the size of the skull |
| Midface | Cheeks are less projected, flatter, and more angular with an even (1:1) projection of medial to lateral cheek Wider glabellar area Wider nasal bridge |
Fuller, projected, round cheeks |
| Lower face | Wider mandible, sharper well-defined mandibular angle, well-defined jaw line (chiseled jaw), and a larger chin with more forward projection | Narrower mandible Chin is slightly posterior to the lower lip |
| Facial musculature and skin | Greater muscle mass. Thicker epidermis and dermis. Subcutaneous adipose layer is less prominent. |
Subcutaneous adipose layer is thicker with thinner epidermis and dermis and lesser muscle mass. |
While some amount of bony resorption occurs with age, it is the overlying soft tissue contours that give rise to the characteristic differences in the surface contours in the male and female cheek. A pair of studies used magnetic resonance imaging to quantify the differences in subcutaneous facial fat in men and women as well as their changes with age. The studies showed that overall the male face has a thinner layer of subcutaneous fat, but the fat distribution in the male cheek is uniform. On the contrary, the female cheek has a thicker fat compartment medially when compared with the lateral area, with a ratio of 1.5:1.[2021] This uneven distribution of fat explains why a female cheek is rounder and fuller, and the male cheek is flatter and more angular.[2021] The malar eminence represents the area of maximal projection of the cheek. Men also have a thicker epidermis and dermis compared with women, whereas the subcutaneous adipose tissue is less prominent.[14]
HA fillers (Juvederm, Allergan, Irvine, CA, USA and Restylane, Galderma, Fort Worth, TX, USA) are widely used for augmentation of the midface. With an increased knowledge and understanding of the properties of HA, such as stiffness (G'), cohesivity, longevity, water absorption, crosslinking, and response to hyaluronidase, physicians are better equipped to treat different anatomical areas.[1822] It is preferred to use soft gels for more superficial use and stiffer products for deeper injections. The type of skin also plays an important role in dictating the choice of the product.[19]
Juvederm Voluma is the ideal option for augmentation of cheeks due to its lifting capacity.[23] The higher stiffness (G') and lesser swelling of Voluma facilitate tissue support and make it appropriate for deeper injections, where a change in volume is required along with support to overlying tissues.[24] Depending on the individual case, Voluma has the versatility to be injected both subcutaneously and supraperiosteally and may be layered depending on the deficit.[2324] An observational, prospective study found that Juvederm Voluma was well accepted by both male and female subjects, with high levels of satisfaction, and was well tolerated and smooth and easy to use when used for the midface volume enhancement.[25]
In the tear trough region, it is advised to use a thinner HA filler to prevent uneven contour irregularities. Fillers that are less hydrophilic are preferred to avoid post-injection swelling.[18] We used JUP for the tear trough region. JUP is a Hylacross product with high cohesivity and degree of cross-linking of HA, which increases its longevity up to a period of 1 year. It has a softer, smoother, and a more natural feel compared with the granular or particulate consistency seen with other HA fillers, making it suitable for tear trough.
Changes in the nasolabial folds may range from superficial lines, deep rhytids to grooves as a result of ptosis of the cheek. It is therefore recommended to begin with augmentation of the zygoma before approaching nasolabial folds.[14] Superficial lines can be treated using Juvederm Ultra Plus by linear threading subdermally, whereas deeper grooves can be augmented by Juvederm Voluma or Ultra Plus on the bone. In a double-blinded, randomized study, Li et al.[26] found Juvederm Ultra Plus to be safe and effective in treating severe nasolabial folds. In a study by Goodman et al.,[27] JUP exhibited greater longevity while treating the nasolabial folds and was well tolerated.
For midface rejuvenation in middle-aged and older individuals, we start with correction of T1 to delay aging, then the lateral point Ck1 for lift followed by zygomatic hollowness, and finally the tear trough and nasolabial folds.
It is believed that complications in many instances may arise as a result of technique rather than due to product characteristics.[19] Complications with filler injections may be reduced by the slow rate of injection and use finer-gage needles.[19] Following midface rejuvenation, common complications such as redness, bruising, tenderness, and swelling were observed. The most serious complication of injectable dermal fillers is vascular compromise, which can lead to skin necrosis if it goes unnoticed or untreated.[28] Other potential complications include infection and foreign body granuloma formation.[13] In a male patient, the most undesirable consequence can be feminization of the face. A careful patient evaluation, use of adequate product and technique, coupled with a thorough knowledge of facial anatomy,[29] and differences with female facial characteristics are required for proper results.
CONCLUSION
Use of injectable HA dermal fillers is a safe, effective, and well-tolerated non-surgical treatment modality for midface rejuvenation in men. While treating the midface, it is important to understand the aesthetic needs of a male patient. Today, men seek treatment not just for correction and positive aging but also to enhance their attractiveness. It is necessary to counsel the patient adequately and arm yourself with thorough knowledge of the midface anatomy, injection techniques, and properties of individual fillers along with an understanding of the considerations in facial features of men to make injectable dermal fillers a rewarding treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Dr. Anupriya Goel is a trainer with Allergan but has not received any funding/support for this study.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: Focus on the midface. Plast Reconstr Surg. 2017;140:540e-50e.
- [Google Scholar]
- Midface injectable fillers: Have they replaced midface surgery? Facial Plast Surg Clin North Am. 2013;21:229-39.
- [Google Scholar]
- The minimal approach: An innovation in facial cosmetic procedures. Aesthet Plast Surg. 2004;28:295-300.
- [Google Scholar]
- Ethnic and gender considerations in the use of facial injectables: Male patients. Plast Reconstruct Surg. 2015;136(5S):40S-3S.
- [Google Scholar]
- Midface anatomy, aging, and aesthetic analysis. Facial Plast Surg Clin North Am. 2015;23:129-36.
- [Google Scholar]
- Surgical anatomy of the midcheek: Facial layers, spaces, and the midcheek segments. Clin Plast Surg. 2008;35:395-404; discussion 393.
- [Google Scholar]
- Anatomic and aesthetic considerations in midfacial rejuvenation. Facial Plast Surg. 2006;22:105-11.
- [Google Scholar]
- Changes in the facial skeleton with aging: Implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2020;44:1151-8.
- [Google Scholar]
- Aging of the facial skeleton: Aesthetic implications and rejuvenation strategies. Plast Reconstr Surg. 2011;127:374-83.
- [Google Scholar]
- Injectables and fillers in male patients. Facial Plast Surg Clin North Am. 2008;16:345-55.
- [Google Scholar]
- Midfacial analysis and planning for midface augmentation with injectable filling materials: An anatomical approach. J Eur Acad Dermatol Venereol. 2012;26:714-8.
- [Google Scholar]
- Nonsurgical jawline rejuvenation using injectable fillers. J Cosmet Dermatol. 2020;19:1940-7.
- [Google Scholar]
- Injectable cosmetic procedures for the male patient. J Drugs Dermatol. 2015;14:1043-51.
- [Google Scholar]
- Role of nonsurgical chin augmentation in full face rejuvenation: A review and our experience. Dermatol Surg. 2018;44:985-93.
- [Google Scholar]
- MD Codes™: A methodological approach to facial aesthetic treatment with injectable hyaluronic acid fillers. Aesthet Plast Surg. 2021;45:690-709.
- [Google Scholar]
- Malar implants for improvement of the facial appearance. Plast Reconstr Surg. 1975;56:157-65.
- [Google Scholar]
- Facial soft tissue augmentation in males: An anatomical and practical approach. Dermatol Surg. 2017;43:S131-9.
- [Google Scholar]
- Advances in facial rejuvenation: Botulinum toxin type A, hyaluronic acid dermal fillers, and combination therapies—Consensus recommendations. Plast Reconstr Surg. 2008;121:5S-30S.
- [Google Scholar]
- Quantifying soft tissue loss in the aging male face using magnetic resonance imaging. Dermatol Surg. 2014;40:786-93.
- [Google Scholar]
- Quantifying soft tissue loss in facial aging: A study in women using magnetic resonance imaging. Dermatol Surg. 2013;39:1895-902.
- [Google Scholar]
- Effective rejuvenation with hyaluronic acid fillers: Current advanced concepts. Plast Reconstr Surg. 2019;143:1277e-89e.
- [Google Scholar]
- Midface: Clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136:219-34S.
- [Google Scholar]
- Current concepts in the use of Voluma, Volift, and Volbella. Plast Reconstr Surg. 2015;136:139S-48S.
- [Google Scholar]
- A prospective, observational study of the volumizing effect of open-label aesthetic use of Juvéderm® VOLUMA® with lidocaine in mid-face area. J Cosmet Laser Ther. 2014;16:171-9.
- [Google Scholar]
- Safety and effectiveness of Juvéderm Ultra Plus injectable gel in correcting severe nasolabial folds in Chinese subjects. Plast Reconstr Surg Glob Open. 2017;5:e1133.
- [Google Scholar]
- A comparison of the efficacy, safety, and longevity of two different hyaluronic acid dermal fillers in the treatment of severe nasolabial folds: A multicenter, prospective, randomized, controlled, single-blind, within-subject study. Clin Cosmet Investig Dermatol. 2011;4:197-205.
- [Google Scholar]
- Midface volumization with injectable fillers. Facial Plast Surg Clin. 2015;23:233-42.
- [Google Scholar]
- Facial contouring by using dermal fillers and botulinum toxin A: A practical approach. Aesthetic Plast Surg. 2019;43:793-802.
- [Google Scholar]




