
Translate this page into:
A Comparative Study to Evaluate the Efficacy of Fractional CO2 Laser + PRP Vs. Fractional CO2 Laser Alone in Patients with Vitiligo
Address for correspondence: Dr. Rajkumar Kothiwala, Room 202, RUHS Resident Hostel, Jaipur, Rajasthan 302033, India. E-mail: rajkumar.kothiwala@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Introduction:
Vitiligo is a multifactorial acquired disorder clinically characterized by amelanotic lesions on the skin, due to destruction of melanocytes. The course of vitiligo is unpredictable. Vitiligo causes significant psychological impact and cosmetic disfigurement. Treatment of vitiligo is challenging and requires a multidisciplinary approach.
Materials and Methods:
A prospective comparative interventional study was carried out from October 2018 to March 2020. The study enrolled 60 stable vitiligo patients divided into groups A and B. Group A (30 patients) was treated with both fractional CO2 laser and autologous platelet-rich plasma (PRP) injection. Group B (30 patients) was treated with fractional CO2 laser alone. A total of four sessions were conducted in each group at 1-month interval along with photographic assessment. Final assessment was done 1 month after the completion of four sessions.
Results:
In group A, the median values of repigmentation and visual-analog score (VAS) were 3 and 7, and in group B, the median values of repigmentation and VAS were 1 and 2, respectively. Lesions over the trunk showed the best response followed by face and extremities lesions. Acral lesions showed the least response.
Conclusion:
A combination of fractional CO2 laser and PRP is superior to fractional CO2 laser alone in the treatment of stable vitiligo.
Keywords
Fractional CO2 laser
platelet-rich plasma
vitiligo

INTRODUCTION
Vitiligo is an acquired, idiopathic disorder clinically characterized by amelanotic lesions on the skin, due to destruction and subsequent absence of melanocytes.[1] It is characterized by milky-white sharply demarcated macules.[2] It affects 0.5–1% of the world’s population.[3] Prevalence is same in both sexes.[4]
Vitiligo is a multifactorial disorder related to both genetic and non-genetic factors. Pathogenic causes are multifactorial, including genetic, dysfunctional biochemical pathways, autoimmune processes, melanocyte adhesion deficits, and nervous system imbalances.[45] CD8+ T cells play a critical role during the progression of vitiligo. Lasers are the most precise and selective surgical tool.
CO2 is a gas-type laser with a wavelength of 10,600 nm. Fractional CO2 lasers have originally been developed for tissue rejuvenation and scar remodeling.[6] Treatment of vitiligo is challenging and requires a multidisciplinary approach. Fractional carbon dioxide laser as an add-on to conventional treatment has been reported to be effective, but there is no consensus on its use.
Platelet-rich plasma (PRP) is an autologous plasma fraction of peripheral blood with concentration of autologous platelets providing multiple growth factors, suspended in a small amount of plasma, after centrifugation.[78] PRP promotes the release of inflammatory mediators and modulators. PRP represents a new biotechnology. It is simple, cheap, and easily available. So far PRP therapy and fractional CO2 lasers have not been utilized and studied in vitiligo on a large scale.
MATERIALS AND METHODS
This comparative interventional study has been carried out in the Department of Dermatology, Venereology, and Leprosy, from October 2018 to March 2020 at JLN Medical College and Group of Hospitals, Ajmer, Rajasthan, India, after taking approval from the Ethics Committee. The study enrolled 60 patients of stable vitiligo for the last 1 year, of either sex with different age groups, satisfying inclusion and exclusion criteria. Patients were divided into groups A and B. No financial implications were imposed on patients. No conflicts of interest noted.
In group A, 30 patients were treated with fractional CO2 laser and intradermal injections of autologous PRP prepared from patient’s own blood once a month after all aseptic precautions.

In group B, 30 patients were treated with fractional CO2 laser once a month. We used point energy between 70 and 100 MJ, power 20 W, duration 5 ms, interval 4 ms, distance 0.7 mm, scan mode normal, three times.
The patients were advised to protect from direct exposure to sunlight in the initial 5 days and to expose the area to sun daily for 10–15 min after that.
Fractional CO2 laser and PRP were the only modes of treatment used. Combination with psoralens or other immunomodulators was not used in the study.
Four sessions were done at a 30-day interval along with photographic assessment. Final assessment was done 1 month after the completion of four sessions.
Patients were followed up for a total of 5 months.
Fr: CO2laser machine

Evaluation of treatment: Both groups were followed up and evaluated by repigmentation in the patch of vitiligo.
Mean improvement score by physician (MISP)
MISP was calculated by comparing the photographs. Clinical assessments were done by two blinded dermatologists using a quartile grading scale.
No response Grade 0
Poor improvement (< 25%) Grade 1
Fair improvement (26–50%) Grade 2
Good improvement (51–75%) Grade 3
Excellent improvement (>75%) Grade 4
Complete Grade 5
Patients’ satisfaction
Patients rated their satisfaction at the end of the study using a 10-point VAS (0–10: a level of 0 for “not satisfied at all,” whereas a level of 10 for “completely satisfied”).
Statistical analysis
Data were entered in MS Excel and analysis was carried out in terms of mean ± standard deviation (SD), median, and range for quantitative variables. For categorical variables, data were represented in terms of frequencies (number of cases) and percentages. Analyses of demographic characteristics were done using unpaired t-test for quantitative variables, whereas the χ2 test was used for categorical variables. Comparison of numerical variables between the study groups was performed using the Mann–Whitney U-test for comparing two groups and the Kruskal–Wallis test for comparing more than two groups. P-values less than 0.05 were considered statistically significant.
RESULTS
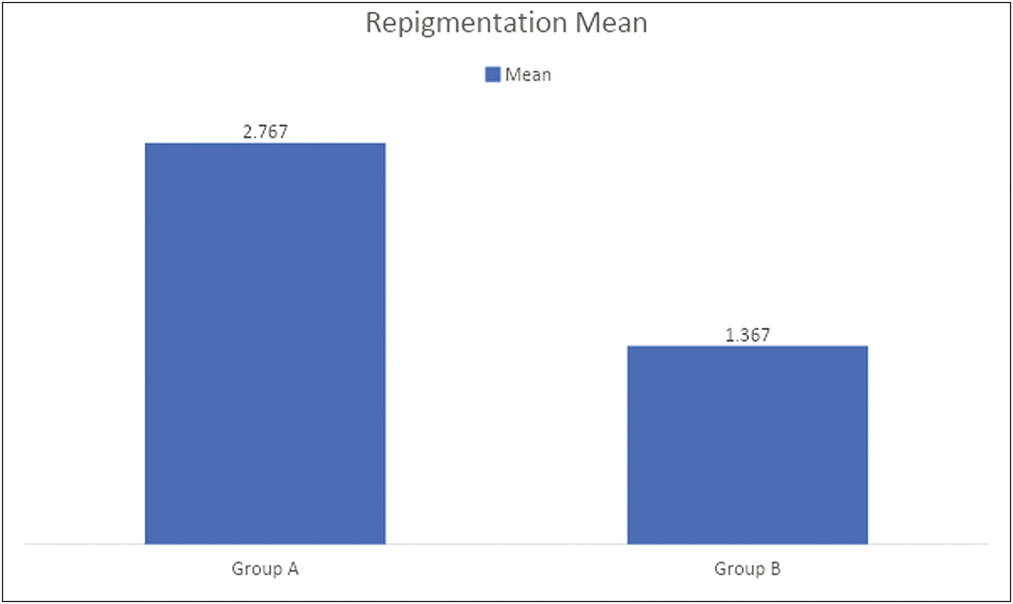
In group A, MISP was 2.76 ± 1.546 and in group B MISP was 1.367 ± 1.067. The Mann–Whitney test was performed. The P-value is 0.00023. The result is significant at P < 0.05 [Table 1].
| Groups | Mean | SD | Mean differences |
|---|---|---|---|
| A (N=30) Fractional carbon dioxide laser plus PRP |
2.767 | 1.546 | 1.4 |
| B (N=30) Fractional carbon dioxide laser |
1.367 | 1.067 |
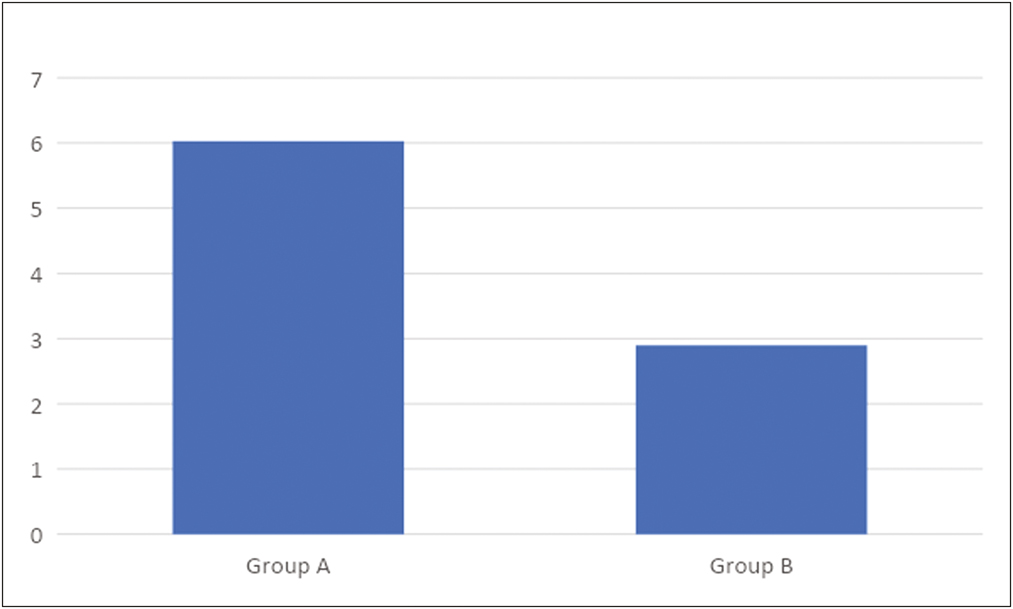
In group A, the mean score of VAS was 6.03 ± 3.31 and in group B the mean score of VAS was 2.9 ± 2.38. The P-value is 0.00038, which is significant at P < 0.05 [Table 2].
| Groups | Mean | SD | Mean differences |
|---|---|---|---|
| A (N=30) Fractional carbon dioxide laser plus PRP |
6.03 | 3.31 | 3.13 |
| B (N=30) Fractional carbon dioxide laser |
2.9 | 2.38 |
Side effects
In group A, erythema was seen in 93.33%, burning in 63.33%, pain in 6.66%, and hyperpigmentation in 3.33% of the patients.
In group B, erythema was seen in 86.66%, burning in 66.66%, pain in 40%, and hyperpigmentation in 10% of the patients.
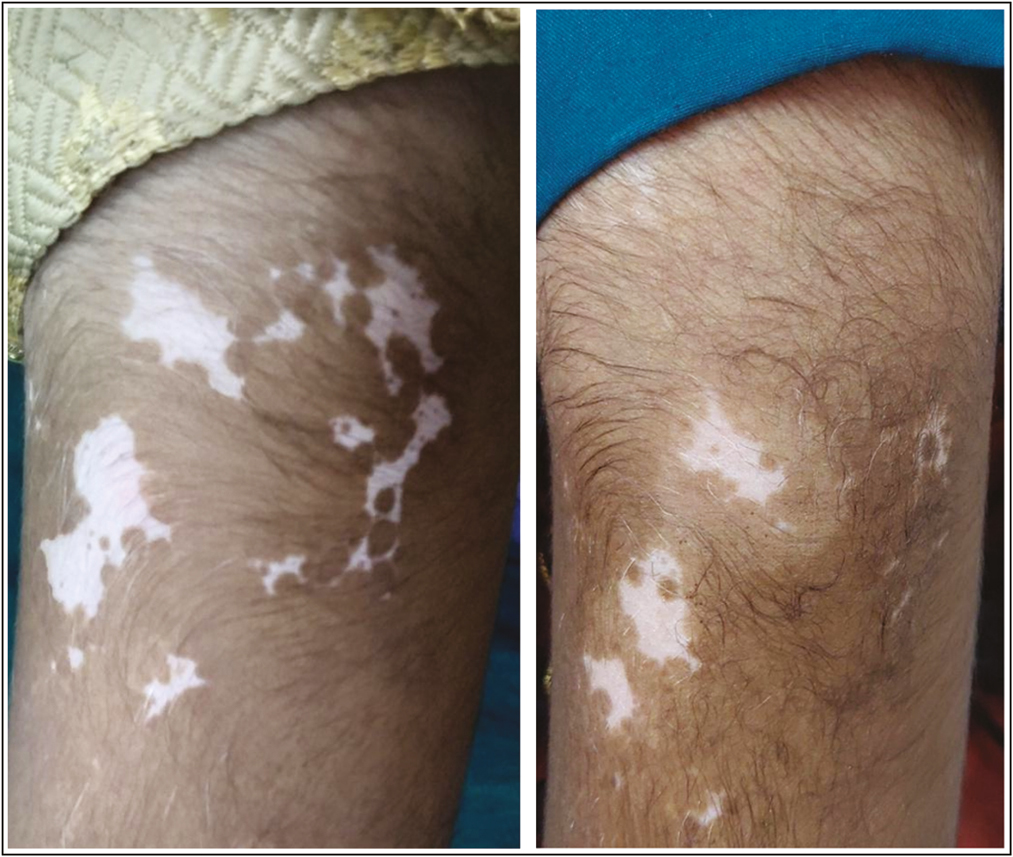
Group A

Group B
DISCUSSION
We conducted this prospective comparative study to evaluate the efficacy and safety of fractional CO2 laser with PRP and fractional CO2 laser in the treatment of stable vitiligo for the last 1 year.
Mean age in group A was 27.46 ± 8.91 years and in group B the mean age was 29.86 ± 11.10 year, which is similar to the study conducted by Abdelghani et al.[9] [Table 3].
| Groups | Age (years) | P-value | ||
|---|---|---|---|---|
| Mean | Standard deviation | Mean differences | ||
| Group A (N=30) | 27.46 | 8.91 | 2.4 | 0.546 (NS) |
| Group B (N=30) | 29.86 | 11.10 | ||
In our study, 56.6% of the patients were females and 43.3% of the patients were males in group A and in group B 50% of the patients were females and 50% were males, which depicts a slight female preponderance similar to the study conducted by Abdelghani et al. and the study conducted by Kadry et al.[10] [Table 4]. In our study, mean age of onset in group A was 21.63 years and in group B was 22.8 years [Table 5].
| Groups | Gender | Total | P-value | |
|---|---|---|---|---|
| Female | Male | |||
| Group A | 17 (56.6%) | 13 (43.3%) | 30 | 1.000 (NS) |
| Group B | 15 (50%) | 15 (50%) | 30 | |
| Total | 32 | 28 | 60 | |
| Groups | Age at onset (years) | P-value | ||
|---|---|---|---|---|
| Mean | Standard deviation | Mean differences | ||
| A (N=30) | 21.63 | 9.59 | 1.17 | 0.713 |
| B (N=30) | 22.8 | 14.44 | ||
We noted in group A, 13% of the patients (4) had duration <2 years and 87% patients (26) had vitiligo for more than 2 years. Whereas in group B, 17% of the patients (5) had duration less than 2 years and 83% of the patients had duration more than 2 years, which is in concordance with the study by Abdelghani et al. in which there was a higher percentage (60% with >2 years vs. 40% with <2 years) of patients with duration more than 2 years signifying the chronicity of the disease [Table 6].
| Groups | Duration (years) | ||
|---|---|---|---|
| Mean | SD | Mean differences | |
| A (N=30) | 5.9 | 3.52 | 2.23 |
| B (N=30) | 8.13 | 6.57 |
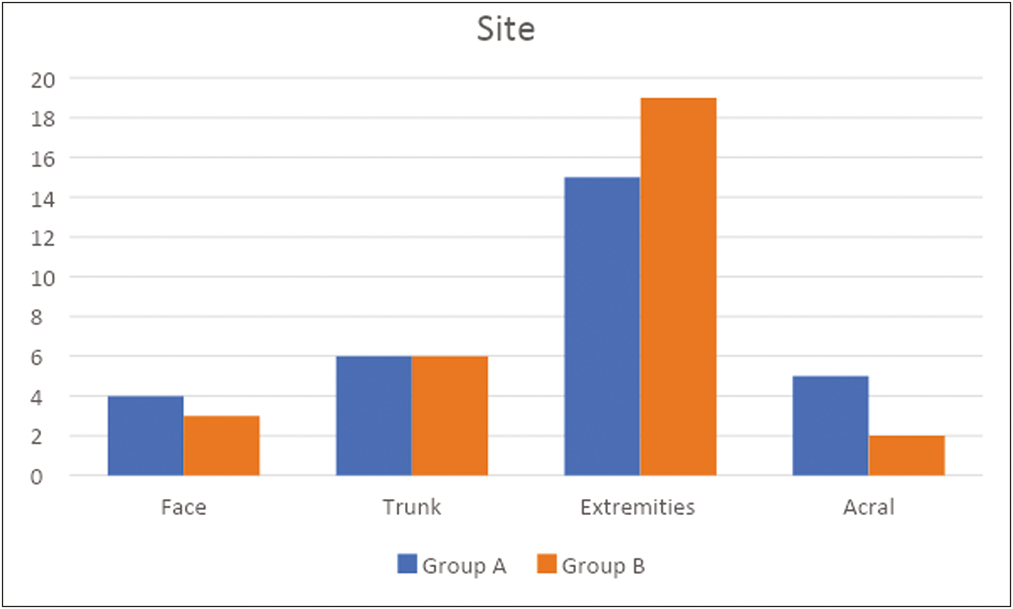
In group A, vitiligo patches were selected in the following order: extremities in 50% of the patients, trunk in 20%, acral in 16.66%, and face in 13.33%, whereas in group B vitiligo patches selected on extremities in 63.33%, trunk in 20%, face in 10%, and acral in 6.67% of the patients [Table 7].
| Site | Total | ||||
|---|---|---|---|---|---|
| Groups | Face | Extremities | Acral | Trunk | |
| A | 4 (13.33 %) | 15 (50%) | 5 (16.66%) | 6 (20%) | 30 |
| B | 3 (10%) | 19 (63.33%) | 2 (6.66%) | 6 (20%) | 30 |
| Total | 7 (11.66%) | 41 (56.66%) | 7 (11.66%) | 12 (20%) | 60 |
In the study by Abdelghani et al., the most common sites selected were face (40% in the laser + PRP group and 40% in the laser group), extremities (35% in the laser + PRP group and 25% in the laser group), trunk (10% in the laser + PRP group and 20% in the laser group), and acral (15% in the laser + PRP group and 15% in the laser group).
Site selection was slightly different from our study, which may be due to geographic variation.
In 2018, Abdelghani et al. studied the effect of combined treatment with fractional CO2 laser, PRP, and NB-UVB for stable non-segmental vitiligo. The laser and PRP group achieved best results regarding repigmentation and patients’ satisfaction. About 60% of the patients developed repigmentation >50%, and 40% of the patients developed repigmentation >75%. In the laser and NB-UVB group, 5% developed repigmentation >75%, and 25% developed repigmentation >50%. Only 10% of the patients developed repigmentation >75% in the laser group and only 20% of the patients developed repigmentation >75% in the PRP group. They concluded that Fr: CO2 laser with PRP injection was a promising treatment for vitiligo, followed by a combination of Fr: CO2 laser with NB-UVB phototherapy. Both fractional CO2 laser and PRP injection gave poor results if they received alone.
In our study, fractional CO2 laser with PRP achieved better results than fractional CO2 laser alone. In group A, excellent response was shown by 26.67%, followed by good response in 20%, fair in 16.67%, complete in 13.33%, and then no response in 10% of the patients. Around 60% of the patients developed repigmentation more than 50%, and 40% showed repigmentation more than 75%. In group B, poor response was seen in 60% of the patients, followed by no response in 16.67%, fair in 10%, good in 10%, complete in 3.33%, and excellent in zero patients. Only 13.33% of the patients had repigmentation more than 75%, and 23.33% showed repigmentation more than 50%.
In another study conducted by Kadry et al., the following findings were observed.
In the combined Fr: CO2 with PRP group, the median values of repigmentation and VAS were 3.50 and 7.50, respectively.
Lesions over the face showed best response followed by acral lesions and truncal lesions. Feet and LL lesions showed less response.
In the laser group, the median values of re-pigmentation and VAS were 2.00 and 5.00, respectively. Lesions over the trunk showed best response followed by lesions over extremities and face. Acral lesions showed no response.
In our study in the combined Fr: CO2 with PRP group, the median values of repigmentation and VAS were 3 and 7, respectively, similar to the above study.
In the laser group, the median values of re-pigmentation and VAS were 1 and 2, respectively.
There was no case of Koebnerization in either group.
In terms of side effects, pain was significantly higher in group A (40%) than in group B (6.66%) [Table 8].
| Group | Erythema (%) | Burning (%) | Pain (%) | Hyperpigmentation (%) |
|---|---|---|---|---|
| A | 93.33 | 63.33 | 6.66 | 3.33 |
| B | 86.66 | 66.66 | 40 | 10 |
Post-inflammatory hyperpigmentation was seen in a smaller percentage of patients in both the groups and it was seen mainly on photoexposed sites. Hyperpigmentation did not subside on its own.
Lesions over the trunk showed best response followed by face lesions and extremities lesions. Acral lesions showed the least response.
CONCLUSION
We observed that the combination of Fr: CO2 laser and PRP is superior to Fr:CO2 laser alone in the treatment of stable vitiligo.
Side effects noted were transient erythema, burning sensation, PIH after fractional CO2 laser.
Current literature is lacking in enough comparative studies on fractional CO2 laser along with PRP and FR:CO2 laser alone. More studies having larger sample size and longer follow-up period with more sessions are needed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Use of platelet-rich plasma to suspend noncultured epidermal cell suspension improves repigmentation after autologous transplantation in stable vitiligo: A double-blind randomized controlled trial. Int J Dermatol. 2019;58:472-6.
- [Google Scholar]
- Revised classification/nomenclature of vitiligo and related issues: The Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25:E1-13.
- [Google Scholar]
- Koebner’s phenomenon in vitiligo: European position paper. Pigment Cell Melanoma Res. 2011;24:564-73.
- [Google Scholar]
- Innate immune mechanisms in vitiligo: Danger from within. Curr Opin Immunol. 2013;25:676-82.
- [Google Scholar]
- Triple combination treatment with fractional CO2 laser plus topical betamethasone solution and narrowband ultraviolet B for refractory vitiligo: A prospective, randomized half-body, comparative study. Dermatol Ther. 2015;28:131-4.
- [Google Scholar]
- Platelet-rich plasma and its utility in medical dermatology: A systematic review. J Am Acad Dermatol. 2019;81:834-46.
- [Google Scholar]
- Combined treatment with fractional carbon dioxide laser, autologous platelet-rich plasma, and narrow band ultraviolet B for vitiligo in different body sites: A prospective, randomized comparative trial. J Cosmet Dermatol. 2018;17:365-72.
- [Google Scholar]
- Platelet-rich plasma versus combined fractional carbon dioxide laser with platelet-rich plasma in the treatment of vitiligo: A comparative study. Clin Cosmet Investig Dermatol. 2018;11:551-9.
- [Google Scholar]




