
Translate this page into:
Hole-retaining Lobeplasty for Type I Ear Lobe Deformities
Address for correspondence: Dr. Lekshmi S. Bhooshan, Department of Plastic Surgery, Government Medical College, Kottayam, Kerela, India E-mail: lekshmibhooshan@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
The aesthetic aspect of Type I incomplete split ear lobe is underestimated. Most of the hole-retaining techniques described for large and split ear lobes are difficult to perform in Type I deformity.
Aim:
(1) To conduct a pilot study based on the postoperative review of the cases of Type I ear lobe deformities surgically managed with hole-retaining lobeplasty in a tertiary care centre in South India.
(2) To assess the postoperative outcome of the hole retaining lobeplasty based on the Global aesthetic improvement scale and Patient satisfaction in Likert scale.
Materials and Methods:
A pilot study of hole-retaining lobeplasty technique was done based on the postoperative review of 6 patients with bilateral type1 incomplete split ear lobes who were operated in our institution with the same. The results were validated based on descriptive statistics and postoperative outcomes using GAIS score and Patient Satisfaction Score measured in a Likert scale.
Results:
None of the patients had any postoperative complications. At six months follow up, all patients had centrally placed, circular ear holes, well settled support flap and rounded lobe contour with an average GAIS score of 4.83 ± 0.38. All the patients were satisfied with their newly created ear hole and lobe contour, with an average Patient Satisfaction Score of 4.8 ± 0.4
Conclusion:
Hole- retaining lobeplasty is a simple, cost effective, single staged, day-case procedure for repair of Type I large ear holes, that can be easily duplicated by young plastic surgeons with is aesthetically better, circular and centrally placed ear hole with a more rounded ear lobe with support to prevent recurrence.
Keywords
Ear hole repair
hole-retaining
large ear hole
lobeplasty

INTRODUCTION
Ear lobe piercing is a practice that dates back to centuries. It is used as a form of sexual orientation, a statement of social status, graceful aging and mostly as a form of fashion.
Wide ear holes are more commonly seen in individuals wearing heavy and/or pendulous ear jewelry. Studies have reported a 1%–2% incidence rate of torn ear lobes in patients wearing ear jewelry.[12] Chronic traction on the earlobe by the jewelry results in atrophy of tissue and gradual widening of the ear hole and subsequently split ear lobe.[3] The various other complications of ear lobe piercing include infection, keloid formation.[4]
An aesthetically normal ear-hole may be central in the ear lobe, circular and should snuggly fit a stud or an earring. Agarwal and Chandra, proposed a classification of acquired cleft ear lobe deformity in 2008;[5] wherein cleft ear lobe deformity is divided into
Type I (stretched out ear hole more than twice the original diameter),
Type II (near total split leaving a thin rim of lobe remaining),
Type III (completely split ear lobe),Type IV (total split of ear lobes with fibrosis and retraction of margins) and
Type V (single/multiple tears on the earlobe with fibrosis and scarring)
The cosmetic problem of Type I ear lobe deformity is usually underestimated. The deformity is ignored if the person prefers large ear studs or hanging ear jewelry. Further, with continued use of large studs or hanging jewelry, these holes stretch over time and eventually progress to Type II to V ear hole deformities. The Type I large ear hole becomes problematic when the person prefers wearing small ear studs wherein the studs will be either loosely fit or fall off through the large hole [Figure 1].
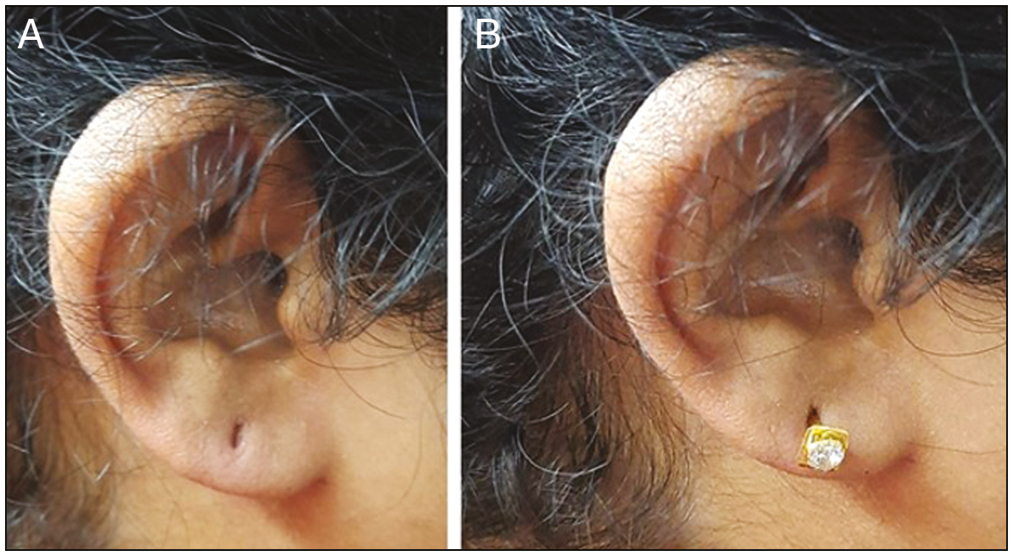
- (A) Type 1 incomplete cleft ear lobe. (B) Ear stud dangling from the ear hole
There are multiple surgical techniques described in literature for the management of Type II to V ear hole deformities.[26] But there is paucity of literature for the surgical techniques for the management of Type I ear lobe deformity. Most commonly done procedure is primary closure of the original hole and re-piercing at a later date.[67] This may require multiple hospital visits and procedures. Hole retaining flap surgeries like Pardue flap[8] are difficult to do in Type I earholes unless the lobe is stretched and the hole is very large and elongated (Type II).
Other techniques such as the Half Z plasty[9] and Hammock flap technique[10] have been described for large ear holes, which involve the use of Z flaps for the recreation of the ear hole, breakage of scar line and restoration of the lobule contour. However, these techniques are difficult to perform in Type I ear lobes. The other drawbacks of these techniques include the oblique orientation of the hole and unaesthetic lengthening and pointing of the ear lobes.[10] An ideal method for ear lobe repair should recreate a central aesthetically pleasing circular ear hole with good ear lobe contour and should have least chance of recurrent tear.[5]
MATERIALS AND METHODS
The aim of our study was to conduct a pilot study of hole- retaining lobeplasty technique based on the postoperative review of patients with Type I ear lobe deformity who underwent the repair, and to assess the postoperative outcome based on the GAIS score and Patient satisfaction in the Likert scale.
A total of 6 patients who had undergone hole- retaining lobeplasty for Type I ear hole deformity (Type I Agarwal and Chandra Classification) during a two year period between 2018 and 2020 in our institution were included in the study. All the patients had bilateral wide ear holes and hence total twelve ear lobes of six patients were operated under local anesthesia using the below mentioned hole-retaining lobeplasty technique by the principal investigator. Instituition Review Board permission was also obtained.
At postoperative follow up, the patients were reassessed by surgeons using Global Aesthetic Improvement Scale (GAIS) which is a five-point scale, i.e., 5 - very much improved, 4- improved, 3- No change, 2-worse and 1- much worse[11] The patient satisfaction was assessed using a five-point likert scale; 5- very much satisfied, 4-satisfied, 3- good, 2- fair and 1- poor.
The results were validated based on descriptive statistics and postoperative outcomes were assessed using GAIS score and Patient Satisfaction Score measured in a Likert scale and photographic comparison. Statistics was done with SPSS version 16 Chicago inc.and Microsoft Excel.
SURGICAL TECHNIQUE
Demonstrative case
The technique described as Hole-retaining lobeplasty is a modification of the Abenavoli’s half Z plasty technique.[9] The technique is a two flap technique planned like Z-plasty with slightly curved limbs, with the central limb on the ear hole [Figure 2]. The ear-hole facing limb of the superiorly based flap forms the future earhole and that of the inferiorly based flap is de-epithelialized. The full thickness flaps are incised. The apex of the superiorly based flap is rolled and sutured to the skin on the superior part of the ear hole. Thus the skin on the hole facing limb of the superiorly based flap forms the new ear hole which is circular and more centrally placed on the ear lobe. The inferiorly based flap with the de-epithelised hole facing limb forms the support flap for the new ear hole and is sutured around the ear hole. This technique differs from the classical Z-plasty in that, the apex of the superiorly based flap is not sutured to the base of the inferiorly based flap. By this technique, the longitudinally elongated ear hole will be reduced in size and will attain a circular shape and the hole will be pushed more centrally which is aesthetically more acceptable. The inferiorly based flap will act as a support flap prevents further scar elongation and recurrence in future. The flaps were sutured with 5-0 polypropylene suture and a spacer made from a 16G intravenous cannula sheath is placed within the newly formed ear hole like a spacer.
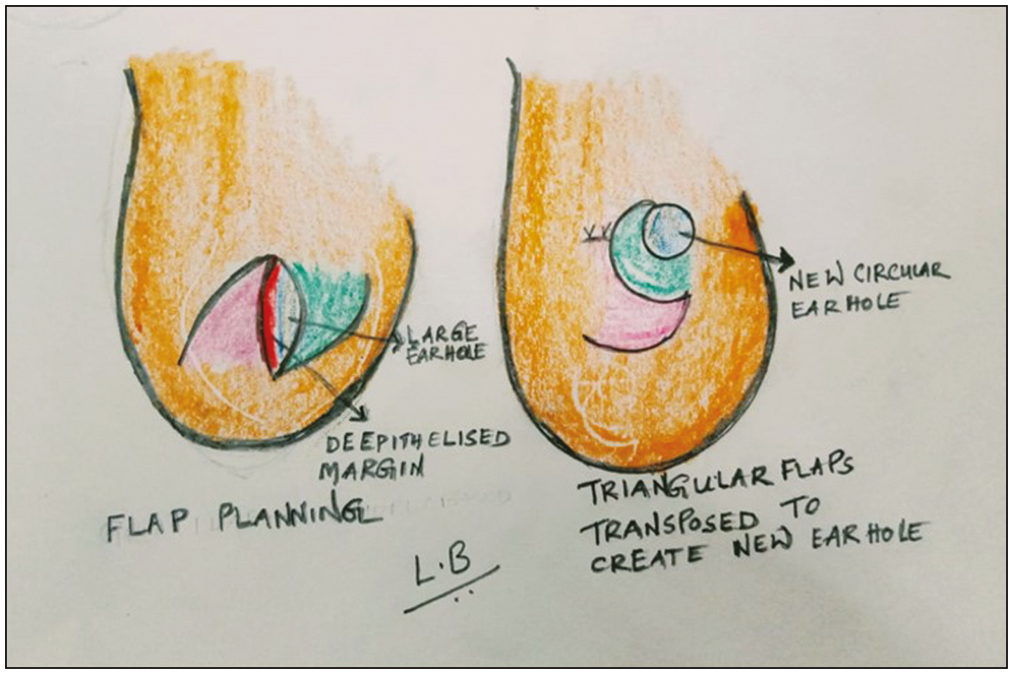
- Schematic diagram showing the flap design and final appearance of ear lobe
The flap planning, intraoperative photos and postoperative photos of the representative cases are shown in the [Figures 3A, 3B, 4A and B].
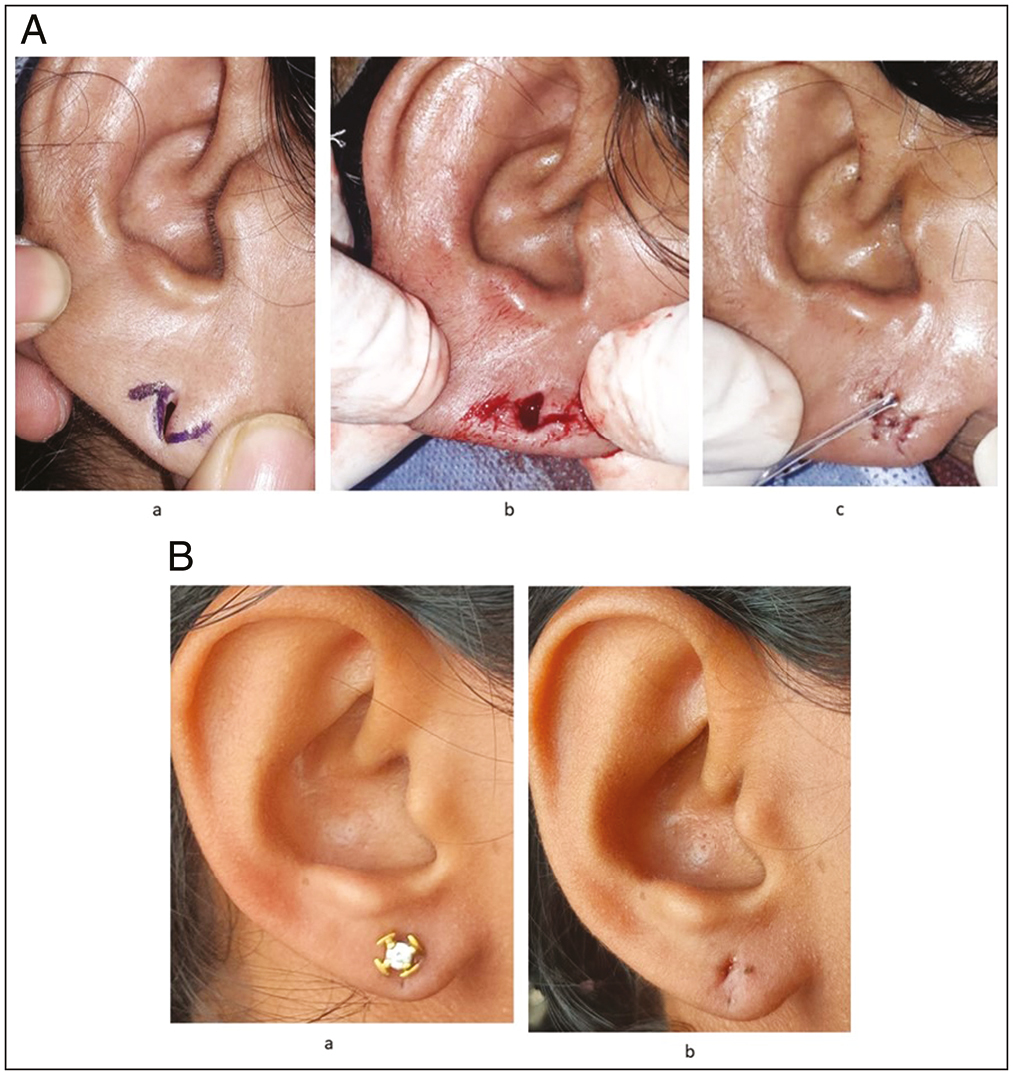
- (A) Representative Case 1: (a) flap design, (b) flaps raised, and (c) after flap inset with spacer. (B) Postoperative results of representative Case 1: (a) with ear stud and (b) without ear stud
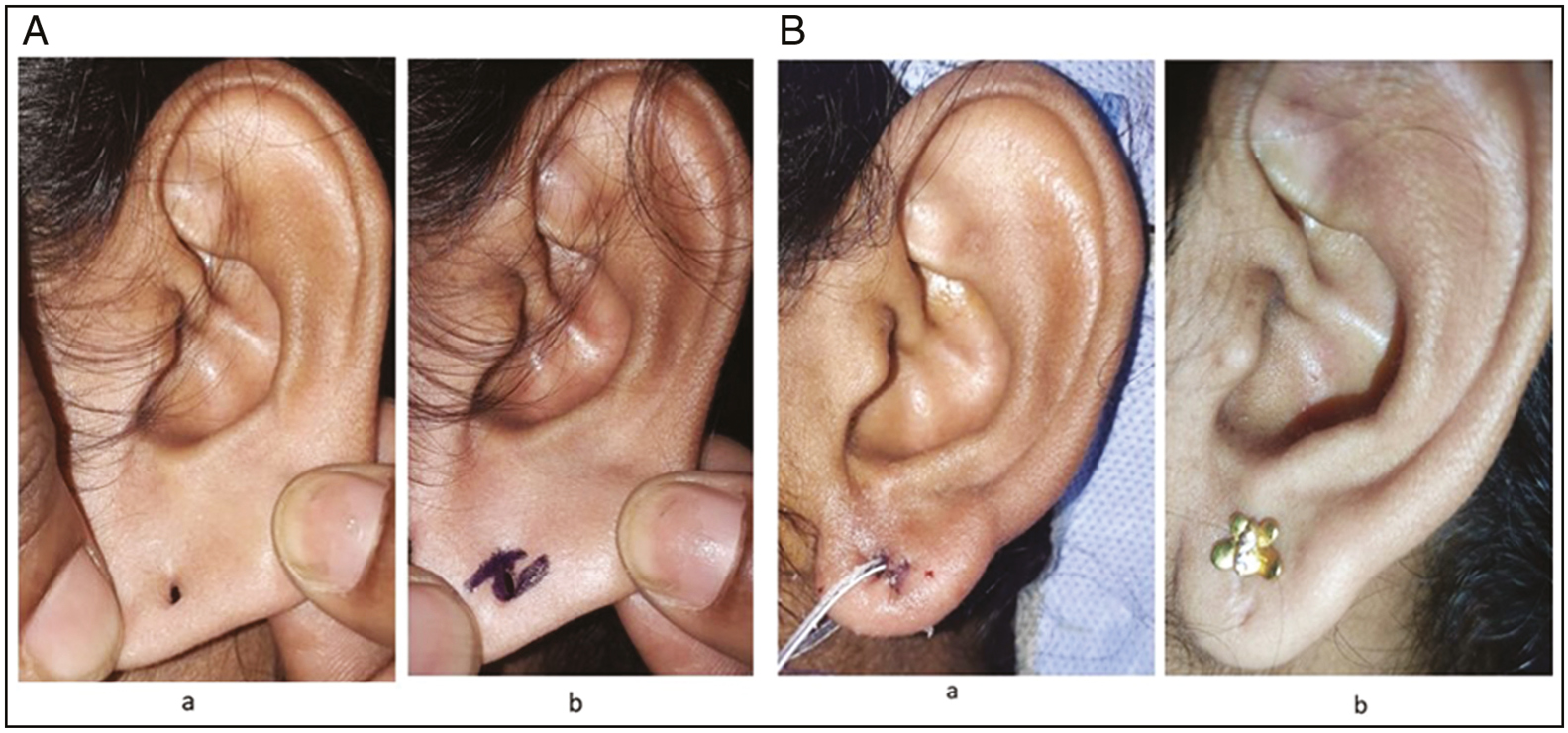
- (A) Representative case 2: (a) large ear hole and (b) flap markings. (B) Postoperative results: (a) immediate postoperative picture and (b) late postoperative picture with stud
All the cases were done as day case surgeries by the same surgeon. They were given oral antibiotics for three days and topical antibiotics for seven days. Sutures were removed on the seventh postoperative day. The spacers that were placed in the ear hole were retained for three weeks. At three weeks, the spacers were replaced with small gold studs. We insisted on gold studs in order to avoid any chance of metal allergy and consequent recurrent split earlobe.[12] All patients were advised not to change the studs for three months so as to avoid any trauma and to ensure proper healing of the flaps. Follow up was done at six months for the reassessment of size of the ear hole, final shape and contour of the ear lobe and evaluation of patient satisfaction with Global Aesthetic Improvement Scale (GAIS), patient satisfaction in Likert scale and photographs.
RESULTS
A total of six patients (12 ear lobes) with Type I ear holes were operated with the hole-retaining lobeplasty technique. All the patients were females and all had bilateral wide ear holes. The age range was 22 years to 56 years (mean age 45.6yr +/- 16yrs)
None of the patients had complications like infection, bleeding, flap necrosis or flap dehiscence in the immediate post-operative period. At three weeks, the spacers were removed. All the holes were found patent and we could easily put the gold ear studs. At six months follow up, it was found that all patients had centrally placed, circular shaped ear holes, with well settled support flap and rounded aesthetically good contour. All the patients were satisfied with their newly created ear hole and lobe contour, with an average Patient Satisfaction Score of 4.8+/-0.4None of the patients operated by the technique developed any recurrence or ear lobe elongation at the end of follow-up. Outcome was assessed by surgeon using the Global Aesthetic Improvement Scale(GAIS) and the average GAIS score was 4.83 +/- 0.38. The average patient satisfaction scores in Likert scale showed satisfactory results as shown in [Table 1 and Figures 5 and 6]. All the patients were satisfied with their newly created ear hole and the shape of the ear lobe with an average Patient Satisfaction Score of 4.8+/-0.4.
| Age | Number | Side | Type of large ear hole | Ear lobe contour | Ear hole shape, size | Lobe notching | GAIS | Patient satisfaction |
|---|---|---|---|---|---|---|---|---|
| 56 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 5 | Very much satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 5 | |||
| 54 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 5 | Very much satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 5 | |||
| 22 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 4 | Satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 4 | |||
| 59 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 5 | Very much satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 5 | |||
| 55 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 5 | Very much satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 5 | |||
| 28 years | Bilateral | Right | Type 1 | Rounded | Maintained | Absent | 5 | Very much satisfied |
| Left | Type 1 | Rounded | Maintained | Absent | 5 |
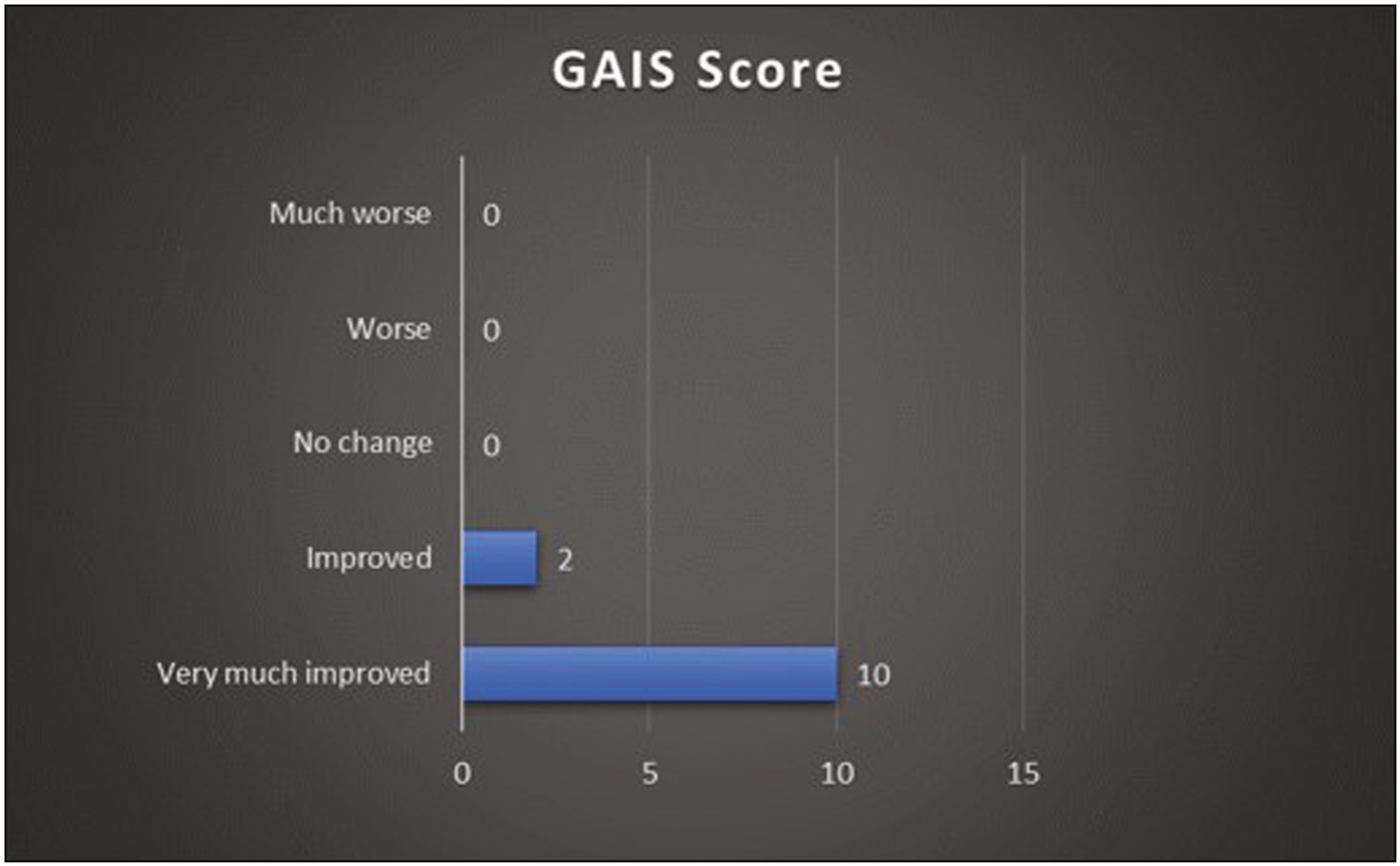
- Bar diagram showing Global Aesthetic Improvement Scale (GAIS) scores

- Bar diagram showing the patient satisfaction scores
DISCUSSION
Ear piercing is a universal trend, associated with various societal and cultural customs. The ear lobe is the most commonly pierced part of the ear as it is made of fibrofatty tissue and thus easy to pierce.[13]One of the major complications of ear piercing is the widening and subsequent tear of the ear. Torn ear lobes can be classified as complete, partial, unilateral or bilateral.[2]
There are many classifications described for the ear lobe deformities in literature. Boo- Chai classified ear lobe deformities into Complete and incomplete clefts.[7] Acquired ear lobe deformities are classified as per the Blanco-Davila and Vasconez classification[6] into:
Type I- where the boundaries of the ear hole is less than half the distance between the original piercing and inferior margin of the earlobe.
Type II- the boundaries of the ear hole extend to more than half the distance between the original piercing and inferior margin of the earlobe
Type III- Cleft hole completely splits the earlobe.
Another classification was proposed by Agarwal and Chandra in 2008, as Type I to V[5]
Type I- stretched out ear hole more than twice the original diameter
Type II-Near total split leaving a thin rim of lobe remaining
Type III-completely split ear lobe
Type IV-total split of ear lobes with fibrosis and retraction of margins
Type V-single/multiple tears on the earlobe with fibrosis and scarring.
Type I and II partial earlobe tears present with a unique problem of being unable to wear small to moderate sized ear studs but being able to wear ear-hangings. This forces the individual to persistently wear pendulous ear-hangings thus eventually progressing to a type III partial cleft.
There have been many techniques proposed for the repair of torn ear lobes such as the Straight line closure with or without hole preservation, hole preserving flap repair with and without inferior margin Z-plasty, etc.[14] Hole retaining techniques incorporating Z-plasties were described for large ear holes like Abenovali’s half Z-plasty and hammock flap technique by Dr. K.Gajiwalla, which are suitable mainly for Type II and III ear lobes deformities.
In his technique of half Z-plasty repair of incompletely cleft ear lobe, Dr. Abenavoli incorporated Z-plasty in the incomplete cleft after leaving a part of the superior part of the hole intact above the Z-plasty.[9] He freshened the margins of the triangular flaps and transposed them. He retained the hole on the superior part. He sutured the transposed the triangular flaps and sutured the rest of the hole below the Z-plasty primarily after freshening. This technique caused lengthening the ear lobe resulting in a pointed rather than rounded shape.[10] There was also an increased risk of an oblique tear that was seen in 2 out of 37 cases operated by him.[10] This technique is also best suited for Type II and III clefts and difficult to be performed in Type I ear lobe clefts.
In the hammock plasty technique, Dr. K. Gajiwala[10] used a true half Z-plasty technique where a triangular flap was raised on one margin of the ear hole and inset on a horizontal or upward slant back cut on the opposing margin to recreate the new hole. The triangular flap that he transposed into the back cut was named as the hammock flap[10] Although the technique provides a strong flap of the inferior part of the ear hole, the primary closure that is done below the hammock flap may result in scar contracture and notching of the ear lobe in the future. The Hammock technique gave rise to horizontally oriented ear holes making them aesthetically displeasing. The hammock flap technique also is suitable in Type II and Type III ear holes.
Our technique of hole retaining lobeplasty is suitable for Type I ear holes, where the boundaries of the ear hole is less than half the distance between the original piercing and inferior margin of the earlobe making it unsuitable for wearing studs. The technique is advantageous that it is a simple, single staged procedure that can be easily mastered and performed as a day-case procedure. In addition, we obtained a strengthened, rounded and well supported inferior margin and a rounded ear hole. Also, there was no incidence of inferior margin notching or recurrence of tear as seen with the other techniques such as straight line closure or simple hole preserving lobeplasties.
In our technique, the superiorly based triangular flap is solely used for the creation of a rounded ear hole. The inferiorly based flap provided adequate tissue support to the new hole. The technique also created a rounded ear hole and absence of the linear scar under the ear hole reduces the chance of future scar dehiscence and lobe notching due to linear scar contracture.
Advantages of hole-retaining lobeplasty
The ear hole is retained. This avoids the requirement of future re-piercing. Thus, this is a single stage procedure.
The shape of the earlobe is improved. The conically shaped ear lobe is made round thereby making it more aesthetically pleasing.
The inferiorly based flap act as support flap for the new ear hole thereby preventing future elongation.
It is a simple procedure that can be easily mastered
There are certain points to be kept in mind to avoid complications. Proper planning is necessary before execution of the procedure. If de-epithelisation is done on the superiorly based flap, then the hole will be pushed down making the new hole very unattractive. Second precaution is that the vascularity of the tip of the flaps might be compromised if an acute angle flap less than 300 is planned as in any Z plasty technique.
Limitation
The limitations of this study include the small sample size and lack of long term follow up. The study needs to be conducted as a prospective, randomized, multi-institutional study with a large sample size over a long period of study for more accurate and valid results.
CONCLUSION
Hole- retaining lobeplasty is a simple, cost effective, single staged, day case procedure for repair of Type I large ear holes,that can be easily duplicated by young plastic surgeons. The newly created hole is aesthetically better, in that it is circular and centrally placed with a more rounded ear lobe. The absence of the weak scar tissue and tissue break down and a support flap below the ear hole prevents the future recurrence and complication.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors would like to thank my colleagues in Plastic Surgery Department for the support.
References
- A comparative study of elongation of earlobe following two different modalities for repair of posttraumatic split of earlobe: Simple side-to-side closure and closure with anterior posterior flap modification. J Cutan Aesthet Surg. 2020;13:5-10.
- [Google Scholar]
- A revised classification and treatment algorithm for acquired split earlobe, with a description of the composite technique and its outcome. Cureus. 2020;12:e10422.
- [Google Scholar]
- Repair of a split or deformed ear lobe with a tongue depressor blade for stabilization during surgery. Innovative Techniques in Skin Surgery 2002:531-4.
- [Google Scholar]
- A new technique for repair of acquired split-ear-lobe deformity: The free conchal cartilage sandwich graft. J Plast Reconstr Aesthet Surg. 2010;63:499-505.
- [Google Scholar]
- The cleft earlobe: A review of methods of treatment. Ann Plast Surg. 1994;33:677-80.
- [Google Scholar]
- Repair of torn earlobe with preservation of the perforation for an earring. Plast Reconstr Surg. 1973;51: 472-3.
- [Google Scholar]
- Split earlobe: Repair using a half Z-plasty technique. Plast Reconstr Surg. 1996;98:372-3.
- [Google Scholar]
- Repair of the split earlobe using a half Z-plasty. Plast Reconstr Surg. 1998;101:855-6.
- [Google Scholar]
- Vertical lifting: A new optimal thread lifting technique for asians. Dermatol Surg. 2017;43:1263-70.
- [Google Scholar]
- Increase Lobuloplasty in the treatment of deformities secondary to the use of stretched piercing.earlobe. Clin Surg. 2020;4:1-4.
- [Google Scholar]




