
Translate this page into:
Treatment of Fordyce Spots with CO2 Laser: A Case Series of Three Patients
Address for correspondence: Dr. Yogesh Bhingradia, Department of Dermatology, Shivani Skin Care and Cosmetic Clinic, Sarthi Doctor house, Fourth floor, Hirabaug, Varachha road, Surat, Gujrat, India. E-mail: yogeshbhingradia@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
The Fordyce spots are ectopic sebaceous glands, located at the lip’s vermilion border or the oral mucosa. Clinically presents as tiny, discrete, white or yellowish, focally grouped papules. It is a common cosmetic disorder and is significantly associated with emotional stress. Herein, we describe three cases that showed satisfactory cosmetic results after the treatment of Fordyce spots using a CO2 laser. Patients were 21-year-old, 25-year-old, and 28-year-old males with Fordyce spots on the upper lip. They were treated with the CO2 laser and after 4 months of treatment, no recurrence was noted. Treatment with pinhole ablation with CO2 laser improves cosmetic results, reduces downtime, and minimizes side effects. To the best of our knowledge, no such case series have been reported to date from the Indian subcontinent.
Keywords
CO2 laser
Fordyce spots
pinhole ablation
The pinhole technique is a conservative approach that helps us to achieve precise dermal ablation, with better cosmetic results, and minimize complications

INTRODUCTION
Fordyce spots are enlarged heterotopic sebaceous glands that can occur on various body parts such as the lips, oral mucosa, retromolar area, penis, and labia. Even though the sebaceous glands are present since birth, this condition is common after puberty. The development of Fordyce spots during this period is in response to the gonadal and adrenal androgenic hormones.[1] In literature, treatment for this disorder has not been published, mainly because it is not considered a pathologic condition. This fact motivated us to report the cases of three male patients with Fordyce spots who were successfully treated with CO2 laser.
CASE SERIES
Case 1
A 21-year-old male patient with multiple, yellowish papules on the upper lip for 2 years is reported [Figure 1A]. The diagnosis was confirmed with a small 2.5 mm skin punch biopsy. On histopathological examination, it shows mild spongiosis attached to the epithelium, and opening onto the surface are several well-developed lobulated sebaceous glands, some of which are connected to the surface by ducts. The submucosa shows a moderately dense lymphoplasmacytic infiltrate [Figure 1B]. We took written informed consent from the patient and later he underwent a CO2 laser session. Before the laser session, we applied topical anesthetic cream for 45 min over the area to be treated. The machine used was a 30W CO2 laser, which was used in continuous mode at a power of 3W. After complete ablation of the lesion crust was left behind which falls off on its own. The patient was advised to apply mupirocin ointment twice a day to the treated area for 2 weeks postprocedure. The patient was evaluated after 2 weeks of treatment, getting re-epithelization and crusting over the lip [Figure 1C]. After 16 weeks, there was significant cosmetic improvement without any recurrences in the treated area [Figure 1D].
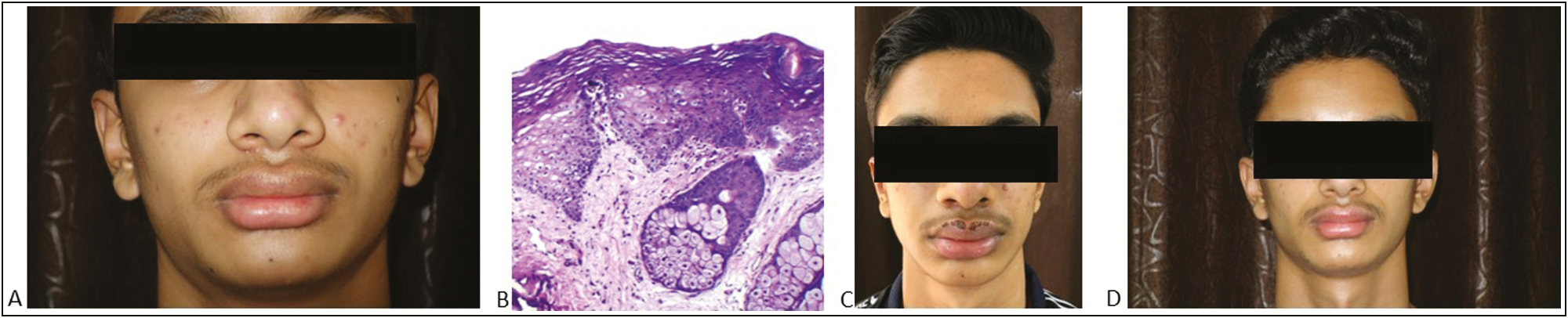
- (A) Multiple, well-defined, yellowish papules over the upper lip, (B) (H&E, 40× magnification) it shows mild spongiosis attached to the epithelium, and opening onto the surface is a well-developed lobulated sebaceous gland. The submucosa shows a moderately dense lymphoplasmacytic infiltrate. (C) (Postprocedure after 2 weeks): crusting present over the upper lip, (D) resolution of lesions postprocedure after 16 weeks of treatment
Case 2
A 25-year-old male patient with multiple yellowish papules coalescing to form plaques on the upper lip since puberty is reported [Figure 2A]. We confirmed our diagnosis with a small 2.5 mm skin punch biopsy. The histopathological examination was co-relating with ectopic sebaceous glands [Figure 2B]. After obtaining informed consent, we performed a CO2 laser treatment. Before the laser session, we applied topical anesthetic cream for 45 min over the area to be treated. We used a super pulsed CO2 laser in continuous mode for this patient because the lesion was widespread with few plaques present over the upper lip. In plaque-type lesions, multiple holes were made at an interval of 1–2 mm. Power of 3W, and two passes removed necrotic tissue with a gauze soaked in physiologic solution between passes. The patient was advised to apply mupirocin ointment twice a day to the treated area for 2 weeks postprocedure. The patient was evaluated after 2 weeks of treatment, getting crusting over the lip. After 16 weeks, there were no recurrences in the treated area with a good cosmetic result [Figure 2C].
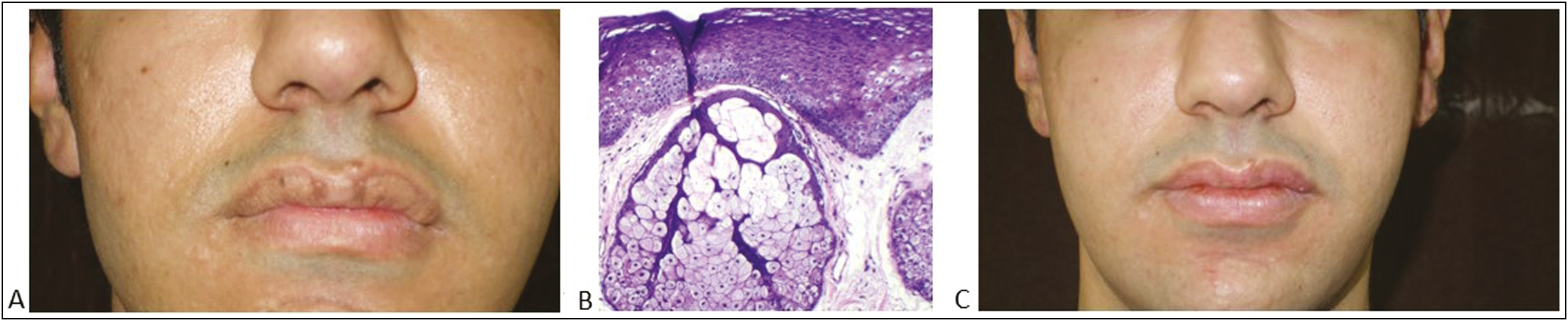
- (A) Multiple, well-defined whitish to yellowish papules coalescing to form plaques on the upper lip, (B) (H&E, 40× magnification) it shows mild spongiosis and well-developed lobulated sebaceous gland suggestive of Fordyce spots, (C) resolution of lesions postprocedure after 16 weeks of treatment
Case 3
A 28-year-old male patient with multiple, yellowish papules on the upper lip for 5 years is reported [Figure 3A]. The diagnosis of Fordyce spots was made clinically. After the patient understood the benign nature of this disorder, he insisted on receiving treatment for cosmetic reasons. Therefore, after obtaining written informed consent, we performed a pinhole ablation using a CO2 laser. The CO2 laser was used in continuous mode at a power of 3W under topical anesthesia. A single hole was made over each of the papular lesions by directing the laser beam perpendicular to the top of the lesions for 2–3 s. This leads to the formation of necrotic columns and thus reducing the bulk of the pathological tissue [Figure 3B and C]. The patient was advised to apply mupirocin ointment twice a day. The patient was evaluated after 2 weeks of treatment, getting an excellent re-epithelization and crusting over the lip. The pinhole ablation technique helps us in the conservation of uninvolved tissue and minimizes downtime and complication. After 6 weeks, there was a complete resolution of the lesion and no recurrence in the treated area [Figure 3D]. The patient is under the follow-up period.
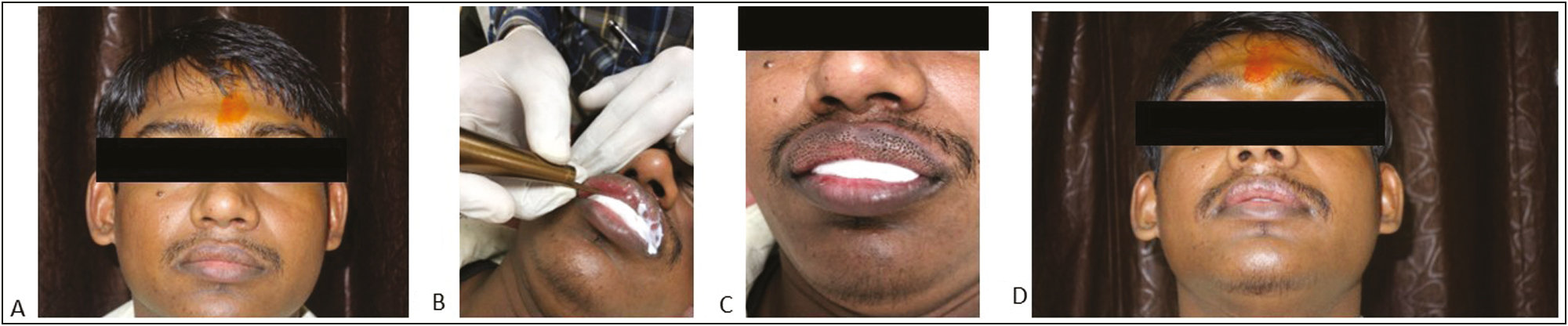
- (A) Multiple, discrete, yellowish papules over the upper lip, (B) Pinhole ablation technique using CO2 laser, (C) immediate postoperative photograph after pinhole ablation, (D) resolution of lesions postprocedure after 6 weeks of treatment
DISCUSSION
In 1896, Fordyce described the occurrence of whitish to yellowish spots on the oral mucosa and vermilion border of lips. The incidence of Fordyce spots, increases with age, being more common after puberty. The prevalence of Fordyce spots in adults is 70–80%. The male-to-female predilection is 2:1.[2] Fordyce spots are discussed only briefly in dermatologic literature, as they are considered a normal variation, not taking into consideration the patient’s need for cosmetic improvement. The various treatment options include micro-punch surgery, electrodesiccation, cryotherapy, ablative laser, photodynamic therapy, topical dichloroacetic acid, topical tretinoin, and oral isotretinoin.[3-5]
Deep ablation with CO2 laser has traditionally been utilized for various conditions. However, it causes excessive thermal injury, which also increases the risk of side effects, especially in Fitzpatrick skin types four and five.[6] To overcome this drawback, the fractional mode in CO2 lasers has been used. Fractional mode is only able to cover 10–30% of the treatment area and can penetrate only up to 1.5 mm depth, necessitating repeat sessions.[78] In continuous mode, a CO2 laser can be used to deliver columns of energy up to the dermal tissue.[9] The super pulsed mode allows high energy peaks, limiting in this way the thermal damage to the cutting area. The pinhole method is making deep, closely set tiny holes reaching down at the upper dermis using a CO2 laser. We choose the method based on our therapeutic experience with CO2 laser and the extent of the lesion.
The Pinhole technique refers to the creation of multiple holes at regular intervals using a CO2 laser. This leads to a precise dermal injury which reduces pathological tissue while stimulating uniform collagen and elastin deposition, thus improving the cosmetic appearance.[10] Our findings allow us to suggest that the pinhole technique using CO2 laser treatment is safe and effective in patients with Fordyce spots. It can be considered an ideal therapeutic tool for this entity. It also reduces the healing time and complications when compared to complete ablation.
In conclusion, we have had positive outcomes with the use of CO2 laser ablation for patients with Fordyce spots. It helps us to acquire better cosmetic results. We also believe that there is a lot of scope for this treatment modality, which needs to be explored further in the future.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Dichotomous long-term response to isotretinoin in two patients with Fordyce spots. Pediatr Dermatol. 2014;31:73-5.
- [Google Scholar]
- Fordyce spots of the lip responding to electrodesiccation and curettage. Dermatol Surg. 2008;34:960-2.
- [Google Scholar]
- Micro-punch technique for treatment of Fordyce spots: a surgical approach for an unpleasant condition of the male genital. J Plast Reconstr Aesthet Surg. 2013;66:e8-11.
- [Google Scholar]
- Pinhole carbon dioxide laser treatment of secondary anetoderma associated with juvenile xanthogranuloma. Dermatol Surg. 2012;38:1741-3.
- [Google Scholar]
- Treatment of periorbital syringoma by the pinhole method using a carbon dioxide laser in 29 Asian patients. J Cosmet Laser Ther. 2015;17:273-6.
- [Google Scholar]
- Treatment of syringoma using an ablative 10,600-nm carbon dioxide fractional laser: a prospective analysis of 35 patients. Dermatol Surg. 2011;37:433-8.
- [Google Scholar]
- The treatment of burn scar-induced contracture with the pinhole method and collagen induction therapy: a case report. J Eur Acad Dermatol Venereol. 2008;22:513-4.
- [Google Scholar]
- Burn scars treated by pinhole method using a carbon dioxide laser. J Dermatol. 2006;33:869-72.
- [Google Scholar]




