
Translate this page into:
Modified platelet rich plasma therapy for alopecia totalis
Address for correspondence: Dr. Manmohan Bagri, Department of Dermatology, Venereology and Leprology, All India Institute of Medical Sciences; Rishikesh, Uttarakhand-249203, India. E-mail: drmanni99@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Alopecia areata (AA) is an autoimmune disease characterized most commonly by patchy nonscarring hair loss which may progress to alopecia totalis which has poor prognosis. Platelet-rich plasma (PRP) therapy along with intralesional triamcinolone acetonide that is modified PRP proved to be beneficial in the case of alopecia totalis and helps in weaning patient off oral immunosuppression.
Keywords
Alopecia
modified
platelet-rich plasma
totalis

INTRODUCTION
Alopecia areata (AA) is an autoimmune disease most commonly characterized by patchy nonscarring hair loss, which may sometimes progress to involve the entire scalp (alopecia totalis) and body hair (alopecia universalis), while few patients may show spontaneous remission. AA has limited treatment modalities, none of which has proven to be curative.[1] Platelet-rich-plasma (PRP) is thought to enhance hair growth by stimulating growth factors such as vascular endothelial growth factor, platelet-derived growth factor, and transforming growth factor, which further promotes the cellular proliferation and angiogenesis around the dermal papilla, enhancing blood circulation around hair follicles and also prolong anagen phase through the increase in expression of fibroblast growth factor -7, while low soluble steroids like triamcinolone acetone (TrA) have anti-inflammatory and immunosuppressive role by suppressing T cell-mediated immune attack.[2] We herein, present a case of alopecia totalis treated with modified PRP that is PRP in conjunction with intralesional TrA.
Case Report
A female in her late twenties presented with hair loss in the entire scalp for 6 months which started initially as patchy loss of hair over the crown and later progressed to involve whole scalp in 2 months [Figure 1A]. There was no significant past medical and family history. Baseline investigations such as CBC, LFT, KFT, sugar (random), HIV, HbsAg, HCV and thyroid profile were within normal range. She was started on tablet prednisolone 40 mg on two consecutive days in pulse form twice weekly, azathioprine 50 mg daily along with topical 5% minoxidil, which showed improvement within 2 months and the same treatment was maintained for next three months, then on tapering oral steroid, she lost her new hair growth which than progressed again to involve entire scalp in a span of 1 month so we planned to give her modified PRP injections along with the continuation of previous therapies. PRP was prepared by the double spin method, 10 ml of the patient’s whole blood was collected in each acid citrate dextrose containing vacutainers and centrifuge at 3500 RPM for 10 min. The plasma collected was then further centrifuged for 8 min with 2100 RPM speed. Supernatant clear plasma that is platelet-poor plasma was discarded. 3.5 ml of PRP was collected in insulin syringes with 40 units markings, up to the mark of 35 units, and then the remaining 5 units were filled with TrA in 10 mg/ml concentration Topical anaesthetic cream containing lidocaine and prilocaine was applied for 45 min, injections were given intradermally 0.1 ml over the entire scalp 1 cm apart. Four weeks after the first session new hair started to grow [Figure 1B]. Four such sessions were repeated at 4 weeks intervals along with which oral steroids were tapered off. She showed marked improvement with thick hair and an increase in density [Figure 1C] in comparison to previous treatment without modified PRP, and she was maintained on topical 5% minoxidil and tablet azathioprine 50 mg once daily which was planned to taper off in the next 3 months with regular follow up.
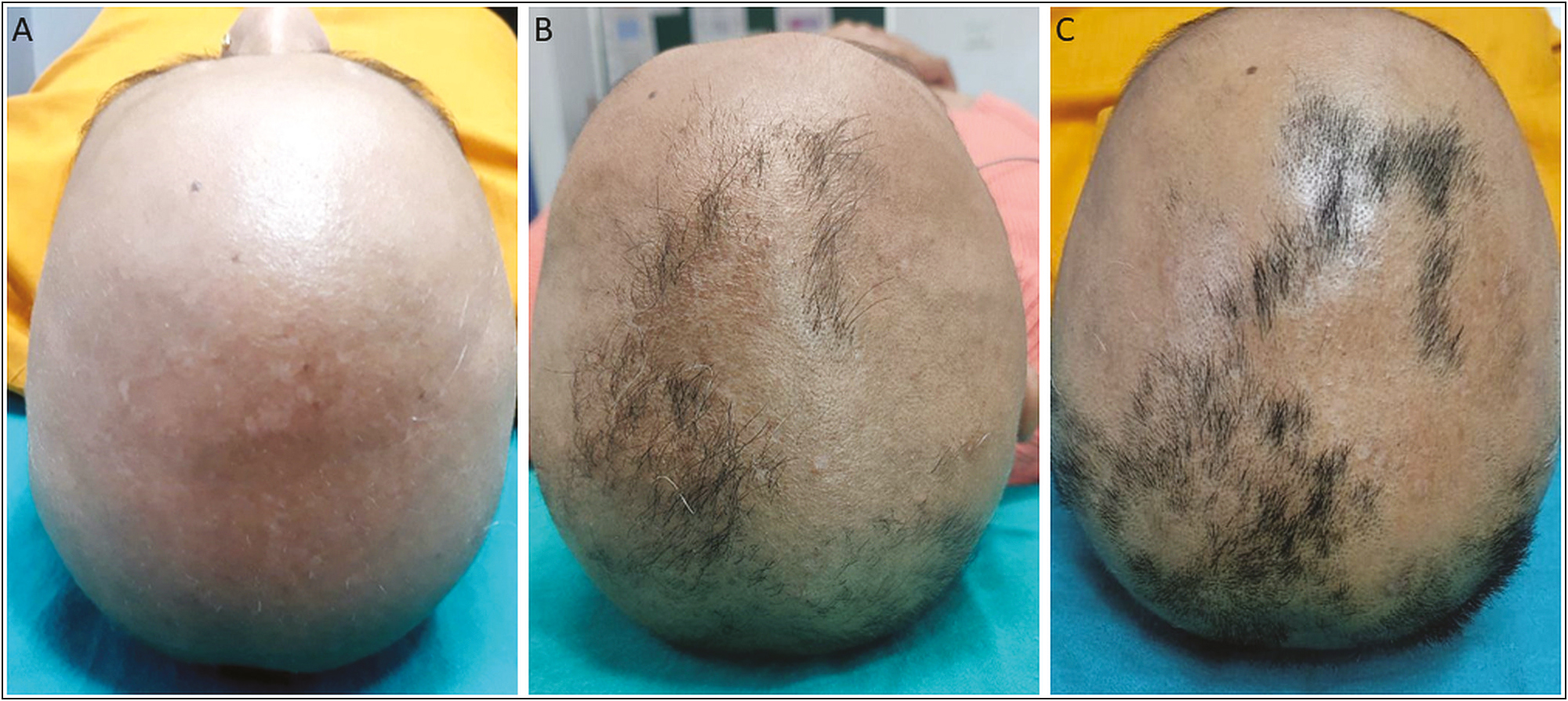
- A: Total hair loss over scalp. B: Hair growth after first session of modified PRP. C: Hair growth after fourth session of modified PRP
DISCUSSION
Alopecia areata is an autoimmune disorder that causes non-scarring hair loss in form of a patchy loss of hair. Alopecia can be categorized based on the extent of involvement as Alopecia areata means partial hair loss, totalis means complete scalp hair loss, Universalis means with 100% scalp and body hair loss, diffuse alopecia areata is a sudden thinning of hair rather than lost patches, ophiasis alopecia areata causes hair loss in a band shape around the sides and back of the head.[3] The first line of treatment for AA is intralesional corticosteroids such as TrA in the dosage of 5–10 mg/ml over the scalp and 2.5–5 mg/ml over the beard and eyebrow areas repeated every 4–6 weeks until favourable hair growth is seen.[4] Preparations used include triamcinolone acetonide, triamcinolone hexacetonide, and hydrocortisone acetate. Triamcinolone acetonide is the preferred intralesional product because it is less atrophogenic than triamcinolone hexacetonide. Few studies showed that both PRP and TrA significantly increased the levels of Ki67 in AA patches compared to placebo.[5] and prevent relapse of the conditions whereas in AA cases treated with TrA relapse rates were 29% in limited AA and 72% in alopecia totalis during a 3-month follow-up period.[67]
Alopecia totalis and alopecia universalis are indicators of poor prognosis. Conventional treatment modalities such as oral/topical/intralesional/intravenous pulse corticosteroid therapy or topical/oral immunomodulators such as azathioprine, cyclosporine, tacrolimus, and psoralen + UVA have failed to show remarkable improvement in severe forms of AA.[8,9,10]
This case showed that PRP in combination with TrA may be effective treatment option in alopecia totalis as it prevents side effects related to prolonged systemic immunosuppression as we are able to taper corticosteroids under its cover and maintaining hair growth. However, studies with larger population and long follow up are needed to prove its benefits.
CONCLUSION
Modified PRP with TrA was successively used for the treatment of Alopecia totalis, which helps in early regrowth and maintenance of hair over the scalp, thus reducing the prolonged consumption of immunosuppressants.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Author contributions
Dr(s) Manmohan Bagri and Avita Dhiman had full access to all of the data in the study and take responsibility for the integrity and accuracy of the data.
Study concept and design:Bagri M,
Acquisition, analysis, and interpretation of data: Dhiman A
Drafting of the manuscript: Dhiman A
Critical revision of the manuscript for important intellectual content: Bagri M
Acknowledgement
None.
REFERENCES
- Alopecia totalis successfully treated with modified platelet-rich plasma therapy in a patient recalcitrant to traditional treatment modalities. Clin Dermatol Rev. 2021;5:120.
- [Google Scholar]
- Principles and methods of preparation of platelet-rich plasma: A review and author’s perspective. Journal of Cutaneous and Aesthetic Surgery. 2014;7:189-97.
- [CrossRef] [Google Scholar]
- Progress in the use of platelet-rich plasma in aesthetic and medical dermatology. The Journal of Clinical and Aesthetic Dermatology. 2020;13:28-35.
- [Google Scholar]
- Role of platelet-rich plasma in chronic alopecia areata: Our centre experience. Indian J Plast Surg. 2015;48:57-9.
- [Google Scholar]
- The effect of platelet-rich plasma in hair regrowth: A randomized placebo-controlled trial. Stem Cells Translational Medicine. 2015;4:1317-23.
- [CrossRef] [Google Scholar]
- Local injection of steroids and hair regrowth in alopecias. Arch Dermatol. 1960;82:894-902.
- [Google Scholar]
- Placebo-controlled oral pulse prednisolone therapy in alopecia areata. J Am Acad Dermatol. 2005;52:287-90.
- [Google Scholar]
- [Intravenous pulse methylprednisolone therapy for severe alopecia areata: An open study of 66 patients] Ann Dermatol Venereol. 2003;130:326-30.
- [Google Scholar]




