
Translate this page into:
Mohs surgery for squamoid eccrine ductal carcinoma
Address for correspondence: Dr. Maryam Eghtedari, Central Clinical School, University of Sydney, The Skin Hospital, Darlinghurst, New South Wales, Australia. E-mail: maryam.eghtedari@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Squamous eccrine ductal carcinoma is a rare cutaneous malignancy. It has the potential to locally recur and may occasionally metastasize. It presents a diagnostic challenge given its rare nature and overlapping histopathological features with other cutaneous carcinomas.
Keywords
Eccrine carcinoma
eccrine ductal carcinoma
mohs micrographic surgery
squamous cell carcinoma
An 82-year-old woman presented with a right cheek squamoid eccrine ductal carcinoma and was treated with Mohs surgery. Squamoid eccrine ductal carcinoma is a rare malignancy with potential for metastasis. It is a diagnostic challenge as it has overlapping histopathological features with squamous cell carcinoma and other eccrine malignancies.

INTRODUCTION
It is estimated that eccrine carcinomas compromise 0.01% of cutaneous malignancies. Squamoid eccrine ductal carcinoma is a rare subtype of ductal eccrine carcinoma.[12] These tumors tend to present as pink to flesh colored nodules or plaques on the head and neck of the elderly.[3]
Histologically, squamoid eccrine ductal carcinoma is characterized by squamous metaplasia, and may be misdiagnosed as squamous cell carcinoma (SCC) on the initial biopsy.[23]
Case History
An 82-year-old woman presented with a two-year history of a growing indurated plaque on her right cheek [Figure 1]. There was no lymphadenopathy. She was otherwise in excellent health and had no history of skin cancer nor immunosuppression. Diagnostic partial biopsy revealed keratinocyte basal atypia enclosing isolated small ductular structures in a desmoplastic stroma. The biopsy features were suggestive of a squamoid eccrine ductal carcinoma [Figure 2]. Mohs surgery was performed with curative intent [Figure 1B] and a sharp central debulk was submitted for standard formalin sections, showing residual carcinoma with mixed squamous and eccrine features, consistent with squamoid eccrine ductal carcinoma. The tumor extended to the subcutis. A further circumferential peripheral and deep margin was taken with Mohs surgery and examination of horizontal frozen section margins was clear of residual tumor. A cheek advancement flap was used to reconstruct the defect. The patient had a satisfactory cosmetic result with no recurrence at one year postoperatively.
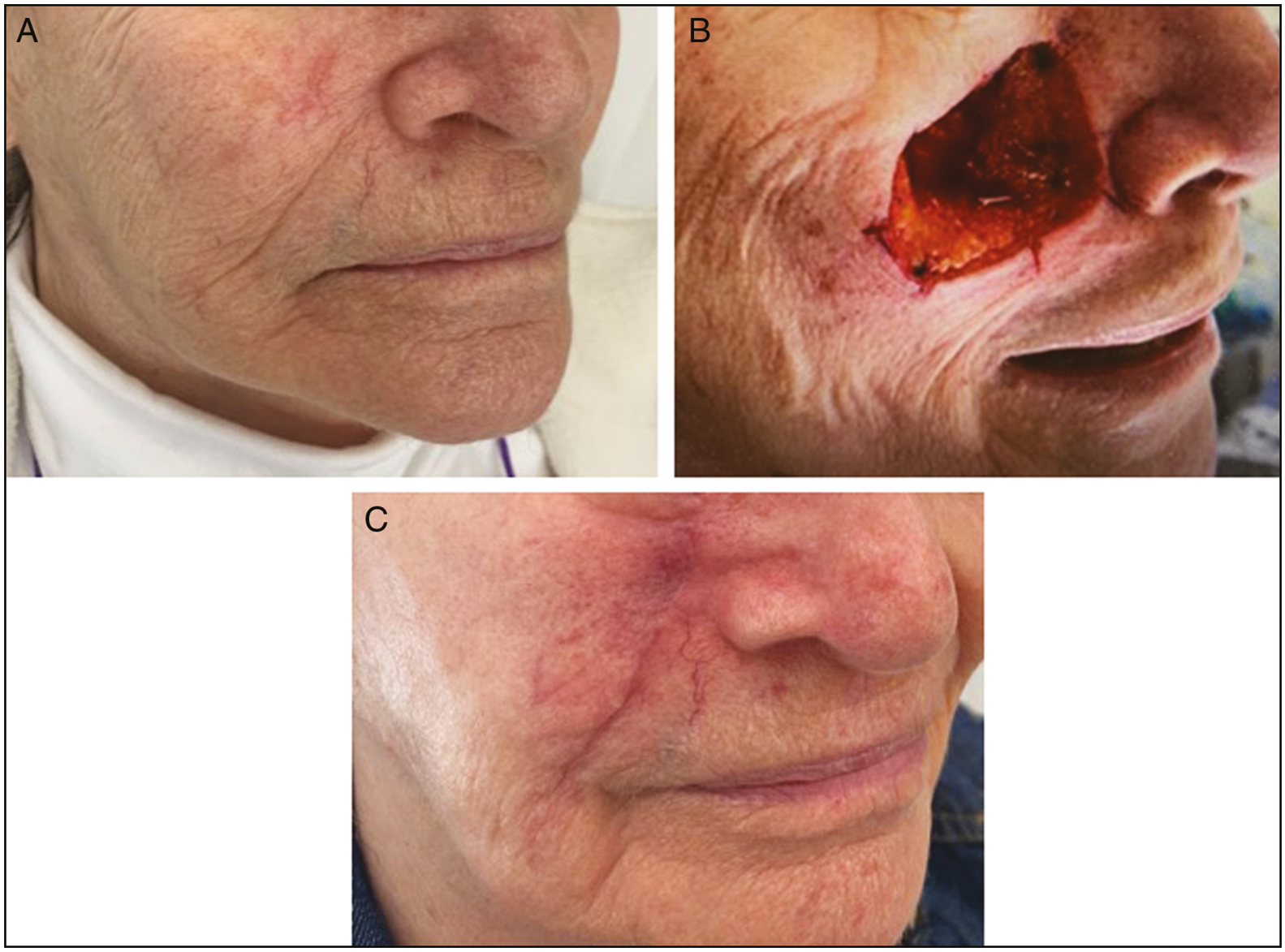
- (A) Female age of 82 years with a right cheek indurated plaque confirmed to be a squamoid eccrine ductal carcinoma. (B) Right cheek defect following Mohs surgery. (C) Right cheek postoperative photo at 1 month
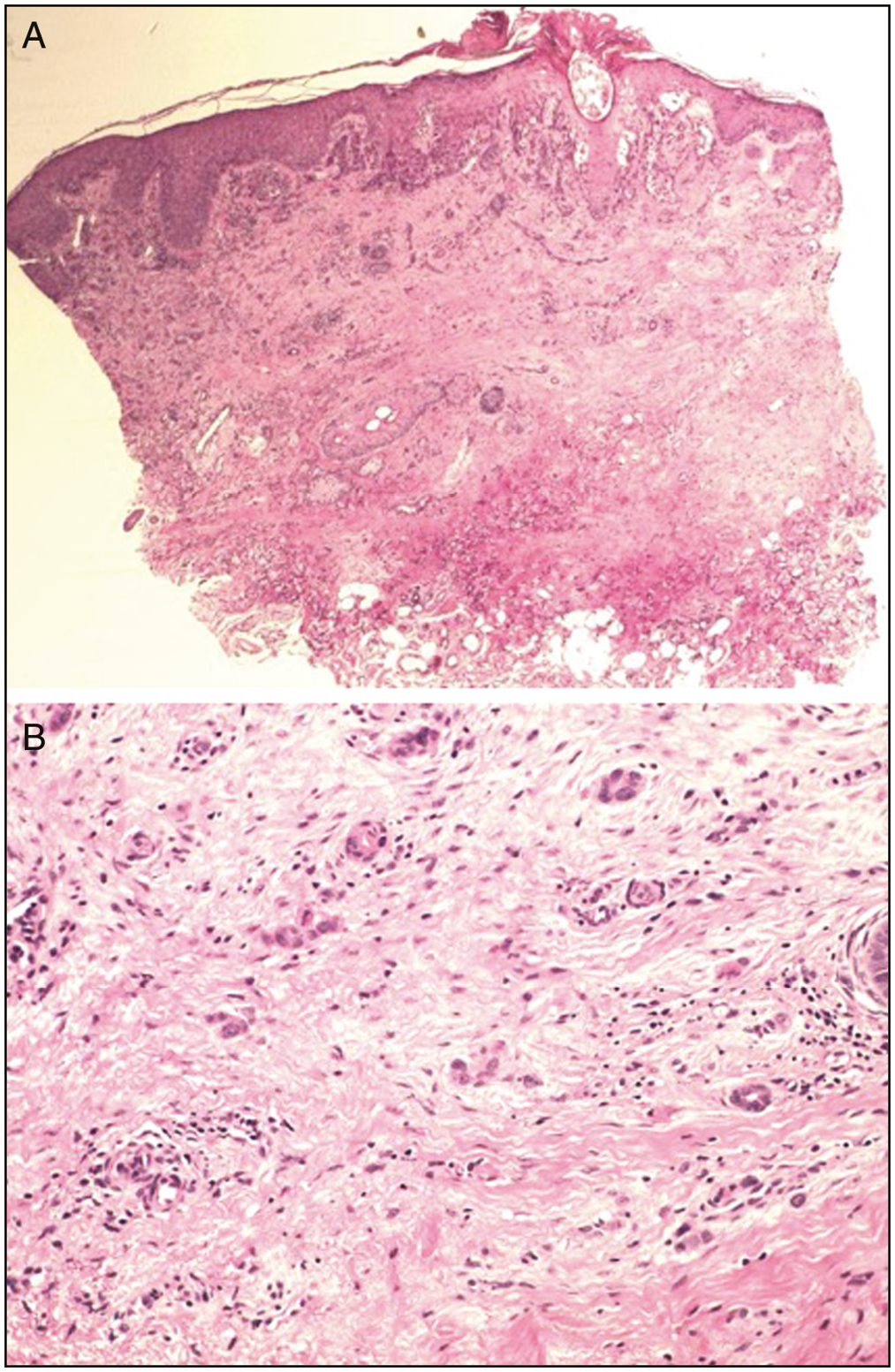
- (A) Low-power view of a squamoid eccrine ductal carcinoma of the right cheek (haematoxylin and eosin stain. (B) High-power view of tumour
DISCUSSION
Squamoid eccrine ductal carcinoma presents a diagnostic challenge because of its rare nature and similar clinical and histopathological features to SCC. However, it is reported that up to 50% of eccrine malignancies metastasize compared to 0.5% of SCCs.[2] Additionally, squamoid eccrine ductal carcinoma can have an aggressive clinical course leading to local perineural invasion, distant nodal metastasis and recurrence.[23]
In contrast to SCC, squamoid eccrine ductal carcinoma has an infiltrative growth pattern and in deeper sections tumor is organized in cords and strands showing duct differentiation in a desmoplastic stroma with median tumor thickness of 4.3 mm. In the presented case, the histology also revealed nests of squamoid cells within deeper eccrine cords and strands, arising from an SCC in situ. Ulceration, necrosis and perivascular and neural infiltrations are other features of SCC. Follow up data has revealed this tumor has the potential for local recurrence in 25% of cases as well as nodal and distant metastasis.[4] No deep local invasion or metastatic disease was present in our case.
At present there is no definitive guidelines regarding treatment of squamoid eccrine ductal carcinoma. Mohs surgery has been proposed for margin control and cure.[56]
For eccrine carcinomas in general, 10–70% rate of recurrence was reported with conventional surgery compared to less than five percent with Mohs surgery.[56]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Squamoid eccrine ductal carcinoma: A case report. The European Research Journal. 2020;6:173-7.
- [Google Scholar]
- Squamoid eccrine ductal carcinoma: A case report and review of the literature. Am J Dermatopathol. 2010;32:287-92.
- [Google Scholar]
- Squamoid eccrine ductal carcinoma. American Journal of Surgical Pathology. 2016;40:755-60.
- [Google Scholar]
- Mohs micrographic surgery for squamoid eccrine ductal carcinoma. Dermatol Surg. 2005;31:1462-4.
- [Google Scholar]




