
Translate this page into:
Successful fat transplant in a rare acquired lipodystrophy Barraquer–Simons syndrome

*Corresponding author: Dr Shreya K. Gowda, Department of Dermatology, All India Institute of Medical Sciences Bhopal, Habibganj, Saketnagar - 462 020, Madhya Pradesh, India. shreyakgowda@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gowda SK, Baheti K, Gupta S, Lakshman AM, Asati D. Successful fat transplant in a rare acquired lipodystrophy Barraquer–Simons syndrome. J Cutan Aesthet Surg. doi: 10.25259/jcas_89_23
Abstract
Lipodystrophies can be generalized and partial/localized lack of subcutaneous tissue, which are uncommon heterogeneous illnesses that can be hereditary or acquired. Acquired partial lipodystrophy’ (APL) is the new name for lipodystrophia progressiva, also known as Barraquer–Simons syndrome (BSS). It could come after a severe viral infection like the measles. Young people and children both experience it. Typically, BSS or APL starts between the ages of 5 and 15. The principal feature of BSS is cephalothoracic lipodystrophy, which affects the face, neck, arms, thorax, and upper abdomen in a cephalocaudal pattern. Alternate complement pathway activation and C3 hypocomplementemia with adipocyte lysis brought on by complement 3 nephritic factor (C3NeF) have been suggested as potential causes of fat loss in individuals with APL, even though the precise process is still mostly understood. Therapeutic options for lipodystrophy include fat fillers. Different types of autologous fat transplants are possible. Autologous free fat graft where a mass of tissue harvested from any discrete subcutaneous location and implanted at a recipient site. Dermofat grafts are made from tissue that has been removed from a region, allowing for the removal of full-thickness skin grafts and the primary closure of defects. The dermofat graft can be employed as a spacer between gliding tissues or as a filler. Omental flaps, which are revascularized fat flaps, can be utilized for microvascular transfer, soft-tissue filler for hemifacial atrophy, or to cover any significant skin defects. When fat is extracted, processed, and transplanted in liquid injectable form for a variety of purposes, it is known as free fat injection.
Keywords
Acquired partial lipodystrophy
Barraquer simons syndrome
autologous fat transplant
autologous free fat graft
cephalothoracic lipodystrophy

INTRODUCTION
Lipodystrophies can be hereditary or acquired loss of subcutaneous tissue either in a generalized or partial/localized manner.1 The acquired partial lipodystrophy (APL) also known as Barraquer– Simons syndrome (BSS) is characterized by a bilateral symmetrical loss of adipose tissue that initially affects the face and later progresses to involve the neck, shoulder, arms, and trunk. The lower extremities are mostly unaffected, with slight female preponderance.2,3
CASE REPORT
A 28-year-old female presented with depressed plaques over bilateral cheeks and arms with no surface cutaneous changes along with hypertrophy of thighs and abdominal region. The patient complained of loss of cheek fat at the onset of puberty followed by her arm fat over the next 3 years. For the past 1 year, the patient had a static course with no fat loss. On examination, loss of buccal fat pads and bilateral arm hypoplasia [Figures 1-3] with normal preservation of subcutaneous fat at the abdominal and thigh region was noticed.

- Bilateral loss of cheek fat pad.

- Disseminated concavities over left arm.

- Irregular contours over right arm.
The patient had a history of normal vaginal delivery with normal developmental milestones with regular attainment of puberty with regular cycles. She was born to a nonconsanguineous healthy parent with no family history . No significant treatment history or drug intake before the onset of the disease. No history of photosensitivity, hair loss, or oral ulcers. No evidence of hepatosplenomegaly, umbilical hernia, acanthosis nigricans, clitoromegaly, hirsutism, or acromegalic features. Ophthalmic and other systemic examinations were unremarkable.
The antinuclear antibody and antinuclear antibody profiles were normal. The patient was denied a biopsy. Magnetic resonance imaging showed loss of cheek fat, arm fat [Figures 4 and 5], and atrophy of muscles of cheeks and arms with preservation of fat and muscle layer of chest, and back. Renal function test, fasting glucose, serum C3 level, and lipid profile were normal. We did surgical correction of facial lipoatrophy, with better aesthetic results over the left cheek.
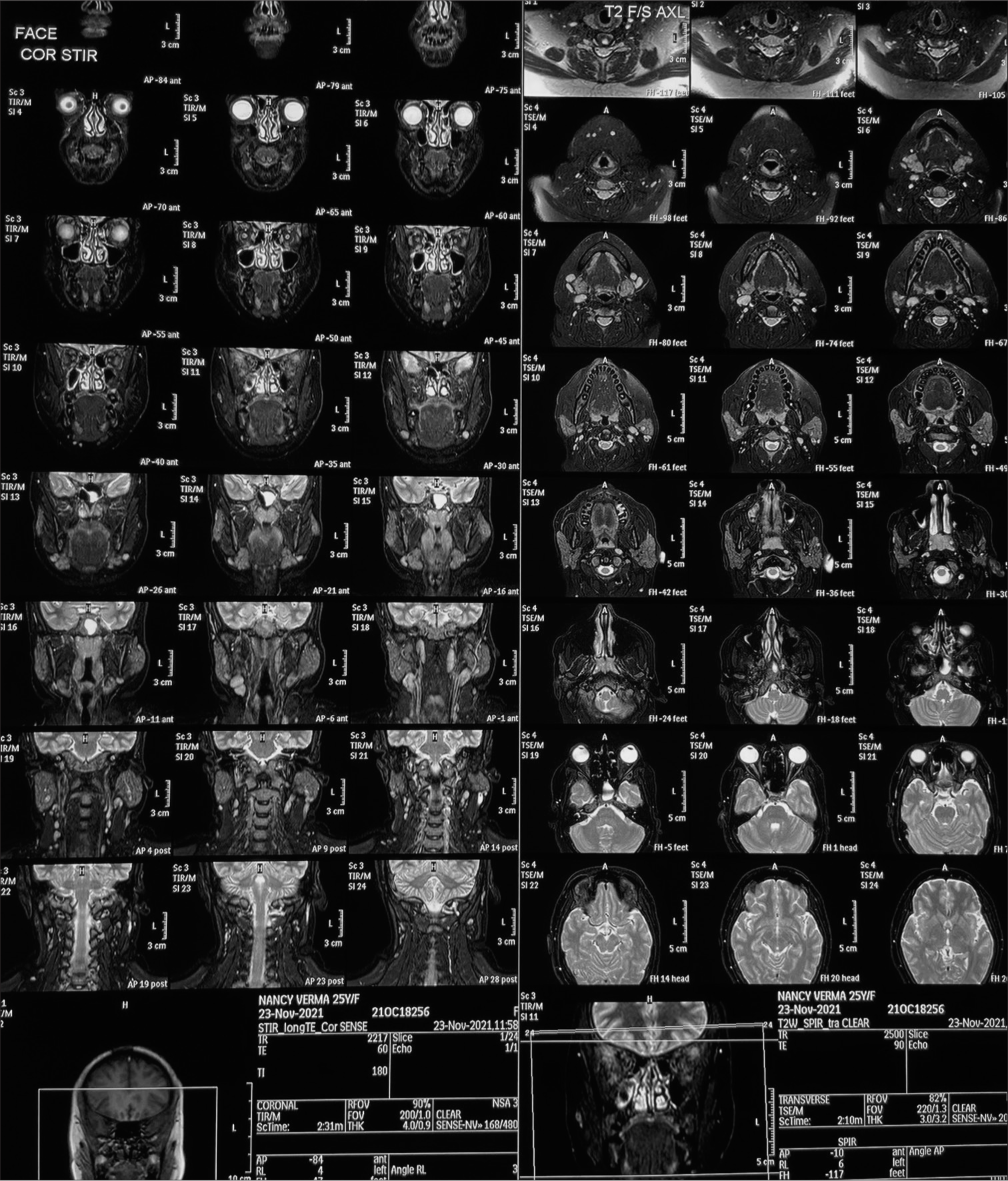
- Magnetic resonance imaging shows loss of fat over the face area.
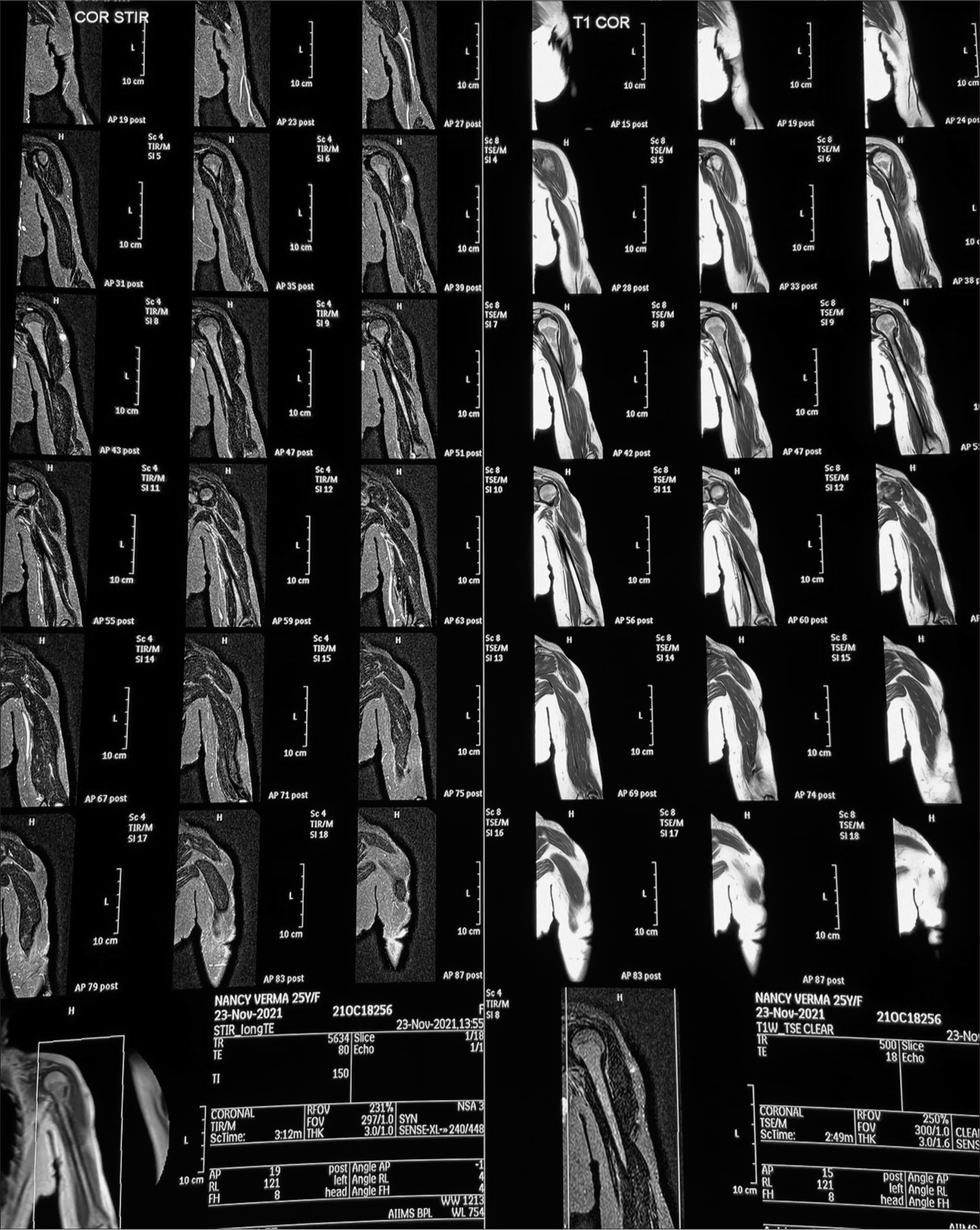
- Magnetic resonance imaging depicts the loss of the subcutaneous layer over arms with preserved fat over the chest area.
Methods
The donor site was selected from the abdominal area. Areas marked for fat harvest were infiltrated with tumescent anesthesia using a spinal cannula. Adequate time allowed for a proper anesthetic and hemostatic effect. Fat was then harvested with a special 2.1–2.4 mm “Tri-port” harvesting cannula. Attached to a 10 cc syringe using gently applied syringe suction to avoid vacuum barotrauma to the tissue.
Fat was harvested with continuous suctioning and to and fro motion of the Coleman cannula. The 30 cc fat harvested was centrifuged at the rate of 3000 revolutions per minute for 3 min in 10 cc syringes with needles bent. The blood settled in the down layer was removed, and the middle-fat layer and superficial aqueous component were retained. The recipient area was infiltrated with local anesthesia with adrenaline. The bilateral cheek area was injected with fat with slight over-correction over the left cheek using the 24 G needle, around 1 – 3 cc in the bilateral cheek and 2 cc in the buccal recess [Figure 6]. The patient was advised to avoid local massage and head end elevation, rest, and antibiotics for 1 week [Figure 7]. Slight atrophy and irregularities were seen in the right cheek after 6 months of follow-up may be due to under-correction at the time of the procedure or due to disease progression [Figure 8].

- The bilateral cheek area was injected with fat along the direction as depicted (black lines).

- Post-operative day 7 after surgical correction with fat transplant.

- Loss of left cheek fat due to under-correction and preserved fat transplant at 6 months of follow-up.
DISCUSSION
Lipodystrophy syndromes are characterized by loss of adipose tissue without any signs of dietary restriction, a catabolic state, or inflammation.4 APL or lipodystrophy progressive or BSS is mostly seen in 25 years (range, 4 – 65 years) with various theories in the pathogenesis, such as sequelae of severe viral infection like measles.5,6 Another theory is alternate complement pathway activation and C3 hypocomplementemia with adipocyte lysis brought on by C3NeF have been suggested as potential causes of fat loss in individuals with BSS, even though the precise process is still mostly understood. It is regarded as a crucial criterion for the differential diagnosis of this kind of lipodystrophy since C3 hypocomplementemia has been observed in 70 – 80% of individuals with BSS.7
BSS is characterized by cephalothoracic lipodystrophy, which affects the face, neck, arms, thorax, and upper abdomen in a cephalocaudal pattern. In contrast, the lower extremities and gluteal regions’ adipose storage often tend to be either enlarged or conserved.8 Contrary to other forms of lipodystrophy, insulin resistance and metabolic complications such as diabetes and hypertriglyceridemia seem to be less common and less severe.9
In 1893, Neuber was the first to discuss the concept of fat transplant to cure atrophic scars.10 Fat is the perfect soft-tissue filler, as it can integrate into the surrounding tissue at the injection site, is autologous, biocompatible, readily available in most patients, and is reasonably permanent.11 Although less information has been published about its safety and efficacy for facial reconstruction or esthetic improvement, its use in the facial region has also increased.
Types of autologous fat transplants include autologous free fat grafts, dermofat grafts, omental flaps, and free fat injections. In autologous free fat graft, a mass of tissue is harvested from any discrete subcutaneous location and implanted at a recipient site. Dermofat grafts are made from tissue that has been removed from a region, allowing for the removal of full-thickness skin grafts and the primary closure of defects. The dermofat graft can be employed as a spacer between gliding tissues or as a filler. Omental flaps are revascularized fat flaps, which can be utilized for microvascular transfer, soft-tissue filler for hemifacial atrophy, or to cover any significant skin defects. When fat is extracted, processed, and transplanted in liquid injectable form for a variety of purposes, it is known as free fat injection.11 Facial fat transfer has evolved from simple grafting techniques to micro-fat (smaller lobule) and nanofat (adipose-derived stem cell) injection techniques. During facial fat transplant, a top-up fat is injected to minimize the risk of fat loss post-procedure which was not done in our case. The volume of fat injected during fat transplantation in the face is depicted in Figure 9.12
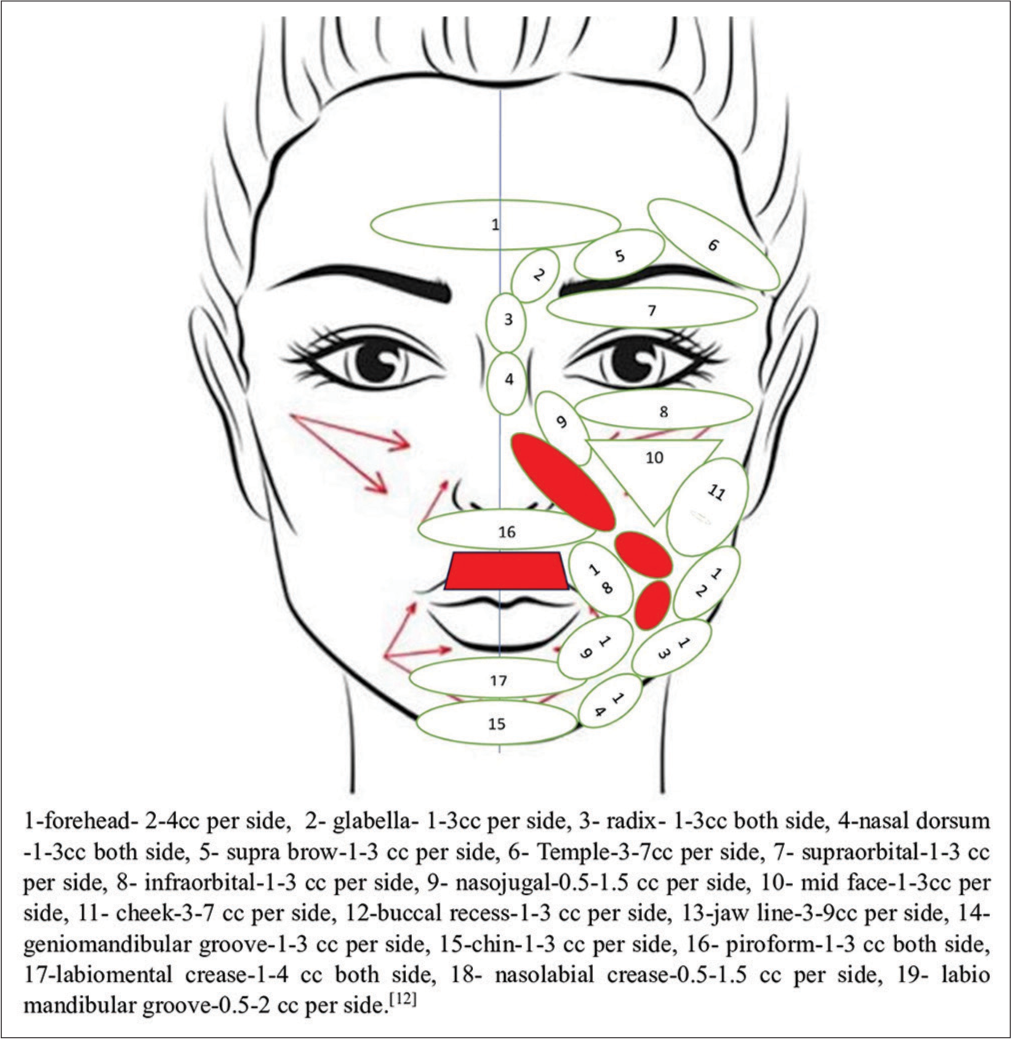
- The volume of fat to be injected during micro-fat graft over the face area. Red highlighted areas indicate places where fat transplants are avoided, whereas red arrows indicate the direction of fat injection.
Indications for fat injection for the face are nasolabial fold, marionette fold, cheeks and malar region, lips, chin, and periorbital rejuvenation. Dermatological conditions where a fat transplant is indicated are post-acne scarring, morphea, Romberg’s disease (hemifacial atrophy), lupus profundus, etc. The complications are either asymmetry or skin irregularities (excessive or inadequate grafting or graft survival), fat necrosis, infections, and fat embolism in the periorbital area.13
CONCLUSION
All things considered, Barquer simon syndrome is a rare acquired lipodystrophy. Through this case report we wanted to highlight the rare case of Baraquer Simon syndrome and fat transplant as a good therapeutic option.
Authors’ contributions
All authors discussed the results and contributed to the final manuscript. Shreya K. Gowda and Kapil Baheti played a pivotal role in manuscript preparation whereas, Sonali Gupta and Amulya M. Lakshman did the manuscript review. Lastly, All the authors along with Dinesh Asati contributed to intellectual content and in the design of the research.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patients consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Diagnosis and treatment of lipodystrophy: A step-by-step approach. J Endocrinol Invest. 2019;42:61-73.
- [CrossRef] [Google Scholar]
- Lipodystrophy syndromes. Endocrinol Metab Clin North Am. 2016;45:783-97.
- [CrossRef] [Google Scholar]
- Panniculitis. Part II. Mostly lobular paniculitis. J Am Acad Dermatol. 2001;45:325-64.
- [CrossRef] [Google Scholar]
- Clinical features and metabolic and autoimmune derangements in acquired partial lipodystrophy: Report of 35 cases and review of the literature. Medicine. 2004;83:18-34.
- [CrossRef] [Google Scholar]
- Barraquer-Simons syndrome: A rare form of acquired lipodystrophy. BMC Res Notes. 2016;9:175.
- [CrossRef] [Google Scholar]
- Two new cases of Barraquer-Simons syndrome. Am J Med Genet. 2004;126A:427-9.
- [CrossRef] [Google Scholar]
- Syndromes lipodystrophiqueslipodystrophies. Rev Méd Interne. 2013;34:614-22.
- [CrossRef] [Google Scholar]
- ACS (I) Textbook on cutaneous and aesthetic surgery. J Cutan Aesthet Surg. 2013;6:60.
- [CrossRef] [Google Scholar]
- Long-term survival of fat transplants: Controlled demonstrations. Aesthetic Plast Surg. 1995;19:421-5.
- [CrossRef] [Google Scholar]
- Microfat and nanofat: When and where these treatments work. Facial Plast Surg Clin North Am. 2019;27:321-30.
- [CrossRef] [Google Scholar]
- A systematic review of the effectiveness and complications of fat grafting in the facial region. JPRAS Open. 2019;19:87-97.
- [CrossRef] [Google Scholar]




