
Translate this page into:
Efficacy and safety of microneedling radiofrequency in acne scars
 , Surya Prasad Chilka1, Bommareddy Anargha1
, Surya Prasad Chilka1, Bommareddy Anargha1
*Corresponding author: Subhashini Konala, Department of Dermatology, Venereology, and Leprosy, GSL Medical College, Rajahmahendravaram, Andhra Pradesh, India. subha.konala@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Navyadevi U, Ganni S, Satya S, Konala S, Kolalapudi SA, Chilka SP, et al. Efficacy and safety of microneedling radiofrequency in acne scars. J Cutan Aesthet Surg. 2024;17:315-9. doi: 10.25259/jcas_175_23
Abstract
Objectives:
To study the efficacy and safety of microneedling radiofrequency (MNRF) in the treatment of acne scars.
Material and Methods:
This is a hospital-based and prospective interventional study. A total of 44 patients (18– 55 years old), skin types III-V, with acne scars, were enrolled. Four sessions of MNRF (Lumenis legend PRO Machine, with non-insulated needle tips GEN6, GEN6L; Israel) were done with an interval of 3 weeks between each session and followed up 1 month after the last session. The outcome was assessed by Goodman and Baron’s qualitative and quantitative acne scar grading, physician global assessment (PGA), and patient satisfaction score (PSS).
Results:
Out of 44 patients, four patients could not complete the study. Goodman and Baron’s qualitative assessment showed patients with Grades 2, 3, and 4 were 6 (15%), 17 (42.5%), and 17 (42.5%), respectively. At the end of follow-up, patients with Grades 1, 2, 4, and 4 acne scars were 5 (12.5%), 24 (60%), 10 (25%), and 1 (2.5%), respectively, which were statistically significant (P < 0.05). Seven patients showed no improvement. Goodman and Baron’s quantitative assessment showed an initial mean of 12.65 and an after-follow-up mean of 8.3, which was statistically significant (P < 0.05). PGA and PSS scores showed excellent to good responses of 70% and 82.5%, respectively. Adverse effects such as post-treatment erythema were seen in all patients, and edema was observed in 12 patients. Post-inflammatory hyperpigmentation was noted in two patients.
Conclusion:
MNRF was found to be effective with a better safety profile for acne scars.
Keywords
Acne scars
Microneedling radiofrequency
Neocollagenesis

INTRODUCTION
The most distressing and undesirable complication of acne vulgaris following inflammatory acne is post-acne scars.1 It causes low self-esteem, and an inferiority complex, and may also lead to severe psychological depression. The severity of acne scars is based on the severity and type of active acne and the healing ability of the patient.2 Scars that originate at the area of tissue injury induce either loss or excess collagen resulting in atrophic or hypertrophic/keloid acne scars, respectively.2,3 Atrophic acne scars are a more common type, which results after inflammatory acne due to the destruction of collagen.
Many treatment options are available, such as chemical peeling, dermabrasion, punch grafting, punch excision, punch elevation, subcision, fillers, ablative, and non-ablative lasers to improve acne scars.1,4 Management of these acne scars poses a therapeutic challenge to dermatologists, as a single modality is not effective in clearing all acne scars. Therefore, there is a need for a newer therapeutic approach that is safe, effective and has minimal downtime.
Recently, microneedling radiofrequency (MNRF) has emerged as a novel therapeutic option for acne scar resurfacing. Microneedles deliver radiofrequency current and create small zones of neocollagenesis, termed “radiofrequency thermal zones,” causing dermal remodeling.5,6 There is minimal damage to the epidermis, unlike lasers, where there is more damage to the epidermis, resulting in post-inflammatory hyperpigmentation (PIH).7 Due to this mechanism, apart from acne scars, MNRF is also used for skin rejuvenation, mild rhytides, large pores, hyperhidrosis, skin tightening, striae, and photoaging.
MATERIAL AND METHODS
Patient selection
The study was done after obtaining permission from the Institutional Ethics Committee (IEC/ERB Ref No: 706-EC/706–11/2020). The study period was between December 2020 and May 2022. Patients in the age group of 18–55 years of both genders with acne scars and skin types III-V attending our outpatient department were included in the study after taking consent. Patients with bleeding and clotting disorders, on anticoagulant therapy, uncontrolled diabetes, active infections, topical acne treatment 1-month before the study, any esthetic procedure on the face within the previous 6 months, metal implants in the treatment area, pregnant and lactating women, not willing to participate voluntarily, and patients with unrealistic expectations were excluded from the study.
Treatment protocol
Each patient had undergone four sessions of MNRF at 3-week intervals and follow-up was done 1 month after the last session. The device used was the Lumenis Legend Pro MNRF machine (Israel). Ultra-thin non-insulated needles GEN6 and GEN6L (length 0.6 mm and 1 mm, respectively), array 6 × 6, and width 35G were selected based on the type and depth of acne scars.
The face was first cleaned with rectified spirit followed by normal saline. Topical anesthetic cream was applied under occlusion for 30–45 min before the procedure. The entire face was cleaned with normal saline and pat dry. Ice cubes were applied over the treatment area before the procedure to reduce pain and discomfort.
The energy of either low (10%), medium (20%), or high (30%) was used based on the type of acne scars. Exposure from 15% to 25% was done. A pulse width of 400 ms and frequency of 1 MHz were used. The skin was gently stretched between two fingers, and the GEN6/GEN6L tip was kept perpendicular to the skin. Two passes of shots without stacking were given covering all the acne scars. In the first pass, energy, exposure, and depth will be higher focusing on deep scars, while in the second pass, settings were adjusted to lower levels focusing on superficial scars. Topical antibiotic cream was applied followed by sunscreen. The patient was advised post-procedure gentle skin care with a gentle cleanser and topical sunscreen and also advised to avoid sun exposure, soaps, pricking or rubbing of the skin, fumes/steam, sweating, and exercise.
Assessment
The patient’s skin type was determined by the Fitzpatrick scale of skin phototypes. Clinical photographs were taken at the beginning of each session and 1-month after the last session. Clinical assessment was done by physician global assessment (PGA) and patient satisfaction score (PSS). Improvement of the grade was assessed by Goodman and Baron’s qualitative and quantitative acne scar grading.8,9 Any side effects observed by the investigator or reported by the patient were recorded.
Statistical analysis
All statistical analysis was done using the Statistical Package for the Social Sciences software version 20.0 and Microsoft Excel 2010. Descriptive data were presented as mean ± standard deviation and percentages. The Chi-square test was done to evaluate the association between Goodman and Baron’s qualitative score. Paired t-test was done to evaluate the association between Goodman and Baron’s quantitative score. For all the statistical analyses, P < 0.05 was considered statistically significant.
RESULTS
The present study was a hospital-based prospective interventional study. A total of 44 patients were enrolled in the study, out of which the majority of the subjects were female (27, 61.4%) and males 17 (38.6%). Four patients could not complete the study due to personal reasons. The mean age of the study group was 27.05 ± 5.154 years, with a minimum age of 20 years and a maximum age of 40 years [Table 1].
| Mean age | 27.05±5.154 years. |
| Gender (%) | |
| Female (F) | 27 (61.4) |
| Male (M) | 17 (38.6) |
| Fitzpatrick skin type (%) | |
| III | 18 (40.9) |
| IV | 20 (45.45) |
| V | 6 (13.6) |
| Mean scar duration | 4.33±1.774 years |
| Minimum scar age | 1 year |
| Maximum scar age | 8 years |
| Goodman and Baron’s qualitative grade (%) | |
| Grade 1 | 0 |
| Grade 2 | 6 (15) |
| Grade 3 | 17 (42.5) |
| Grade 4 | 17 (42.5) |
| Goodman and Baron’s quantitative grade | |
| Mean at baseline | 12.65±5.352 |
Initially, using Goodman and Baron’s qualitative grading, patients with Grade 2 were 6 (15%), Grade 3 were 17 (42.5%), and Grade 4 were 17 (42.5%). During follow-up, the majority of the patients with Grade 4 and Grade 3 scars were improved to Grade 2 scars. At the end of follow-up, patients with Grade 1 acne scars were 5 (12.5%), Grade 2 were 24 (60%), Grade 3 were 10 (25%) and Grade 4 were 1 (2.5%) [Figures 1-3]. Seven patients showed no improvement. The Chi-square test was performed to assess the improvement, which showed a value of 31.837 and P = 0.001, which was statistically significant.
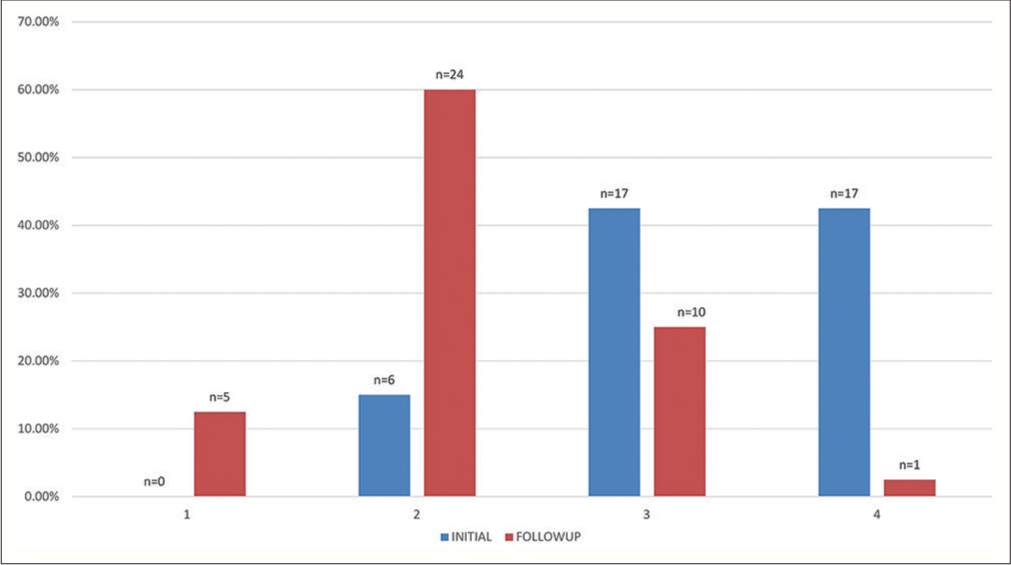
- Comparison of Goodman and Baron’s qualitative assessment grades among patients at baseline and at follow-up (1 month after the last session).

- Improvement in the acne scars from (a) grade 4 to (b) grade 2 during follow-up (1 month after the last session).

- Improvement in the acne scars from (a) grade 4 to (b) grade 3 during follow-up (1 month after the last session).
In Goodman and Baron’s quantitative acne scar grading, the mean at baseline was 12.65 ± 5.352 points and during follow-up was 8.30 ± 3.976 points. The overall percentage reduction in Goodman and Baron’s quantitative mean score was 34.35%, and the mean difference was 4.350 with P = 0.001. Among the scar types, rolling and boxcar scars showed superior response compared to icepick scars.
At the end of the follow-up period, PGA showed excellent improvement in 7 patients (17.5%), good in 21 patients (52.5%), moderate in 4 patients (10%), and minimal in 1 patient (2.5%). No improvement was observed in seven patients. PSS was excellent in 14 patients (35%), good in 19 patients (47.5%), moderate in 3 patients (7.5%), and minimal in 2 patients (5%). Two patients observed no improvement.
Adverse effects such as post-treatment erythema were observed in all the patients and edema in 12 patients, which were transient and subsided within 24 h. PIH was noticed in only two patients. No bleeding was observed during or post-treatment in any of the patients. There was no worsening of skin texture or any new scar formation or scab formation. We also observed improvement in facial contour and skin tightness in the majority of the patients.
DISCUSSION
Acne scarring, the sequelae of inflammatory acne, leads to psychological implications such as depression and suicidal tendencies, mainly in adolescents and young adults. Scarring is more typically seen in inflammatory acne than non-inflammatory acne. Inadequate response in healing results in diminished deposition of collagen, which leads to the formation of an atrophic scar, and if the healing response is too exuberant, a raised nodule of fibrotic tissue forms hypertrophic scars.2,3
Ablative and non-ablative lasers are also good therapeutic options for laser resurfacing, with an efficacy of 25–90%, but the main drawback is that they cause prolonged erythema and PIH.10
MNRF is a novel, minimally invasive technology for post-acne scar resurfacing. The energy delivered creates a pyramid shape of fractionated thermal zones, the impact of energy is narrow on the epidermal surface, wide, and deeper into the dermis. Controlled volumetric heating of the dermis triggers neocollagenesis by activating the cascade of growth factors involved in wound healing, including transforming growth factor-a (TGF-a), TGF-b, and platelet-derived growth factor.11,12 There were increased levels of type I and type II procollagen and elastin in the patients after treatment with MNRF.13 It has less downtime and side effects, such as PIH due to the melanin-sparing effect.14 Meta-analysis conducted by Dai et al. in six studies of MNRF in Asian patients showed that MNRF procedure was superior compared to fractional lasers for acne scars.15
In the present study, improvement by one grade was seen in 55% (22 patients), by two grades in 27.5% (11 patients), and seven people showed no improvement during 1 month of follow-up with Goodman and Baron’s qualitative scar grade. This is similar to Pudukadan16 who observed improvement by one grade in 11 out of 19 patients (57.9%) after 1 month of follow-up but observed improvement in all patients at the end of 3 months. Chandrashekar et al.17 observed two grades of improvement in 80.64% of patients, which is in contrast to our study (27.5%). This could be due to more gaps between the sessions and longer duration of follow-up compared to our study.
In Goodman and Baron’s quantitative acne scar grading, the overall percentage reduction in mean score was 34.39%, which was statistically significant. Rajput et al. observed a 60.72% reduction in the mean score.18 Only a few studies are available using this quantitative scar grading.18
In the PGA score, improvement was good to excellent in 70% of patients. Similar observations were documented by other workers such as Harth et al.19 (75%), and Rajput et al.18 (89%), whereas Bulbul Baskan and Akin Belli1 observed a 44.4% improvement, which was less. This could be due to the smaller sample size and difference in the number of sessions among the individuals in their study. In our study, PSS showed improvement from excellent to good in 82.5% of patients. Cho et al.20 observed an improvement of 86.7% which is similar to our study. Kim et al.13 and Eubanks and Solomon21 observed improvement of 93.56% and 91.3%, respectively, which is slightly higher than our study, whereas Bulbul Baskan and Akin Belli1 observed good response only in 33%, and excellent response was not seen in any.
PSS scores were higher compared to PGA scores, thus suggesting patient satisfaction was higher compared to actual clinical improvement, which may be due to MNRF having skin tightening and rejuvenation effects.
Adverse effects observed were post-treatment erythema in all patients and edema in 30% (12 patients), which were transient and subsided within 24 h. However, in a few studies, erythema took a longer time to resolve and this could be due to differences in treatment settings. PIH was noticed in only two patients, which is similar to the study by Pudukadan16 This lower incidence of PIH was due to the sparing of melanocytes by radiofrequency technology.
Out of scar subtypes, rolling scars and boxcar scars responded better compared to ice pick scars which is similar to the study by Chandrashekar et al.17 and Cho et al.20
In comparison to a single modality approach, combination therapies are more effective at treating acne scars. MNRF alone can be a reasonable alternative, as there was a significant improvement with minimal downtime. Very few studies are available using MNRF alone for acne scars, this study adds value to the existing literature.16,17,21
Limitations
The follow-up period was short in our study. A longer follow-up might have given much more better results.
CONCLUSION
MNRF was found to be efficient in managing post-acne scars in Indian skin types with a better safety profile. It also showed a high PSS along with skin tightening and rejuvenation effects.
Authors’ contributions
All the authors have made substantial contributions in intellectual content, conceptualizing and designing of the work, the analysis and interpretation of the data, as well as the writing of the manuscript.
Ethical approval
The research/study approved by the Institutional Ethics Committee (IEC/ERB Ref No: 706-EC/706–11/2020)., dated 12/11/2020.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Evaluation of the efficacy of microneedle fractional radiofrequency in Turkish patients with atrophic facial acne scars. J Cosmet Dermatol. 2019;18:1317-21.
- [CrossRef] [Google Scholar]
- Acne scars: Pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080.
- [CrossRef] [Google Scholar]
- Management of acne scarring, part II. Am J Clin Dermatol. 2012;13:331-40.
- [CrossRef] [Google Scholar]
- Acne scar treatment: A multimodality approach tailored to scar type. Dermatol Surg. 2016;42:S139-49.
- [CrossRef] [Google Scholar]
- Radiofrequency microneedling for acne, acne scars, and more. Dermatol Rev. 2020;1:33-7.
- [CrossRef] [Google Scholar]
- Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8:259-65.
- [Google Scholar]
- Combined use of monopolar radiofrequency and transdermal drug delivery in the treatment of melasma. Dermatol Surg. 2014;40:748-55.
- [Google Scholar]
- Postacne scarring: A qualitative global scarring grading system. Dermatol Surg. 2006;32:1458-66.
- [CrossRef] [Google Scholar]
- Postacne scarring-a quantitative global scarring grading system. J Cosmet Dermatol. 2006;5:48-52.
- [CrossRef] [Google Scholar]
- Laser resurfacing of skin for improvement of acne scarring: A systematic review of evidence. Br J Dermatol. 2000;142:413-23.
- [CrossRef] [Google Scholar]
- Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17:51-63.
- [CrossRef] [Google Scholar]
- Bipolar fractional radiofrequency treatment induces neoelastogenesis and neocollagenesis. Lasers Surg Med. 2009;41:1-9.
- [CrossRef] [Google Scholar]
- Objective evaluation of the clinical efficacy of fractional radiofrequency treatment for acne scars and enlarged pores in Asian skin. Dermatol Surg. 2014;40:988-95.
- [CrossRef] [Google Scholar]
- Comparison of a fractional microplasma radio frequency technology and carbon dioxide fractional laser for the treatment of atrophic acne scars: A randomized split-face clinical study. Dermatol Surg. 2013;39:559-66.
- [CrossRef] [Google Scholar]
- The efficacy and safety of the fractional radiofrequency technique for the treatment of atrophic acne scar in Asians: A meta-analysis. J Cosmet Laser Ther. 2017;19:337-44.
- [CrossRef] [Google Scholar]
- Treatment of acne scars on darker skin types using a noninsulated smooth motion, electronically controlled radiofrequency microneedles treatment system. Dermatol Surg. 2017;43:S64-9.
- [CrossRef] [Google Scholar]
- Evaluation of microneedling fractional radiofrequency device for treatment of acne scars. J Cutan Aesthet Surg. 2014;7:93-7.
- [CrossRef] [Google Scholar]
- A prospective, nonrandomized, open-label study, comparing the efficacy, safety, and tolerability of fractional CO2 laser versus fractional microneedling radio frequency in acne scars. J Cutan Aesthet Surg. 2021;14:177-83.
- [CrossRef] [Google Scholar]
- Depressed acne scars effective, minimal downtime treatment with a novel smooth motion non-insulated microneedle radiofrequency technology. J Cosmet Dermatol Sci Appl. 2014;4:212-8.
- [CrossRef] [Google Scholar]
- Evaluation of the clinical efficacy of fractional radiofrequency microneedle treatment in acne scars and large facial pores. Dermatol Surg. 2012;38:1017-24.
- [CrossRef] [Google Scholar]
- Safety and efficacy of fractional radiofrequency for the treatment and reduction of acne scarring: A prospective study. Lasers Surg Med. 2022;54:74-81.
- [CrossRef] [Google Scholar]




