
Translate this page into:
Unravelling harpoon nail: Surgical outcome and insights
*Corresponding author: Joy Dhirendranath Das, Department of Dermatology, Venereology and Leprosy, Vedantaa Institute of Medical Sciences, Dahanu, Maharashtra, India. jad6688@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shah SS, Firdaus Z, Das JD, Shah YM. Unravelling harpoon nail: Surgical outcome and insights. J Cutan Aesthet Surg. doi: 10.25259/JCAS_62_2024
Abstract
An ingrown toenail (onychocryptosis) is a chronic, painful condition, especially prevalent among adolescents. A rare variant, termed “harpoon nail,” involves a sharp spike of the nail plate penetrating deep tissue, causing inflammation and granulation tissue formation. Such cases are seldom reported in India, and improper nail cutting is the most common cause. This condition typically affects the hallux, particularly its outer edge, leading to a nail spur that pierces surrounding soft tissues, forming a channel. Factors such as trauma, excessive sweating, and tight shoes can exacerbate the condition by compressing the nail fold against the nail plate, sometimes leading to secondary bacterial infections. Here, we present a unique and rare case of a distal lateral ingrowing toenail-harpoon nail and its surgical management. A 28-year-old Indian female presented with severe pain and swelling in the left hallux for 5 years. Examination revealed hypertrophic soft tissue covering the distal nail plate, which extended 3 mm beyond this tissue. She was diagnosed with a harpoon nail due to hypertrophy of both lateral and distal nail folds. The modified Winograd technique was used for surgical correction and ablation of the germinal matrix was done by radiocautery. The procedure was minimally invasive, quick, and effective, resulting in high patient satisfaction and low recurrence rates. During follow-up visits, the patient reported no difficulty in wearing shoes, and her left hallux appeared normal and healthy, with proper alignment and no nail dystrophy. This case underscores the effectiveness of the modified Winograd technique in managing harpoon nails, providing both functional and cosmetic benefits.
Keywords
Harpoon nail
Ingrown toenail
Onychocryptosis
Granulation tissue
Modified Winograd procedure

INTRODUCTION
An ingrown toenail (onychocryptosis) is a chronic and painful condition affecting adolescents. In a rare variant called “harpoon nail,” a sharp spike of the nail plate penetrates deep tissue, which results in inflammation and granulation tissue formation.1 Such cases are rare in occurrence, and only a few are reported in India. The most common cause of the harpoon nail is improper cutting of the nail.2 It typically affects the hallux, especially its outer edge, causing a nail spur that pierces surrounding soft tissues, which leads to channel formation.1 Trauma, excessive sweating, and tight shoes can worsen this condition, as it compresses the nail fold against the nail plate. Sometimes, it can be complicated by secondary bacterial infection.3 Hereby, we describe a unique and rare variant of the distal lateral ingrowing toenail - the harpoon nail and its surgical management.
CASE REPORT
A 28-year-old Indian female presented with severe pain and swelling in the left hallux for 5 years. Her prior treatments included analgesics and local dressing. On examination, the distal nail plate was found to be covered with hypertrophic soft tissue, extending 3 mm beyond this tissue [Figures 1 and 2]. The patient showed no signs of infection, and pre-operative antibiotics were not administered. Only induration and a localized increase in temperature were observed on palpation. She was diagnosed with a harpoon nail due to both lateral and distal nail fold hypertrophy.

- Dorsal view of the left hallux showing hypertrophic nail folds covering the distal nail plate.

- Frontal view of the left hallux showing granulation tissue and extended nail plate distally.
Surgical technique
The left forefoot was prepped and draped using betadine, and hemostasis was achieved with a rubber tourniquet. The nail surgery was performed under a proximal digital block, using 2% xylocaine infiltrated into the medial and lateral aspects of the left hallux. Initially, the hypertrophic tissue covering the nail plate was excised, and the underlying granulation tissue was removed with a nail spatula. Approximately 15% of the medial and lateral nail plates were resected using Adson’s forceps and scissors, followed by the application of the modified Winograd technique to excise the hypertrophic nail folds [Figure 3a and b]. The lateral horn of the matrix was ablated by radiocautery using a tungsten electrode that was flat and bent at an angle. The electrode was placed for 3–5 s and it was repeated 2–3 times. The remaining nail fold tissue was advanced to the nail plate and sutured with 4–0 ethilon bilaterally and distally [Figure 4]. The tourniquet was then removed, showing an immediate hyperemic response and prompt capillary refill distally. The soft tissue was granular without any pus or non-viable tissue. The patient was discharged with a short course of prophylactic antibiotics and analgesics. At the first follow-up visit a week later, the sutures were removed, and the nail unit showed minimal inflammation. Thus, a modified Winograd procedure with matricectomy using radiocautery was chosen for the surgical correction of this rare case.
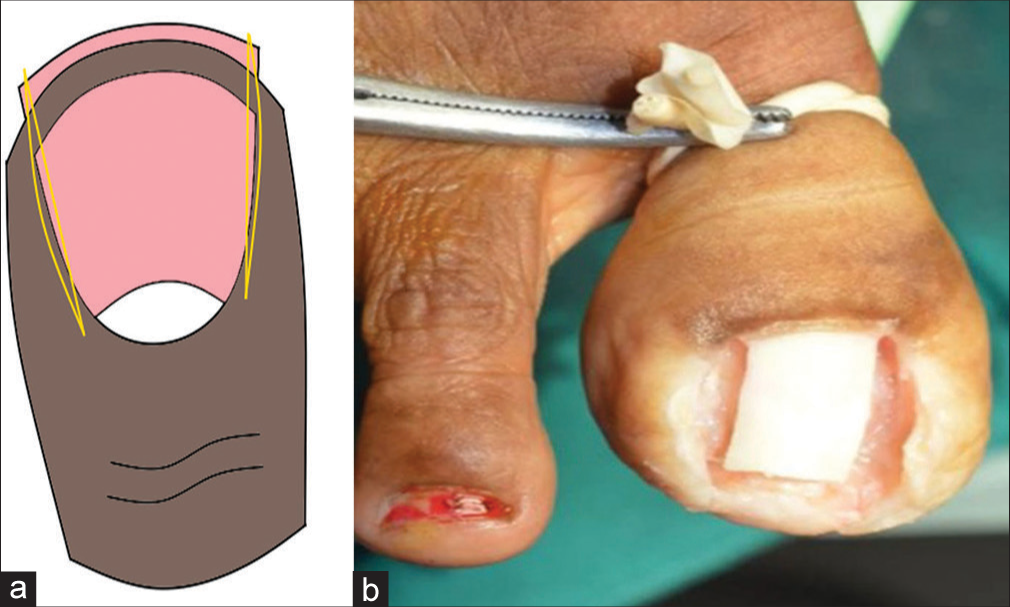
- (a) Diagrammatic representation of wedge resection of lateral nail folds in a harpoon nail and (b) dorsal view of left hallux after excision of nail plate and nail fold.

- Immediate post-operative photograph after suturing of both lateral and distal folds.
Results
The modified Winograd technique, along with radiocautery for matricectomy, effectively treated the rare harpoon nail variant of onychocryptosis. During regular follow-up visits, the patient reported no complaints about wearing shoes. After 2 years, the patient’s left hallux appeared normal and healthy, with proper alignment, no nail dystrophy, and satisfactory cosmetic results [Figure 5].

- Post-operative photograph of the left hallux.
DISCUSSION
This rare variant of onychocryptosis was first described by Richert (2014).4 They called it “a harpoon nail” because it looks like a marine hunting tool with a pointed tip and a broad base.4 It results from a vicious cycle of pain, edema, and faulty technique of nail clipping. When a patient tries to relieve pain from an ingrown nail by adjusting the side of the nail plate but cannot reach the outermost and deepest part of the nail plate, a lateral nail fragment can be left behind. This fragment then grows into a nail spicule, piercing through the surrounding tissue and creating a fistulous path that surfaces in the hyponychium.1 In the acute stage, it manifests with erythematous, edematous swelling with oozing and crusting, and if left untreated, progresses to the chronic form, where the inflammation resolves and the epithelialization of the fistulous tract takes place.4
Onychocryptosis can be classified into different stages as described by Heifetz,5 Frost,6 Martinez Nova et al.,7 and Mozena,8 with some modifications among them. This rare variant, known as the Harpoon nail, is classified solely by Mozena as stage 4, characterized by hypertrophic tissue entirely covering the medial, lateral, and distal nail plate.8 However, this staging system does not account for the formation of unilateral spur, bilateral spur, or complete nail plate penetration from the distal hypertrophied nail fold.
We propose classifying the harpoon nail into three stages. This will help categorize the severity and guide appropriate treatment options for patients presenting with this rare condition [Figure 6].
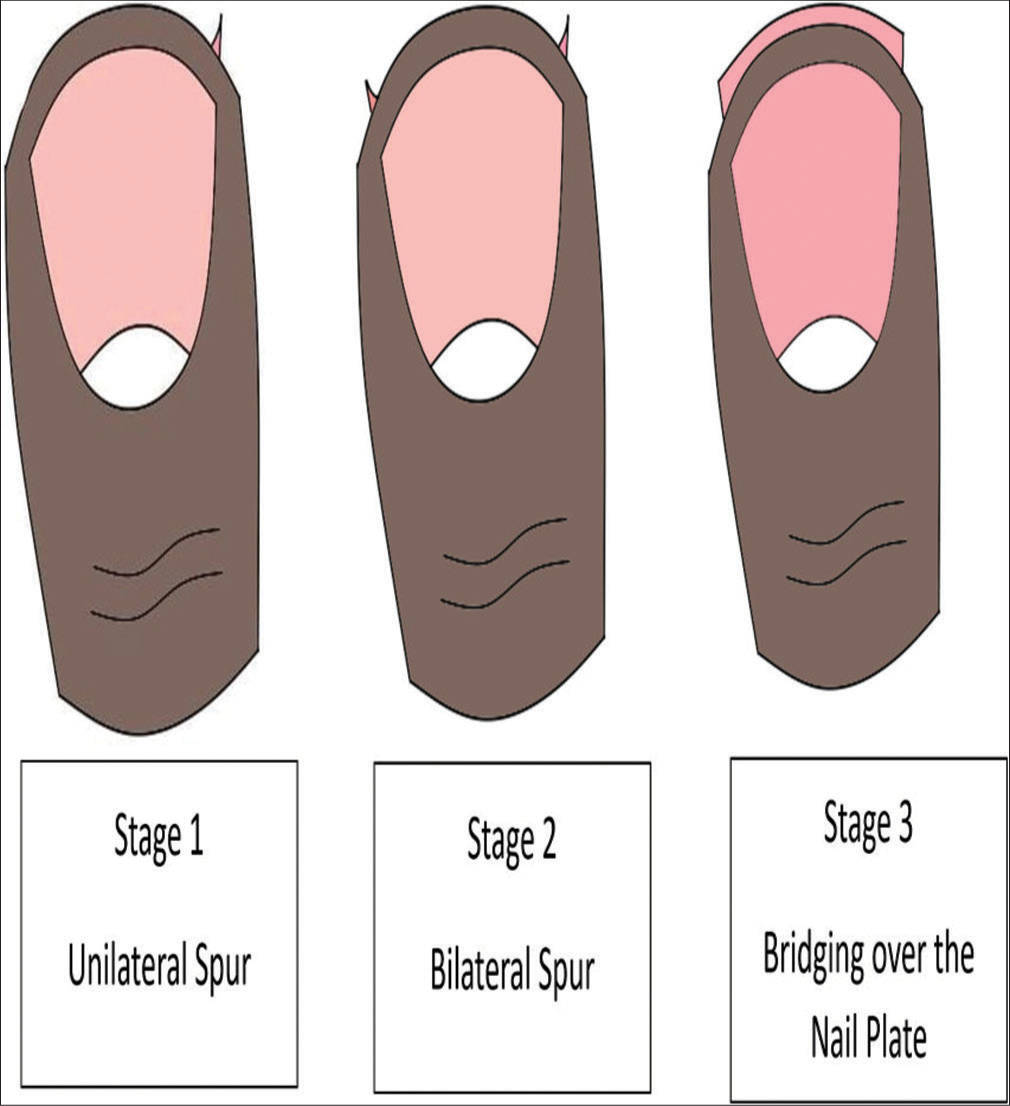
- Harpoon nail staging system.
Surgery remains the primary treatment for harpoon nails.1 The modified Winograd technique offers significant advantages over the traditional method, including precise curette removal of the germinal matrix and nail fold, followed by radiocautery. This approach is minimally invasive, quick, and highly effective, resulting in high patient satisfaction and low recurrence rates. In addition, it is preferred for its cosmetic benefits and minimal tissue damage.9 Other treatment options, such as the Vandenbos procedure, Zadik’s method, or the Super U technique, involve debulking all periungual soft tissues to expose the spicule. However, these alternatives tend to cause more tissue damage and require a longer healing time.10,11
CONCLUSION
The excessive soft-tissue hypertrophy seen in harpoon nails can be successfully managed with the modified Winograd technique. This method yields high patient satisfaction by achieving both functional and cosmetically pleasing outcomes.
Authors’ contributions
Dr Samkit S Shah performed the surgery and definition of intellectual content. Dr Zeenat-ul-Firdaus assisted in the surgery and contributed to manuscript preparation. Dr Joy D Das designed and edited. Dr Yogesh M Shah reviewed the manuscript.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Harpoon nail: An unusual form of onychocryptosis. Surg Cosmet Dermatol. 2022;14:e20220107.
- [CrossRef] [Google Scholar]
- An uncanny kin of the ingrown toenail: Harpoon. Nail and the surgical challenge in its management. J Cutan Aesthet Surg. 2020;13:142-4.
- [CrossRef] [PubMed] [Google Scholar]
- Algorithm for the management of antibiotic prophylaxis in onychocryptosis surgery. Foot. 2010;20:140-5.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical approach to harpoon nail: a new variant of ingrowing toenail. Dermatol Surg. 2014;40:700-1.
- [Google Scholar]
- Atraumatic nail avulsion with a novel ungual elevator. J Am Podiatry Assoc. 1958;48:51-3.
- [Google Scholar]
- A new onychocryptosis classification and treatment plan. J Am Podiatr Med Assoc. 2007;97:389-93.
- [CrossRef] [PubMed] [Google Scholar]
- The Mozena Classification System and Treatment Algorithm for Ingrown Hallux Nails. JAPMA. 2002;92:131-5.
- [CrossRef] [PubMed] [Google Scholar]
- A minimally-invasive, simple, rapid, and effective surgical technique for the treatment of ingrown toenails: A reminder of the original Winograd procedure. Int J Environ Res Public Health. 2021;18:278.
- [CrossRef] [PubMed] [Google Scholar]
- Definition-pathogenesis risk factors-classification-scoring In: Management of ingrowing nails: Treatment scenarios and practical tips. Germany: Springer; 2016. p. :35-58.
- [CrossRef] [Google Scholar]
- Surgical approach to harpoon nail: A new variant of ingrowing toenail. Dermatol Surg. 2014;40:700-1.
- [Google Scholar]




