
Translate this page into:
Split-face comparative case series of intralesional radiofrequency ablation and carbon dioxide laser pinhole ablation for syringoma
*Corresponding author: C. Madura, Department of Dermatosurgery, CUTIS Academy of Cutaneous Sciences, Bengaluru, Karnataka, India. maduradr@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nehete SS, Madura C, Chandrashekar BS. Split-face comparative case series of intralesional radiofrequency ablation and carbon dioxide laser pinhole ablation for syringoma. J Cutan Aesthet Surg. doi: 10.25259/JCAS_25_2025
Abstract
Syringomas are benign adnexal tumors originating from the intraepidermal part of eccrine glands, commonly appearing as skin-colored papules in the periorbital region. These lesions are usually asymptomatic, cosmetic concerns being more prominent. Among various treatment modalities, intralesional radiofrequency ablation and carbon dioxide (CO2) laser pinhole ablation are well-established treatments. This study aimed to compare the efficacy of these two techniques in a split-face manner. To minimize adverse events and downtime, intralesional radiofrequency (RF) on the one side and CO2 laser on the other side were performed. Since RF was applied only to the lesion’s center, the CO2 laser was also limited to pinhole ablation with conservative parameters. Five female patients aged 23–57 years with syringoma underwent treatment, with the left side of the face receiving intralesional radiofrequency ablation and the right side undergoing CO2 laser pinhole ablation. Post-procedure, lesion reduction was assessed after 1 month using lesion count, the Global Improvement Scale, and the Patient Satisfaction Scale. Results showed that intralesional radiofrequency ablation led to an average reduction of 41% in lesion count, compared to 10.3% with CO2 laser pinhole ablation. In comparison to CO2 laser pinhole ablation of the syringoma, intralesional RF ablation with an insulated insulin needle stands to be a more efficient treatment at a much lesser cost. However, careful patient selection based on skin type should be done.
Keywords
Carbon dioxide laser
Intralesional radiofrequency
Pinhole ablation
Syringoma

INTRODUCTION
Syringomas are benign adnexal tumors clinically presenting as skin-colored to brown-colored papules of 1–5 mm in size.1 These are commonly seen around the periorbital area but uncommonly found on the neck, chest, and axillae. They occur predominantly in females and can develop at any age, although peak incidence between the third and fourth decades.1 Syringomas are usually asymptomatic and do not require treatment unless they cause cosmetic concerns or discomfort.
Multiple options for treating syringoma include electrodessication, surgical excision, cryotherapy, and carbon dioxide (CO2) laser.2,3 Other options include the use of two of the commonly known options for the treatment of syringoma including intralesional radiofrequency ablation and CO2 laser pinhole ablation.4 Radiofrequency is a technology that uses modulated current to destroy the tissue. Intralesional radiofrequency ablation indicates that the energy is directly delivered into the tissue, sparing the epidermal part. CO2 laser is an ablative laser that destroys the tissue with a laser beam. This study aims to compare the efficacy and safety of two techniques, intralesional radiofrequency ablation and CO2 pinhole ablation, for syringoma management.
METHODOLOGY
This is a prospective split-face (left-right) comparative case series, which was conducted at Cutis Academy of Cutaneous Sciences, Bengaluru, India. After informed consent, patients diagnosed clinically with syringoma were included in the study. Patients with a history of any procedure being done for syringoma in the past 2 months were excluded. Due ethical approval was sought and a clinical trial was registered. The study was done during the period from December 2023 to June 2024. The treatment was performed under topical local anesthesia using a eutectic mixture of lidocaine 2.5% and prilocaine 2.5%. Syringomas on the left side of the face were treated with intralesional radiofrequency ablation. The tip of the insulin syringe needle was insulated using cyanoacrylate glue except for the distal most part. The needle was inserted into the bulk of the syringoma, and a radiofrequency probe was applied to the needle. The radiofrequency machine used was UM-150A with the settings (Cut mode 0.1). Syringomas on the right side of the face underwent CO2 laser ablation using the pinhole technique with CO2 point beam (point beam at the center, 1–2 Watt/10 Millisecond/2 passes). The machine used was the Ultrapulse CO2 machine. To minimize adverse events and downtime, intralesional RF on the one side and CO2 laser on the other side were performed. Since RF was applied only to the lesion’s center, the CO2 laser was also limited to pinhole ablation with conservative parameters. Post-procedure care included the application of an antibiotic cream for 5 days. Patients were also advised to follow strict photoprotection measures and use sunscreen regularly. Data regarding the number of lesions was counted before and after 1-month post-treatment and photographic comparisons were assessed using a Global Improvement Scale and Patient Satisfaction Scale as given in Table 1.
| Global improvement scale | Patient satisfaction scale | ||
| Grades | Total number of syringoma lesions | Grades | Patient’s satisfaction |
| Grade 0 | Worsened | Grade 0 | Worsened |
| Grade 1 | Minimal improvement (up to 25%) | Grade 1 | Poor |
| Grade 2 | Moderate improvement (26–50%) | Grade 2 | Slightly satisfied |
| Grade 3 | Marked improvement (51–75%) | Grade 3 | Satisfied |
| Grade 4 | Near total improvement (>75%) | Grade 4 | Very satisfied |
CASE DETAILS
Five female patients (ages 23–57) with Fitzpatrick skin types 3–5 underwent treatment [Table 2]. Case 1 showed a reduction from 25 to 13 syringomas on the left and 28– 25 on the right. Case 2 had hyperpigmented syringomas, decreasing from 10 to 4 on the left and 12–9 on the right. Case 3 saw a reduction from 11–4 (left) to 15–13 (right). Case 4 had syringomas decrease from 13–5 (left) to 16–15 (right). Case 5 showed minimal reduction (25–23) and developed post-inflammatory hyperpigmentation with scarring on the left.
RESULTS
A total of 5 patients were assessed for split-face comparison with ages of the patients ranging from 23 to 57 years. Duration of syringoma ranged from 4 years to 10 years. Three patients reported progression of syringoma, and two did not. Treatments taken included topical or laser treatment taken earlier. Sun exposure varied from 2 to 4 h daily. It was noted that the percentage of reduction in the average number of syringomas from baseline to post-procedure after 1 month was 41% for the intralesional side, whereas it was as low as 10.3% over the carbon dioxide laser side. While comparing, mean global improvement scale for the left side (RF side) was 2.6, but for the right side (CO2 laser side) was as low as 1. The patient satisfaction scale for the RF side was 2.2 and for the CO2 laser side was 1.4 [Table 2].
| Age | Sex | Skin type | Left side (Intralesional RF) | |||||
| Baseline O/E | Baseline left number | Post left | Global improvement scale | Patient satisfaction | Complications | |||
| 27 | F | 4 | Skin coloured | 25 | 13 | 3 | 1 | Nil |
| 54 | F | 4 | Hyperpigmented | 10 | 4 | 3 | 3 | Nil |
| 43 | F | 5 | Skin coloured | 11 | 4 | 3 | 3 | Nil |
| 23 | F | 3 | Skin coloured | 13 | 5 | 3 | 2 | Nil |
| 57 | F | 5 | Hyperpigmented | 25 | 23 | 1 | 2 | PIH; Scarring |
| Average: | 16.8 | 9.8 | 2.6 | 2.2 | ||||
| Age | Sex | Skin type | Right side (CO2 laser pinhole technique) | |||||
| Baseline O/E | Baseline right number | Post right number | Right global improvement scale | Right patient satisfaction | Complications | |||
| 27 | F | 4 | Skin coloured | 28 | 25 | 1 | 1 | Nil |
| 54 | F | 4 | Hyperpigmented | 12 | 9 | 1 | 2 | Nil |
| 43 | F | 5 | Skin coloured | 15 | 13 | 1 | 1 | Nil |
| 23 | F | 3 | Skin coloured | 16 | 15 | 1 | 2 | Nil |
| 57 | F | 5 | Hyperpigmented | 26 | 23 | 1 | 1 | PIH |
| 19.4 | 17 | 1 | 1.4 | |||||
CO2: Carbon dioxide, PIH: Post inflammatory hyperpigmentation, O/E: On examination, F: Female, RF: Radiofrequency
DISCUSSION
The data indicate that intralesional RF ablation yields superior lesion reduction compared to CO2 laser pinhole ablation, particularly evident in patients with lighter skin types [Figure 1]. Ablating the whole lesion using radiofrequency or with CO2 laser beam might lead to excessive tissue damage, increasing downtime and increasing chances for adverse events. Thus, intralesional radiofrequency or pinhole ablation using CO2 laser with conservative parameters where only the center of the lesion is ablated was used in this study. There is the least amount of lateral spread of energy for CO2 laser beams, but for radiofrequency, it is higher as compared to CO2 lasers. This might be a probable explanation behind better outcomes for the intralesional radiofrequency side. Thus, to choose a safer way to treat syringoma, one can opt for intralesional radiofrequency. Patients with Fitzpatrick skin type 3 with a relatively lower risk of PIH demonstrated a Global Improvement Score of 3.
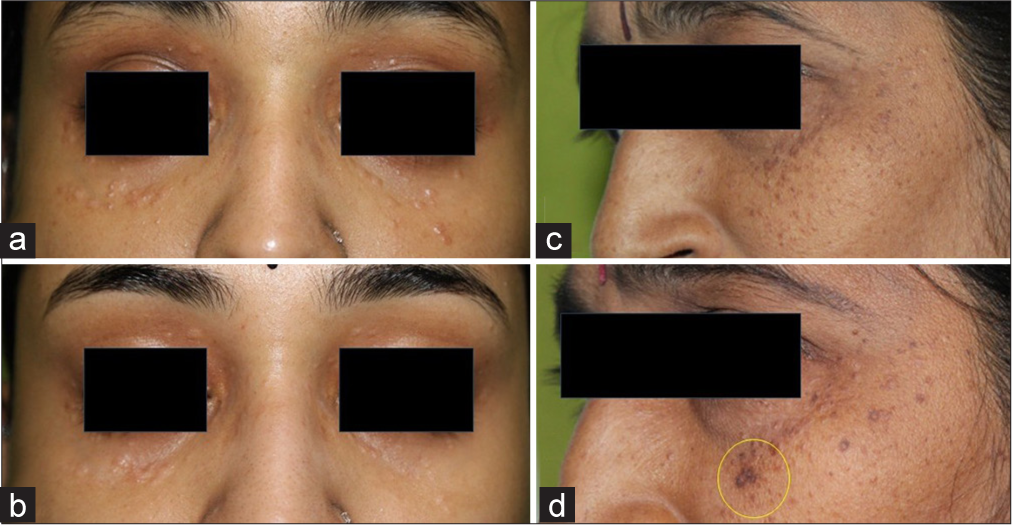
- (a and b) Before and after photographs: Good improvement on the left side of the face (intralesional radiofrequency) as compared to right side (carbon dioxide laser pinhole ablation). (c and d) Before and after photographs: Post-inflammatory hyperpigmentation and scarring after intralesional radiofrequency. Yellow Circle shows an area where post-inflammatory pigmentation was noted.
In contrast, a patient with Fitzpatrick skin type 5 with and not using inadequate sunscreen exhibited PIH and scarring [Figure 1]. The limitation of this method includes the skill of applying the glue uniformly over the needle without skip areas. Any kind of inadequacy of insulation will lead to a high chance of PIH. However, the risk is more seen in individuals with darker skin types and those with unprimed skin using inadequate sunscreen. Pre-procedure skin priming and post-procedure sun protection are essential to mitigate these risks. Further studies with larger, diverse cohorts and longer follow-ups can be done; one established finding from this study is that the RF technique described should be used with caution in individuals with darker skin types due to the risk of post-inflammatory pigmentation.
CONCLUSION
In comparison to CO2 laser pinhole ablation of the syringoma, intralesional RF ablation with an insulated insulin needle stands to be more efficient treatment at much lesser cost. However, careful patient selection based on skin type, priming of the skin and post-procedure care is crucial as the chances of complications are higher. The carbon dioxide laser, pinhole technique can be considered a comparatively safer technique, though it requires more sessions to treat syringoma effectively.
Authors’ contributions:
Sanket Sanjay Nehete: Concept, making the manuscript, collection of data, analysis of data, writing manuscript, editing manuscript, Dr Madura C: Concept, edit and review manuscript ; B. S. Chandrashekar: Concept, review of manuscript.
Ethical approval:
The research/study was approved by the Institutional Review Board at Cutis Institutional Ethics Committee, number ECR/930/Inst/KA/2017/RR-20, dated November 29th, 2023.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242-6.
- [CrossRef] [PubMed] [Google Scholar]
- Eruptive syringomas: Summary of ninety cases and a brief literature review. J Cosmet Dermatol. 2023;22:1128-33.
- [CrossRef] [PubMed] [Google Scholar]
- Laser therapy for treatment of syringoma. Egypt J Hospital Med. 2023;90:1651-4.
- [CrossRef] [Google Scholar]
- Comparison of microinsulated needle radiofrequency and carbon dioxide laser ablation for the treatment of syringoma. Dermatol Ther. 2019;32:e12912.
- [CrossRef] [PubMed] [Google Scholar]




