
Translate this page into:
A rare presentation of labial porokeratosis: An innovative approach yielding exceptional esthetic results

*Corresponding author: Yogesh M. Bhingradia, Department of Dermatology, Venereology and Leprosy, Shivani Skin Care and Cosmetic Clinic, Surat, Gujarat, India. yogeshbhingradia@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhingradia YM, Farista A, Solanki VG, Mehra M. A rare presentation of labial porokeratosis: An innovative approach yielding exceptional esthetic results. J Cutan Aesthet Surg. doi: 10.25259/ jcas_161_23
Abstract
Porokeratosis (PK) is a rare genodermatosis characterized by abnormal keratinization, resulting in crateriform lesions with central atrophy and distinct ridge-like borders. We present an unusual case of isolated labial PK in a 50-year-old female without oral mucosal involvement. The patient underwent successful treatment with CO2 laser ablation, resulting in complete resolution without recurrence during a 9-month follow-up period.
Keywords
Labial porokeratosis
CO2 Laser ablation
Laser

INTRODUCTION
Porokeratosis (PK) is a rare dermatological condition characterized by abnormal keratinization, typically presenting as single or multiple lesions with crateriform morphology, central atrophy, and well-defined ridge-like borders. This condition can manifest in various subtypes, both localized and generalized, and can occur anywhere on the body.1 Involvement of mucosae, palms, soles, and genitalia is exceedingly rare.2 We report a unique case of isolated labial PK, a rare presentation, which was successfully treated with CO2 laser ablation.
CASE REPORT
A 50-year-old female presented with a raised lesion on her upper lip that had been progressively growing for 3 years. The lesion exhibited centrifugal expansion and occasional pain. One year prior, the lesion spontaneously ulcerated, leading to recurrent bleeding. On examination, we observed a well-defined erythematous to skin-colored annular plaque with a thread-like margin, measuring 5 × 3 cm, on the upper lip. The plaque featured a single ulcer ,as shown in Figure 1, measuring 1 × 1 cm, with sloping edges and a floor containing slough and hemorrhagic crusts [Figure 1a]. A histopathological examination was performed to confirm the diagnosis and rule out malignancy. The examination revealed hyperkeratosis with microabscess formation by polymorphonuclear leukocytes, diminished Malpighian layer, hydropic degeneration of basal keratinocytes, and a dermal perivascular lymphocytic infiltrate. Clusters of necrotic keratinocytes were noted, but no malignant changes were observed [Figure 2].
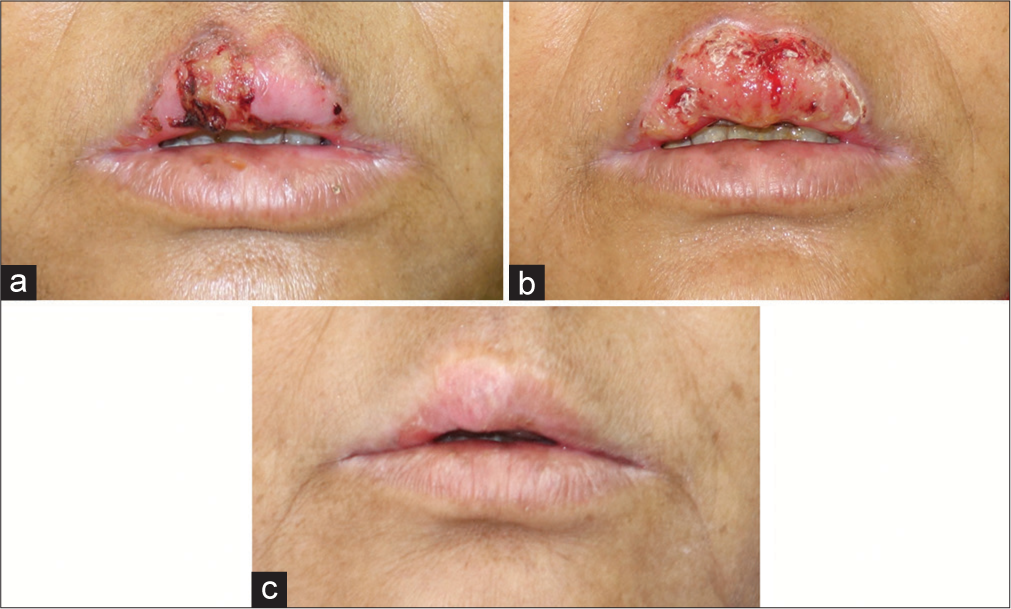
- (a) Solitary plaque with prominent thread-like margins associated with ulceration seen over the upper lip. (b) Lesion 2 weeks after first sitting of CO2 laser ablation. (c) Lesion after complete healing, at 2 months after the second sitting.
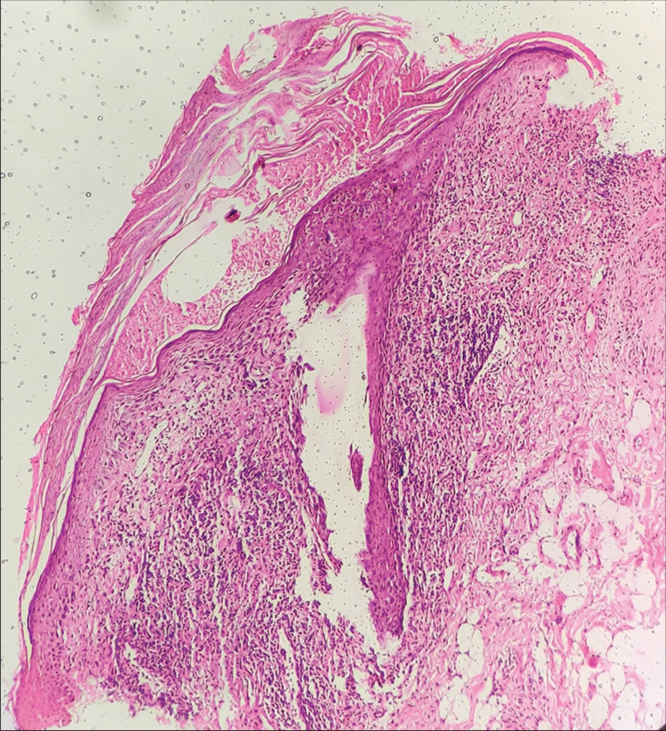
- Hyperkeratosis with microabscess formation, diminished malpighian layer, basal layer degeneration, and dermal lymphocytic infiltration (H&E, × 40). H&E: Hematoxylin and eosin.
The lesion was treated with CO2 laser ablation over two sessions, spaced 1 month apart. A 30W CO2 laser machine in continuous mode at 4W power was used for each session. Post-procedure healing required 2 weeks with the administration of antibiotics and anti-inflammatory drugs [Figure 1b]. Complete resolution was observed after the second session, with no recurrence during a 9-month follow-up [Figure 1c].
DISCUSSION
PK of Mibelli is typically seen in children and follows an autosomal dominant inheritance pattern.2 Labial PK is an exceptionally rare subtype of PK of Mibelli, with only a limited number of cases reported in the literature.3 Treatment modalities for PK include topical agents such as 5-fluorouracil and imiquimod, cryotherapy, photodynamic therapy, dermabrasion, and excision.2 CO2 laser ablation has shown promising results for PK at various sites.4
Carbon dioxide laser treatments have been widely employed across various types of PK, with numerous studies reporting positive outcomes. Clinical results have shown low recurrence rates and notably favorable cosmetic improvements in disseminated superficial actinic porokeratosis (DSAP), porokeratosis of Mibelli (PM), and reticulate porokeratosis.4-6 In the context of labial PK, a combination of cryotherapy and carbon dioxide laser therapy has demonstrated beneficial effects.3 In addition, a combined approach involving methyl aminolevulinate-photodynamic therapy alongside carbon dioxide laser therapy has resulted in marked clinical enhancements.7 Conversely, less satisfactory outcomes were documented in cases of PM, DSAP, and PK ptychotropica.8-10 Furthermore, among four patients with genital PK, approximately 50% exhibited complete lesion healing during follow-up periods extending up to 13 years.11
CONCLUSION
In this report, we have described a case of isolated labial PK successfully treated with CO2 laser ablation, an innovative approach for a rare presentation of mucocutaneous PK. The patient achieved excellent esthetic results with no recurrence during a 9-month follow-up period. This case underscores the potential effectiveness of CO2 laser ablation in managing labial PK and warrants further investigation in a larger patient cohort.
Authors’ Contributions
Yogesh M. Bhingradia, Arshi Farista, Vikas Ganesh Solanki, Mriganka Mehra have contributed to the research. Tasks such as Concepts, Design, Literature Search, Clinical Studies, Experimental studies, Data acquisition, Data analysis, Statistical analysis, Manuscript preparation, Manuscript editing, and Manuscript review are equally taken care of by all the authors. All authors are the Guarantors as well.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Porokeratosis: An enigma beginning to unravel. Indian J Dermatol Venereol Leprol. 2022;88:291-9.
- [CrossRef] [PubMed] [Google Scholar]
- Porokeratosis-head to toe: An unusual presentation. Indian Dermatol Online J. 2015;6:101-4.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of porokeratosis of Mibelli with CO2 laser vaporization versus surgical excision with split-thickness skin graft. A comparison. J Dermatol Surg Oncol. 1993;19:199-202.
- [CrossRef] [PubMed] [Google Scholar]
- Split-face trial of CO2 laser-induced ring abrasion and high-dose tacalcitol in the treatment of disseminated superficial actinic porokeratosis. J Dermatol. 2012;39:879-80.
- [CrossRef] [PubMed] [Google Scholar]
- Reticulate porokeratosis: Successful treatment with CO2-laser vaporization. Clin Exp Dermatol. 1992;17:178-81.
- [CrossRef] [PubMed] [Google Scholar]
- Photodynamic therapy combined with CO2 laser vaporization on disseminated superficial actinic porokeratosis: A report of 2 cases on the face. Ann Dermatol. 2011;23(Suppl 2):S211-3.
- [CrossRef] [PubMed] [Google Scholar]
- Porokeratosis of mibelli: Rapid recurrence of a large lesion after carbon dioxide laser treatment. Pediatr Dermatol. 1994;11:267-70.
- [CrossRef] [PubMed] [Google Scholar]
- Successful treatment of disseminated superficial actinic porokeratosis with Q-switched ruby laser. J Dermatol. 2007;34:816-20.
- [CrossRef] [PubMed] [Google Scholar]
- A rare variant of porokeratosis: Porokeratosis ptychotropica. J Am Acad Dermatol. 2006;55(5 Suppl):S120-2.
- [CrossRef] [PubMed] [Google Scholar]
- Genital porokeratosis: A series of 10 patients and review of the literature. Br J Dermatol. 2006;155:325-9.
- [CrossRef] [PubMed] [Google Scholar]




