
Translate this page into:
A Therapeutic Trial Comparing Modified Autoinoculation, a Novel Approach with Topical Potassium Hydroxide Application in the Treatment of Molluscum Contagiosum
Address for correspondence: Dr. Leena Raveendra, Department of Dermatology, Venereology & Leprosy, RajaRajeswari Medical College & Hospital, Kambipura, Mysore Road, Bangalore 560074, Karnataka, India. E-mail: cbleena@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Context:
Molluscum contagiosum (MC) is a common viral cutaneous infection. Despite multiple treatment options, there is no definitive treatment. In some cases, the lesions are severe, recurrent, and cosmetically odd. Modified autoinoculation (MAI) is a novel technique that induces cell-mediated immunity resulting in clearance of local as well as distant lesions. Potassium hydroxide (KOH) acts by dissolving the keratin and penetrating deeply destroys the hyperproliferative tissue. We would here like to compare MAI with topical KOH in the treatment of MC.
Aims and Objective:
The aim of this study was to assess the effectiveness of MAI in treatment of MC and to compare its response with topical KOH application.
Settings and Design:
This was an open-labeled longitudinal therapeutic outcome study carried out at a tertiary care center over a period of 1 year.
Materials and Methods:
Hundred consenting MC patients attending the department of dermatology were randomized into Group A and Group B. Group A patients were subjected to MAI and Group B to topical application of 10% KOH.
Statistical Analysis Used:
The continuous variables are presented as mean ± standard deviation (SD). The difference between the mean score was analyzed using Student’s t test for independent variable and paired t test for paired results.
Results:
At the end of 16 weeks, 91.48% showed complete clearance by MAI compared to 81.64% with topical 10% KOH solution. There was a significant reduction of mean score of lesions in patients treated by MAI compared to patients treated with KOH.
Conclusion:
MAI therapy provides a promising, easy, cost-effective, daycare option for MC infections.
Keywords
Modified autoinoculation
molluscum contagiosum
potassium hydroxide
Modified autoinoculation therapy is a promising treatment option in treating severe, recurrent, extensive, and recalcitrant molluscum contagiosum infections. Modified autoinoculation is a safe, highly effective, and immune-stimulating mode of therapy that can cause resolution of lesions at distant sites also.

INTRODUCTION
Molluscum contagiosum (MC) is a cutaneous infection that is commonly seen in children and young adults.[12] Treatment options available are ablative or immunomodulatory in nature. Destructive modalities are not practical when lesions are extensive and in children. Recurrence of lesions is also an issue.[3] Autoinoculation helps to trigger a cell-mediated immune response to the antigen helping to clear local as well as distant lesions.[3] Our study aimed to assess the effectiveness of modified autoinoculation (MAI) in treatment of MC and to compare the treatment response with topical potassium hydroxide (KOH) application, which is a well-established treatment. There are various randomized controlled studies, systematic reviews, and meta-analysis proving the efficacy of KOH in the treatment of MC.[45678]
SUBJECTS AND METHODS
This study was an open-labeled longitudinal randomized therapeutic study carried out at the department of dermatology in a tertiary care referral hospital. The study was conducted for 1 year between January 2019 and December 2019, after obtaining the institutional ethics committee clearance. Treatment naïve patients above 5 years of age with ≥5 lesions and with a treatment-free washout period of at least 1 month were included in the study. Immunocompromised patients or patients on immunomodulatory or immunosuppressive drugs, pregnant women/lactating mothers were excluded. Total patients screened were 136 of which 36 patients were excluded as they did not fit the inclusion and exclusion criteria. These 100 consenting patients clinically diagnosed with MC satisfying the inclusion and exclusion criteria were randomized into two groups, Group A and Group B using simple random sampling technique [Figure 1]. Both groups were age and sex matched.
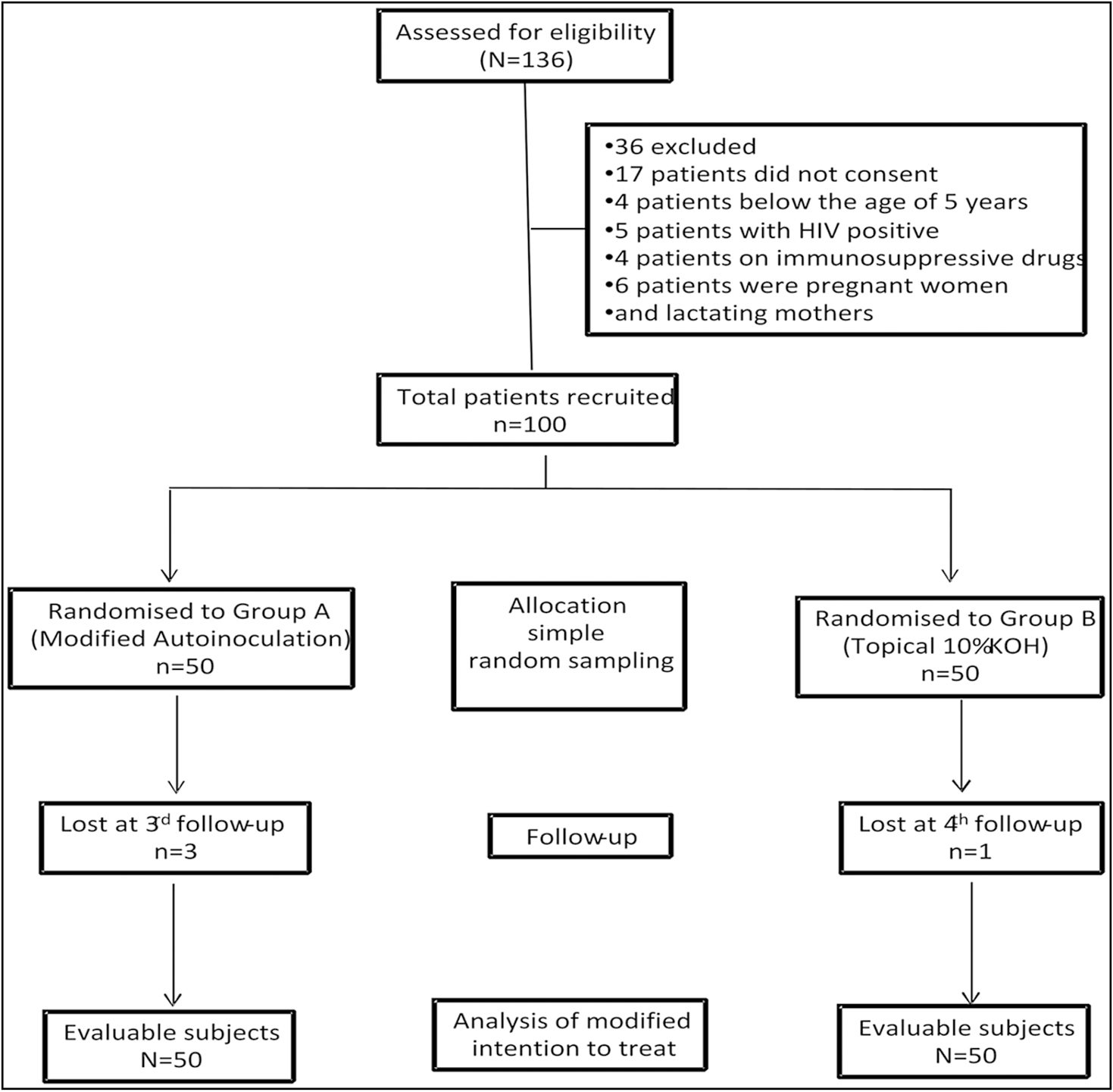
- Flow chart of the progress of study through various phases
Group A––50 patients with MC were subjected to MAI.
Group B––50 patients with MC were subjected to topical application of 10% KOH.
Detailed history, clinical examination, and clinical photographs of all the patients were taken.
Group A: The procedure was performed in the dermatology minor operation theatre. A well-developed lesion was chosen as a donor. Under topical anesthesia, and using all aseptic precautions, an insulin syringe was used to puncture 8–10 times along all the axis and planes of the lesion to direct the contents of the molluscum body into the dermis resulting in multiple bleeding points from the site of entry [Figure 2A and B]. To enhance a successful exposure of viral antigens to the immunological surveillance system, a mild compression by rotatory movements with a cotton swab was done [Figure 2C].
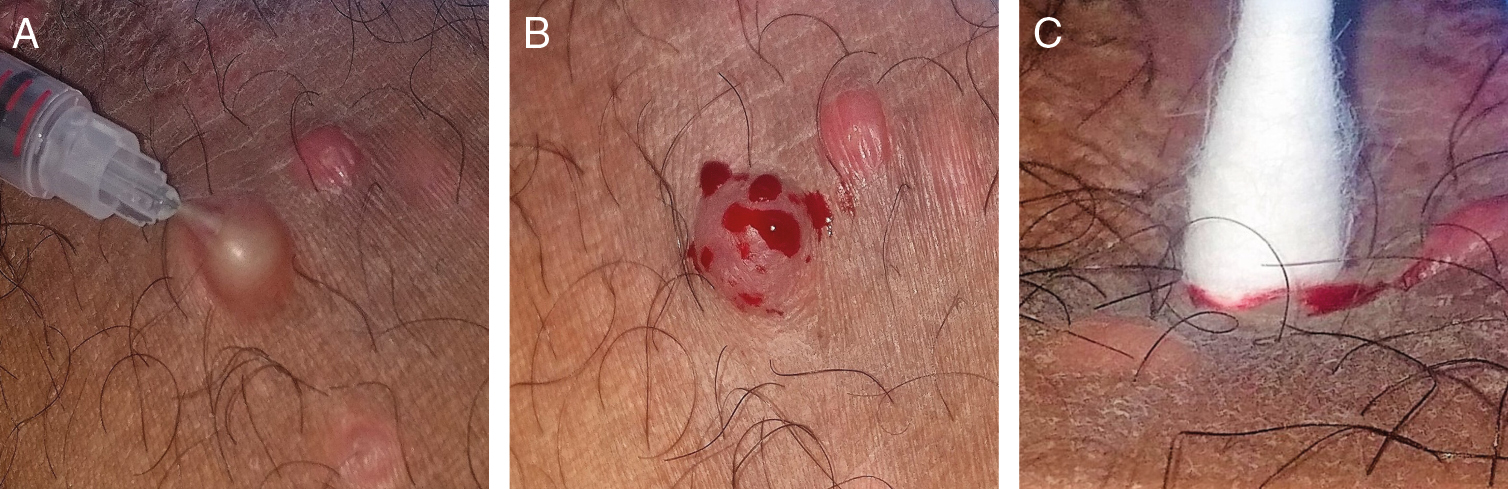
- (A) An insulin syringe used to puncture MC lesion deep into the dermis, along all the axes and planes of a fully developed lesion. (B) Multiple bleeding points from the site of entry. (C) A mild compression by rotatory movements with a cotton swab
After the procedure, mupirocin cream 2% was applied locally over the punctured site for 5 days to prevent any secondary bacterial infection. Patients were advised to avoid taking any anti-inflammatory medications for 72 h to increase the likelihood of a successful controlled inflammatory response. If there was an inadequate response (less than 10% reduction in number) after second follow-up at week 2, the procedure was repeated.
Group B: Patients or their parents were advised to apply KOH (10%) solution daily at night on all the lesions with a toothpick after covering the surrounding area with petrolatum to avoid any spillage, and wash it off in the morning. It was advised to wash off immediately if there was redness or irritation or if there was any accidental spillage. Application was continued till the lesions showed signs of inflammation or superficial erosions or up to a maximum of 16 weeks.
Subjects of both the groups were asked to follow-up to assess the reduction in number of lesions on 1st, 2nd, 4th, 8th, 12th weeks, and last assessment was on the 16th week.
All the data were entered in the Excel sheet and demographic details were represented as frequency and percentage. The continuous variables are presented as mean ± standard deviation (SD). The difference between the mean score was analyzed using Student’s t test for independent variable and paired t test for paired results. Data were analyzed using the Statistical Package for the Social Sciences (SPSS) software program, version 23.0 for Windows.
RESULTS
A total of 100 patients were included in the study after fulfilling the inclusion and exclusion criteria. Three patients among Group A and 1 patient among Group B were lost to follow up in the study. The mean age (Group A = 22.6 ± 10.3, Group B = 22.72 ± 10.42, P = 0.954) and the mean number of the lesions at baseline (Group A = 32.1 ± 15.8, Group B = 27.68 ± 15.34, P = 0.159) were statistically insignificant between the groups at the initiation of treatment. In this study, 42 cases were females and 58 cases were males with male-to-female ratio of 1.4:1.
The mean lesion count decreased from 27.1± 14.54 at first follow-up to 0.32 ± 1.2 at the end of 16 weeks in patients treated with MAI in Group A [Table 1]. The number of lesions at any juncture during the follow-up was compared using paired t test. The comparison between the number of lesions at baseline (Week 0) and the number of lesions at 16 weeks were found to be statistically significant (P < 0.001) in Group A patients [Table 1].
| Modified autoinoculation method Mean ± SD | Topical potassium hydroxide Mean ± SD | P Value | |
|---|---|---|---|
| Week 1 follow-up | 27.1 ± 14.54 | 24.84 ± 14.46 | . 439(NS) |
| Week 2 follow-up | 17.56 ± 11.64 | 19.86 ± 12.49 | .352(NS) |
| Week 4 follow-up | 7.34 ± 7.23 | 11.84 ± 9.11 | .009** |
| Week 8 follow-up | 2.21 ± 3.9 | 5.45 ± 5.68 | .002** |
| Week 12 follow-up | 0.64 ± 1.81 | 1.81 ± 4.14 | .042* |
| Week 16 follow-up | 0.32 ± 1.2 | 1.41 ± 3.81 | .01* |
NS = nonsignificant
*P <0.05 is statistically significant
**Highly significant
The mean lesion count decreased from 24.84 ± 14.46 at first follow-up to 1.41 ± 3.81 at the end of 16 weeks of follow-up in patients treated with topical 10% KOH solution application in Group B [Table 1]. The number of lesions at any juncture during the follow-up was compared using paired t test. The comparison between the number of lesions at baseline (Week 0) and the number of lesions at 16 weeks was found to be statistically significant (P < 0.001) in Group B patients [Table 1].
The number of lesion clearance at various junctures was compared between Group A and Group B. The difference between the number of lesions at various points in time between the two groups was statistically significant (P < 0.001), except at week 0, week 1, and week 2 [Table 1]. The mean lesion score in Group A was significantly lower than the Group B patients at every follow-up after 2 weeks of treatment [Figure 3].
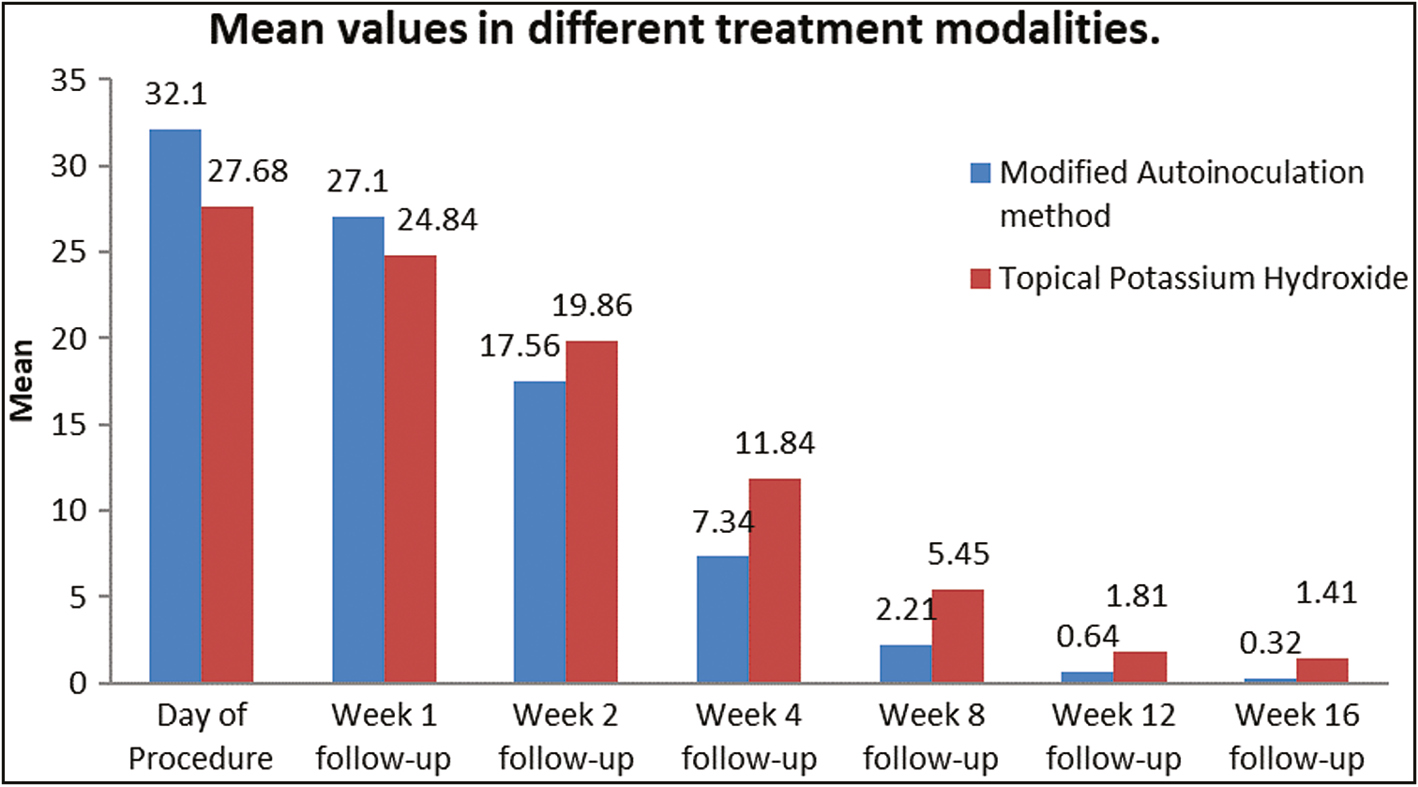
- Graph depicting average number of lesions among both the groups, on follow-up
The complete resolution of the MC in patients at 12th week was seen in 39 (82.97%) patients in MAI group and 34 (69.4%) in KOH group. The same at 16th week follow-up was 43 (91.48%) in MAI and 40 (81.64%) in KOH group. When compared by chi-square test there was no statistically significant difference in complete clearance in patients at 12th and 16th weeks of follow-up when both the treatment modalities were compared. There was a statistically significant response at the 8th week of follow-up [Table 2].
| Method | Week 4 | Week 8 | Week 12 | Week 16 |
|---|---|---|---|---|
| Modified autoinoculation method (n = 47) | 15(31.91%) | 30(63.82%) | 39(82.97%) | 43(91.48%) |
| Topical potassium hydroxide (n = 49) | 8(16.33%) | 17(34.70%) | 34(69.40%) | 40(81.64%) |
| P Value | 0.082797(NS) | 0.005617* | 0.160605(NS) | 0.231536(NS) |
NS = nonsignificant
*P < 0.005 is highly significant
Of the 50 patients who received 10% KOH, 20 (40%) showed adverse effects, whereas of the 50 patients who received the MAI method, 8 (16%) showed adverse effects. Of the patients on KOH, erythema was seen in 12 patients (24%), contact allergy and post-inflammatory hyperpigmentation was seen in 4 patients each (8%) and among patients of MAI, 5 (10%) had pain, 2 (4%) had scarring and 1 (2%) had post-inflammatory hyperpigmentation.
DISCUSSION
MC is a cutaneous infection caused by molluscum contagiosum virus (MCV) that is part of the family poxviridae with four serotypes.[12] It is transmitted through direct contact, indirectly via fomites, and by sexual contact as well.[3]
The infection with the molluscum virus is confined to the epidermal layers and remains inconspicuous to the immune reconnaissance. It forms a complex hyperproliferative lesion with an abundance of viral particles, as a characteristic inclusion body known as Henderson–Paterson body. The virus evades immune detection by not entering the basal membrane.[910] Inflammatory reaction is known to be induced if the contents of the molluscum papule are introduced into the dermis.[2]
MC is self-limiting without treatment. Treatment options available are either ablative or immunomodulatory in nature. They include mechanical destruction with curettage, cryotherapy, electrodessication, photodynamic therapy, and laser ablation.[3] Chemical destruction of MC can be achieved by treatment with KOH, liquid phenol, salicylic acid, glycolic acid, trichloroacetic acid, tretinoin, tazarotene, and cantharidin.[36,10] Immunomodulatory agents like imiquimod, interferon-alpha, antiviral agents like cidofovir, immunotherapy with candida antigen, and more recently autoinoculation for multiple lesions and recurrent lesions have been tried.[37,810]
Potent keratolytic like KOH is proven to be safe and efficacious in various studies.[611] It desquamates and destroys the hyperproliferative tissue by dissolving the keratin. It is inexpensive, easy-to-apply and it has an added benefit of being relatively painless.[811]
Autoinoculation is a technique that helps to trigger a cell-mediated immune response to the antigen helping to clear local as well as distant lesions. In the conventional method of autoimplantation, a distant donor lesion is curetted for a substantial amount of waxy material, crushed, and introduced into a pocket extending to the deep dermis in volar aspect of the forearm.[3] Kachhawa et al.[9] modified the autoinoculation method by adapting a single donor-recipient lesion in the treatment of MC. MAI is a newer simpler technique and this technique was further modified by multiple piercings and mild compressions of the lesion in our study.
MAI is a safe, highly effective, and immune-stimulating mode of therapy. This work has opened a new era of therapy that needs no repetitive application of corrosive chemicals or tissue destroying ablative procedures. Autoinoculation can cause resolution of lesions at distant sites also.[12] Specific autoimplantation studies done previously on warts have shown to be associated with the development of Th1 cytokines (TNF-α and IL-1) that down-regulate gene transcription. Also INF-γ and IL-2 are known to activate cytotoxic T cells and natural killer cells to remove the cells infected with human papillomavirus.[13] Same immune response is to be expected in MC which is a similar viral entity both clinically and immunologically.[3] Cell-mediated immunity is known to have a major role in controlling and elimination of the MC infection.[2]
In our study, MAI has shown higher rates of resolution with shorter treatment time and mild side effects compared to studies by Gupta et al.[3] and Kachhawa et al.[9] In our study 82.97% clearance was achieved at the end of 12 weeks. Gupta et al.[3] using conventional method of autoinoculation have achieved a complete clearance of 68.2% at the end of 12 weeks. Kachhawa et al.[9] chose a well-developed lesion as a donor and did autoinoculation by few punctures along the plane of skin and introduced it to dermis to obtain a complete clearance by 55.17% at 12th-week follow-up.
In the study by Maluki et al.[10] MC lesions responded to pricking with a 27-guage needle alone in 75% of patients. This result was achieved after three sessions of pricking the lesion with the needle 1 week apart. It has been reported that pricking the lesions stimulated the immune system by releasing cytokines and other immune factors which promote the attraction of T cells which can clear the MC lesions.
In this study, we modified the method of Kachhawa et al. by making multiple punctures along different planes and by a mild push for adequate dermal inoculation and thus obtained 82.97% and 91.48% complete clearance at the end of 12th and 16th weeks, respectively.
In Group B where KOH was used, complete clearance of lesions was seen in 69.4% of patients in our study compared to 42.1% in the study by Metkar et al. and 85% by Chathra et al. at the end of 12 weeks. Metkar et al. and Chathra et al. compared 10% KOH with 5% imiquimod to obtain an equal and a twofold better response with KOH, respectively. In both studies, KOH showed a faster onset of action than imiquimod but a higher incidence of side effects.[811]
In our study, we found that both MAI and conventional therapy with 10% KOH are effective in the treatment of MC [Figures 4 and 5]. However, there was a significant difference in their efficacies, with MAI being a better treatment option when the lesion count was considered. Faster clearance of the lesions was achieved by autoinoculation compared to 10% KOH. When complete clearance of the lesions in patients was considered, both modalities showed similar response except at 8 weeks of follow-up when autoinoculation was found better. Also, there was no influence of age and sex on the outcome, as in our study age and sex were matched. Also, there was no significant strength of association between variables with follow-up of variables using Spearman correlation
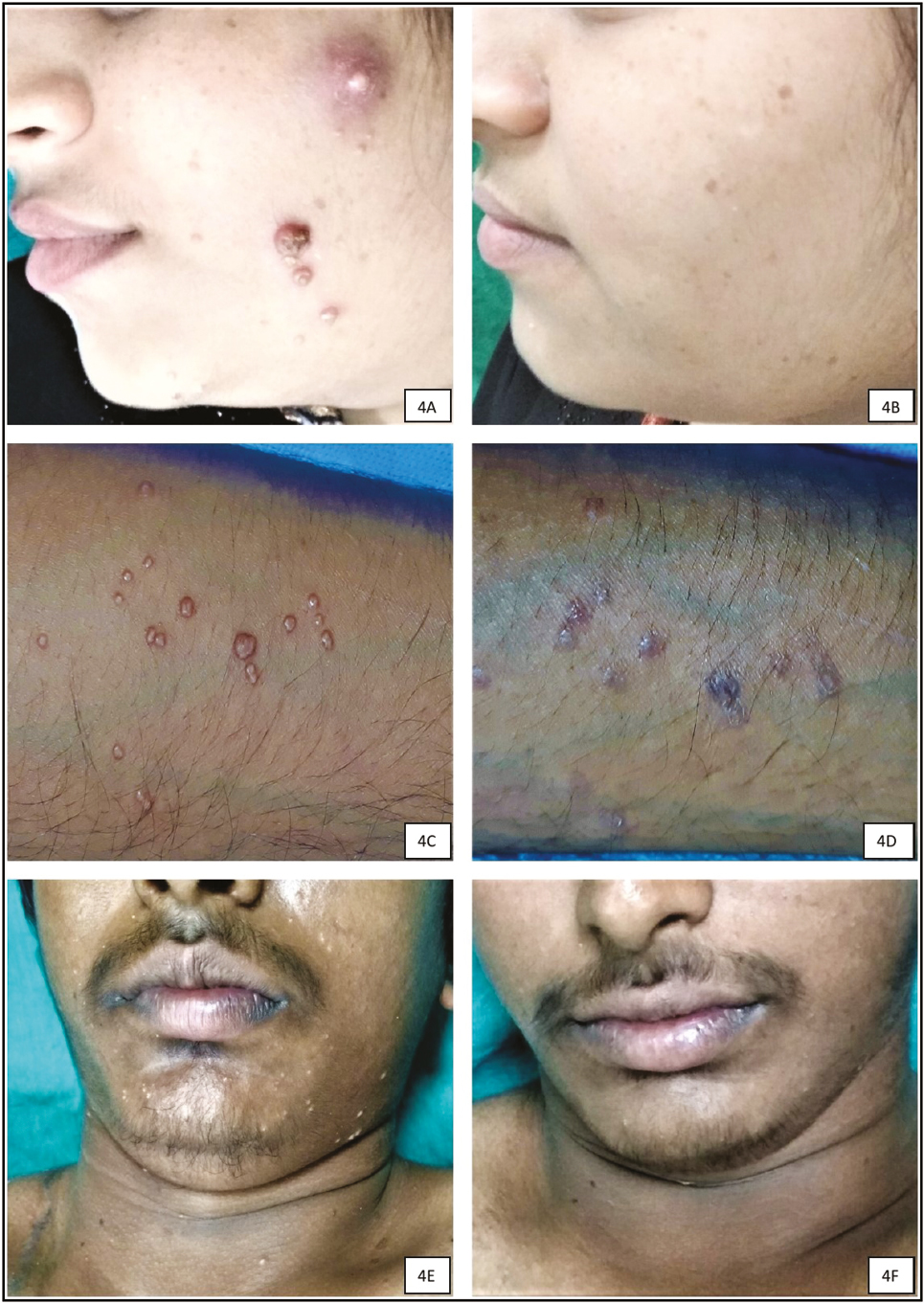
- Responses to modified autoinoculation on day 0 (A, C, and E) and complete resolution at the end of 16th week (B, D, and F) follow-up

- Responses to topical potassium hydroxide on day 0 (A, C, and E) and complete resolution at the end of 16th week (B, D, and F) follow-up
The local adverse reactions related to MAI were seen in 16% of patients and included pain, scarring, and post-inflammatory hyperpigmentation. Similar adverse effects were reported by Gupta et al.[3] in 50% of their patients disappeared in 3–5 days. Kachhawa et al.[9] reported skin irritation, redness, and pain at the site of autoimplantation in their study.
One more point to note is that most of the MC lesions resolve spontaneously within 24–36 weeks.[2] The mean of initial duration of lesions in both the groups was 28 (range: 6–40) and 31 (range: 8–37) weeks, respectively. Therefore, the natural course of the disease may be a possible confounding factor in our study. MAI may be combined safely with the other modalities like topical tretinoin or 10% KOH applied on uninoculated lesions for early resolution of lesions the results of which can be analyzed with further studies.
In our study, the adverse reaction to the treatment was higher among the patients treated with 10% KOH (40%) compared to MAI. Other studies have reported adverse effects in 40%, 50%, and 78.9% of patients while using KOH.[68,11] The most common adverse effect observed was erythema at the site of application in our study. In other studies, side effects noted were erythema, crusting, hyperpigmentation, hypopigmentation, and local irritation.[68,11]
CONCLUSION
MAI therapy is a novel, simple, daycare, and cost-effective procedure, emerging as a promising treatment option in treating severe, recurrent, extensive, and recalcitrant MC infections.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- UK national guideline for the management of genital molluscum in adults, 2014 clinical effectiveness group, British Association for Sexual Health and HIV. Int J STD AIDS. 2015;26:687-95.
- [Google Scholar]
- Viral infections. In: Grifftiths C, Barker J, Bleiker T, Chalmers R, Creamer D, eds. Rook’s textbook of dermatology (9th ed). Oxford: Wiley-Blackwell; 2016. p. :25.12-25.14.
- [Google Scholar]
- Autoimplantation therapy for the management of extensive molluscum contagiosum: A novel treatment approach. Int J Res Med Sci. 2016;4:1392-6.
- [Google Scholar]
- The efficacy and safety of topical 10% potassium hydroxide for molluscum contagiosum: A systematic review and meta-analysis. J Dermatolog Treat 2021 doi: 10.1080/09546634.2021.1898527. Online ahead of print
- [Google Scholar]
- Randomized placebo-controlled clinical trial on efficacy and safety of topical 10% Potassium hydroxide for molluscum contagiosum treatment in children. J Dermatolog Treat. 2019;30:750-6.
- [Google Scholar]
- An open, randomized, comparative clinical and histological study of imiquimod 5% cream versus 10% potassium hydroxide solution in the treatment of molluscum contagiosum. Ann Dermatol. 2010;22:156-62.
- [Google Scholar]
- Treatment of molluscum contagiosum in adult, pediatric, and immunodeficient populations. J Cutan Med Surg. 2014;18:299-306.
- [Google Scholar]
- A comparative study of 10% KOH solution and 5% imiquimod cream for the treatment of molluscum contagiosum in the pediatric age group. Indian Dermatol Online J. 2015;6:75-80.
- [Google Scholar]
- Autoinoculation as a treatment modality for molluscum contagiosum: a preliminary uncontrolled trial. Indian J Dermatol Venereol Leprol. 2018;84:76-8.
- [Google Scholar]
- Treatment of molluscum contagiosum by potassium hydroxide solution 20% with and without pricking and by pricking alone: a comparative study with review of literature. Int J Dermatol Clin Res. 2015;1:31-41.
- [Google Scholar]
- An open, nonrandomized, comparative study of imiquimod 5% cream versus 10% potassium hydroxide solution in the treatment of molluscum contagiosum. Indian J Dermatol Venereol Leprol. 2008;74:614-8.
- [Google Scholar]
- Autowart injection therapy for recalcitrant warts. Indian J Dermatol. 2010;55:367-9.
- [Google Scholar]
- Safety and effectiveness of autoinoculation therapy in cutaneous warts: a double–blind, randomized, placebo–controlled study. Indian J Dermatol Venereol Leprol. 2014;80:515-20.
- [Google Scholar]




