
Translate this page into:
Accessory tragus on the nasal vestibule: A rare case report with literature review
 , Sara M. Mohy2, Sameh Fawzy Fahmy Mohamed1, Mohamed S. Hasan1, Mofreh Mansour3, Mohamed El-Khalawany1
, Sara M. Mohy2, Sameh Fawzy Fahmy Mohamed1, Mohamed S. Hasan1, Mofreh Mansour3, Mohamed El-Khalawany1
*Corresponding author: Mahmoud A. Rageh, Department of Dermatology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt. dr.mahmoudrageh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rageh MA, Mohy SM, Mohamed SFF, Hasan MS, Mansour M, El-Khalawany M. Accessory tragus on the nasal vestibule: A rare case report with literature review. J Cutan Aesthet Surg. doi: 10.25259/jcas_69_24
Dear Editor,
Accessory tragus (AT) is a congenital pedunculated or sessile, skin-colored papule or nodule, most often unilateral and solitary. The papule size is usually 3–5 mm and might be covered with vellus hair. Diagnosis is based on the age of onset, the clinical appearance of the lesion, and the characteristic anatomical location anterior to the tragus. However, uncommonly, accessory tragi may appear at unusual sites.1,2
A 21-year-old male presented with a solitary, roughly spherical, 6 × 4 mm, soft, and skin-colored mass with a short pedicle located on the left nasal vestibule since birth [Figure 1a]. There was no history of consanguinity nor family history of similar cases. The patient was otherwise healthy without any system abnormalities. The patient wanted to remove the lesion for cosmetic purposes; however, he refused complete surgical excision, so the lesion was shaved by a scalpel, followed by cauterization of the base [Figure 1b], and then sent for histopathologic examination that revealed undulated epidermis with basket-weave hyperkeratosis, mild papillomatosis, and focal increase in basal melanin. The dermis showed loose collagen bundles and fat lobules occupying the central core [Figure 1c]. Based on history and clinicopathological findings, the diagnosis was AT.
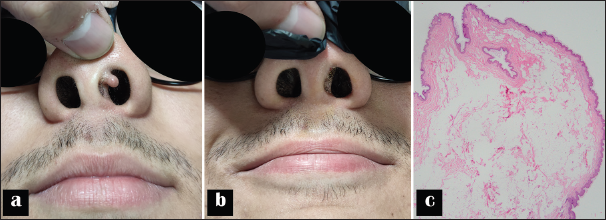
- (a) Clinical appearance of accessory tragus on the left nasal vestibule in the form of a solitary, soft, and skin-colored nodule, (b) immediately after the lesion was shaved and the base was cauterized, and (c) histopathology of the excised specimen showing surface epithelium and a dermal core of numerous fat lobules and loose collagen bundles (hematoxylin and eosin, × 4).
AT is a malformation that almost exclusively is located in areas derived from branchial arches, most commonly the preauricular area. Less common locations of AT include the cheek in an area extending along an imaginary line drawn from the angle of the mouth to the ear, as well as the lateral neck anterior to the sternocleidomastoid muscle.1
Embryologically, the auricle develops from the first and second branchial arches in the 4th week of gestation. During the 5th and 6th weeks, the first and second arches form six mesenchymal tubercles, the hillocks of His. Three hillocks appear on each arch, and as they develop, they fuse to form the structures of the auricle. As the mandible grows, the primitive auricle ascends from the lower lateral neck to the side of the head level with the eyes. For this reason, AT is generally detected near the tragus but rarely on the cheek, the lateral neck along the anterior edge of the sternocleidomastoid muscle, or the glabella or the suprasternal area.3
Outside these predilection areas, accessory tragi are rarely encountered in the skin. Only three previous cases were located on the nasal vestibule,2-4, and they were summarized in Table 1.
| Author | Year | Age/Sex | Duration | Number | Location | Clinical presentation | Associations or other anomalies | Treatment |
|---|---|---|---|---|---|---|---|---|
| Shin et al.3 | 2010 | A 1-day-old girl | Since birth | Single | The left nasal vestibule | Soft, skin-colored mass with an ovoid pedicle that was about 8×8 × 8 mm in size | None | Completely removed by adequate excision. |
| Moradi et al.2 | 2020 | A 3-month-old boy | Since birth | Single | The left nostril rim | A 6 mm pedunculated skin tag. The lesion appeared to have had another portion that auto-amputated. | Not reported | The lesion was removed surgically. |
| Bandaranayake et al.4 | 2021 | A 3-week-old female baby | Since birth | Multiple (2 lesions) | One lesion was on the right nasal vestibule, while the other was on the tip of the nose. | Spherical, soft, skin-colored mass with a short pedicle. The larger lesion measured about 10×5 mm in size. | None | Both lesions were completely excised. |
There are a few reports of familial AT.3 It is usually an isolated developmental defect not associated with other abnormalities. However, AT may rarely be associated with other genetic syndromes such as Wolf-Hirschhorn, Treacher-Collins, vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities (VACTERL), Goldenhar, and Townes-Brooks. In addition, it can also be associated with hearing impairment and renal abnormalities such as horseshoe kidney and hydronephrosis.5
Biopsy findings have shown a sessile or pedunculated polyp, including multiple small hair follicles, fibrovascular tissue with fat lobules, a central core of cartilage, and a prominent connective tissue framework.3 These are the typical diagnostic clues for AT. Our case is distinctive because we report an AT developed on the nasal vestibule. Furthermore, cartilage could not be identified histopathologically in our case by examining serial sections, which is not necessarily uncommon in cases of AT.6
Management includes complete lesion excision with relevant investigations to rule out other congenital abnormalities.4 In our case, the lesion healed perfectly with no evidence of recurrence at a 6-month follow-up visit.
Authors’ contributions
Mahmoud A. Rageh and Sara M. Mohy contributed to the concept, data collection, drafting and critical revision of the article. The remaining authors contributed to analysis and interpretation. All authors approved the final version to be published.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Accessory auricle: Classification according to location, protrusion pattern, and body shape. Arch Plast Surg. 2018;45:411-7.
- [CrossRef] [PubMed] [Google Scholar]
- Accessory tragus: Report of a case in a rare location on the nasal vestibule. Pediatr Dermatol. 2020;37:383-4.
- [CrossRef] [PubMed] [Google Scholar]
- A case of accessory tragus on the nasal vestibule. Ann Dermatol. 2010;22:61-2.
- [CrossRef] [PubMed] [Google Scholar]
- A rare case of accessory tragi in the nose. Ceylon J Otolaryngol. 2021;10:48-50.
- [CrossRef] [Google Scholar]
- Review of accessory tragus with highlights of its associated syndromes. Int J Dermatol. 2014;53:1442-6.
- [CrossRef] [PubMed] [Google Scholar]
- Histological diagnostic criteria for accessory tragi. J Cutan Pathol. 1990;17:206-10.
- [CrossRef] [PubMed] [Google Scholar]




