
Translate this page into:
Achieving esthetic improvement in a rare case of facial blaschko-linear lichen planus using 1064 nm Q-switched neodymium: Yttrium-aluminium-garnet laser and microneedling pen
*Corresponding author: Shruthi Pavana Janardhanan, Everything Skin and Hair Medical and Aesthetic Dermatology Clinic, Mumbai, Maharashtra, India. shruthjan@yahoo.com.sg
-
Received: ,
Accepted: ,
How to cite this article: Saraogi P, Janardhanan SP. Achieving esthetic improvement in a rare case of facial Blaschko-linear lichen planus using 1064 nm Q-switched neodymium: Yttrium-aluminium-garnet laser and microneedling pen. J Cutan Aesthet Surg. doi: 10.25259/JCAS_50_2024
Abstract
Lichen planus (LP) affects between 0.5 and 1% of the population. Linear LP accounts for <0.2% of LP cases. Linear LP of the face is even rarer, with only a handful of cases. Linear facial LP follows Blaschko’s lines, usually along the mandible, has follicular localization and leaves long-standing pigmentation and atrophy. There is a paucity of data for the treatment of LP esthetic sequelae, more so for facial linear LP in darker skin types with atrophy. Most treatments are attempted to stabilize the spreading of the disease and limit its progression but do not successfully address esthetic pigmentation and atrophy. Our case is an Indian woman with isolated facial linear LP clinically who was successfully treated for esthetic sequelae with 1064 nm Q-switched neodymium: Yttrium-aluminiumgarnet laser and microneedling pen without relapse even after 1 year.
Keywords
Atrophy
Facial Blaschko-Linear lichen planus
Microneedling
Pigmentation
Q-switched neodymium: Yttrium-aluminium-garnet laser

INTRODUCTION
Facial Linear Lichen Planus (LP) along Blaschko’s lines is a rare variant of classical LP, with a paucity of data on its treatment.1 Most available treatments restrict the disease spread but do not effectively address the residual pigmentation and atrophy especially in darker skin types. We report a case of Blaschko-linear facial LP in an Indian female who was successfully treated with Q-switched neodymium-doped yttrium aluminum garnet (QSNY) laser and microneedling to address the residual hyperpigmentation and atrophy, without any relapse 1 year post-treatment completion.
CASE REPORT
A 52-year-old healthy Indian female (Fitzpatrick skin-type IV) presented with a 6-month history of unilateral asymptomatic dark brown macules on the right angle of the lip, which quickly progressed along the right underside of the mandible following a Blaschko line [Figure 1]. There were areas of atrophy and follicular plugging on the chin. There was no history of trauma, topical application, excessive sun exposure, photosensitivity, or drug intake up to 6 months before onset. Dermoscopy revealed an erythematous to violaceous background “peppered” with brown dots and globules and accentuated pigment pseudo-network [Figure 2]. She refused a biopsy, fearing a scar, considering her main concern was cosmetic disfigurement restricting her from social activities (dermatology life quality index [DLQI] – score 20). The rest of the skin, scalp, oral and genital mucosa, and nails were normal. The patient had no other medical comorbidities, and routine blood investigations were within normal limits. Antinuclear antibody (ANA) and double-stranded DNA (dsDNA) were negative and ruled out linear discoid lupus erythematosus (DLE) of the Lupus erythematosus (LE) spectrum. A clinical diagnosis of linear LP of the face was made based on the pigmented character, mandibular topography, blaschkoid distribution, atrophic progression, and dermoscopic features.1

- Clinical photograph before treatment: Dark gray-brown hyperpigmented macules extending along the mandible with some areas of atrophy and follicular plugging.
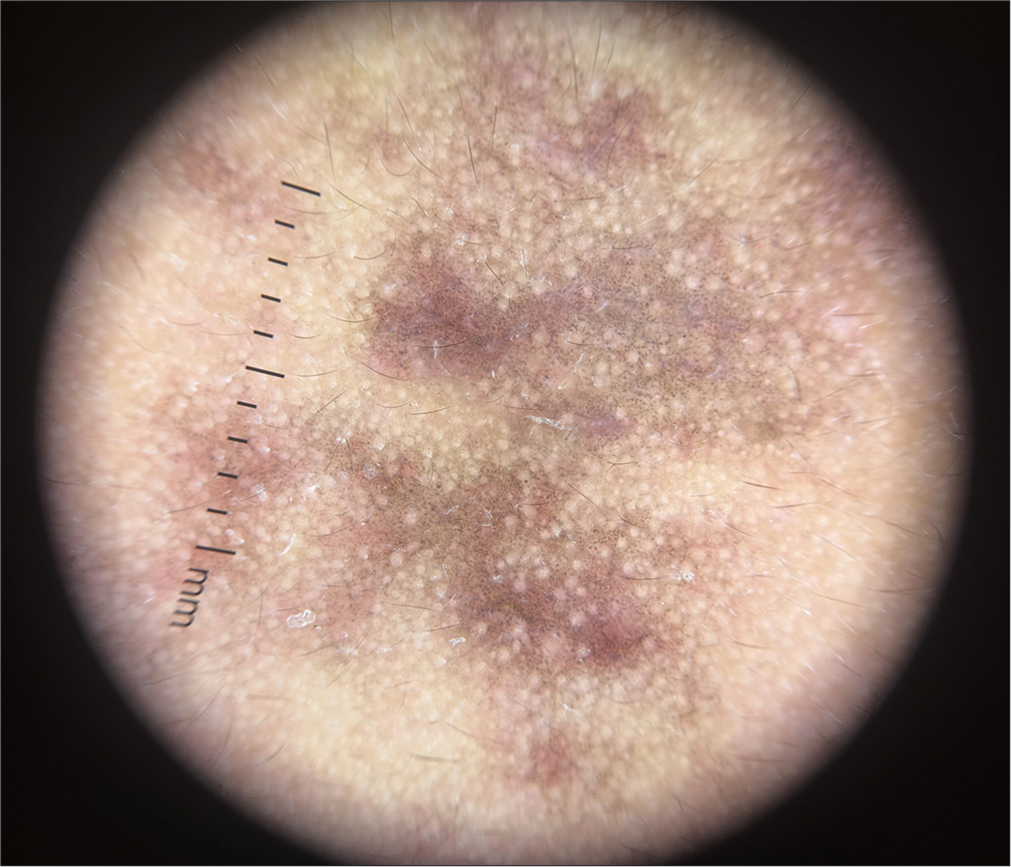
- Dermatoscopic features before treatment visualized with polarized light at 10x magnification shows irregularly distributed bluish grey and brown pigment dots (peppering) and globules in a background of patchy erythema with violaceous hue with some areas of perifollicular and perieccrine accentuation of pigment pseudo network.
We initially treated her with topical steroids and tacrolimus for 4 months. There was no disease progression but hyperpigmentation and atrophy persisted. She was then started on a monthly 1064 nm QSNY laser (HeliosIII; Laseroptek, South Korea) with a 5–8 mm spot size, 1.2–2 J/cmsq. Alongside, we performed microneedling with a pen device every 2 months at 2 mm depth, 10 passes or until pinpoint bleeding. Over 18 months, she received a total of 12 QSNY and 5 microneedling sessions, with significant esthetic and dermoscopic improvement [Figures 3 and 4]. She no longer needed to conceal the scar, improving her DLQI score to 3. At 1 year follow-up, she remained disease-free without any relapse.

- Clinical photograph after 18 months of treatment: Almost complete resolution of the scar.
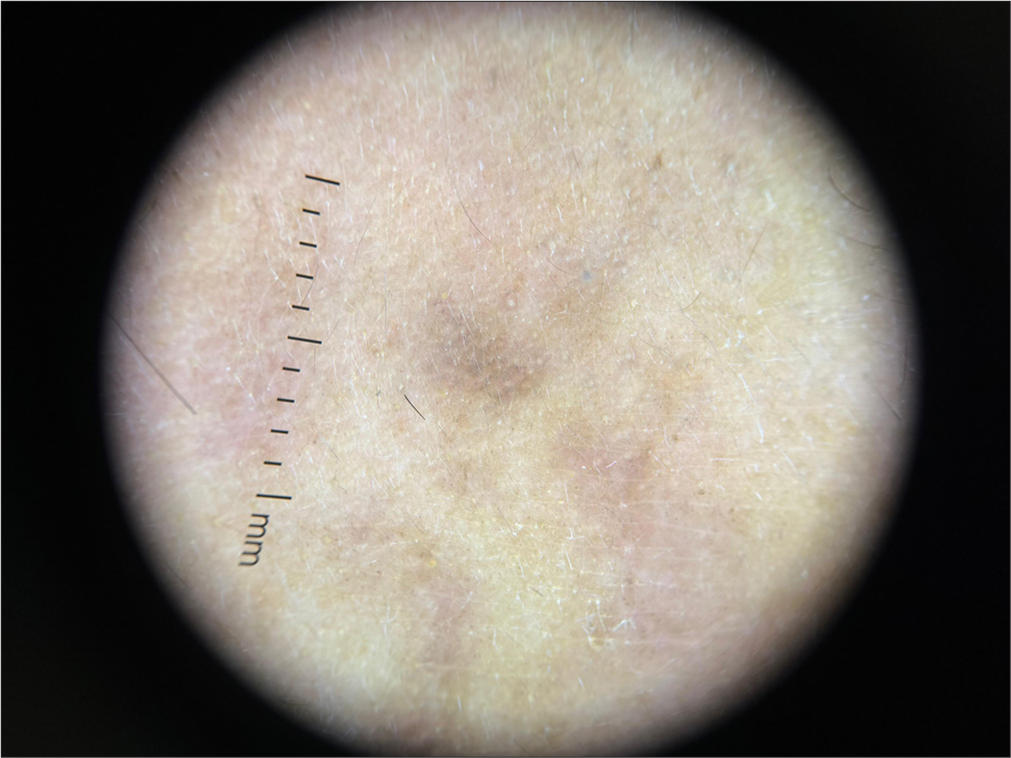
- Dermatoscopic features after treatment visualized with polarized light at 10x magnification shows significantly reduced erythema with minimal dark brown dots.
DISCUSSION
LP is a chronic idiopathic inflammatory skin disease affecting skin, mucous membranes, hair, and nails, having a prevalence of 0.5–1% of the population.1 Clinical variants of LP can be mucosal, lichen planopilaris (LPP), hypertrophic, atrophic, linear, LP pigmentosus (LPPig), bullous, etc.1 Linear LP along the lines of Blaschko is rare, accounting only for about 0.2% of LP cases.2 Linear LP of the face is even rarer, with only a handful of reported cases.1,3
LP may occur along a line as seen during koebnerization; however, linear LP occurs unilaterally along Blaschko’s lines, suggesting cutaneous mosaicism along migration lines of ectodermal cells during embryogenesis.3,4 The final lesion occurs following an unknown trigger warranting a mosaic T-cell response attacking these immunologically susceptible cells with different antigenic profiles.3,4
Merio et al. published six similar cases with Blaschko-linear facial LP with a literature review of 24 previously published similar cases, all with the following characteristics – not associated with oral or other skin lesions, mean age of 40 years, male predominance, linear disposition along Blaschko’s lines, predominance of mandibular topography, and hyperpigmentation and atrophy as sequelae with histopathology suggestive of LPP.1 The degree of hyperpigmentation was higher in Fitzpatrick skin types 4 and 5. A more recent case series by Kothari et al. on the rare clinical presentation of linear LPP of the face also had similar clinical and dermoscopic features to our patient.5 Most of these reported Blaschko-linear LP of face case reports and series consistently seem to have a combination of features shared between LPP and LPPig, with Kennedy et al. proposing the term ‘linear lichen planopilaris pigmentosus’ to describe this hybrid entity.1,3,5
The clinical differential diagnoses of pigmented linear dermatosis distributed along the lines of Blaschko that may result in atrophy include linear DLE which starts as photosensitive scaly erythematous plaques, lichen sclerosus et atrophicus (LSA) that is rare over the face and presents as porcelain white papules and plaques, linear atrophoderma of Moulin that is more common over trunk and extremities in children, Blaschkitis or adult lichen striatus which is more common over the trunk, and linear morphea which presents commonly as a wide, vertical depression over the forehead.1,5
Among reported cases of linear LP, there is no therapeutic consensus and not much focus on post-LP pigmentation and atrophy. Most topical regimens using a combination of retinoids, corticosteroids, and calcineurin inhibitors resulted in little or no change in the lesions.1 Topical depigmenting agents such as 4% hydroquinone, triple combination, azelaic acid, and chemical peels have been tried with minimal improvement due to dermal depth of pigment incontinence.6
Certain oral medications, namely hydroxychloroquine, cyclosporine A (CysA), and steroids have achieved suboptimal responses of limiting disease progression with persistent hyperpigmentation or atrophy except in the case of Yanaru et al., who reported successful treatment of facial linear LPP with low-dose CysA over 5 months with minimal residual pigmentation.1,3,5,7
Asz-Sigall et al. published a case report and review of linear LPP of the face in which they initially treated with topical steroids and tacrolimus followed by pulsed dye laser and hyaluronic filler with moderate esthetic results.8 Hyaluronic acid fillers are used for facial atrophy, depressed scars, and morphea, but they provide only temporary improvement.9 Jung et al. successfully treated 2 Korean women with linear LPPig of the chin with a combination of fractional lasers and intralesional polydeoxyribonucleotide injections.10 Kim et al. showed significant cosmetic improvement in a case of linear LPPig of the forehead using a combination of topical tacrolimus and QSNY.11 Bhari et al.’s pilot study of QSNY on LPPig documented poor/modest results both clinically and histologically.12
We used a novel combination of microneedling and QSNY, achieving excellent cosmetic results and DLQI improvement. Treating Indian skin tones (Fitzpatrick IV-VI) is safest with the 1064 nm QSNY, which works by selective photothermolysis, disrupting melanin pigment in the papillary dermis with subsequent clearance of melanophages.12 Microneedling involves repetitive skin puncture using sterile microneedles to disrupt dermal collagen that connects scar tissue creating micro conduits that stimulate collagen and elastin production with the release of growth factors in dermal vasculature without any damage to stratum corneum.13 This improved the atrophic nature of scars in our case.
CONCLUSION
We present a rare case of achieving remarkable esthetic improvement in hyperpigmentation and atrophy in Blaschko-linear LP of the face in an Indian Fitzpatrick type 4 patient, with an innovative combination of QSNY microneedling, with no recurrence post 1 year of therapy, significantly enhancing the patients quality of life. Among the few reports on this rare LP variant, our case stands out for its innovative approach and successful outcome.
Author contribution
All the authors contributed equally to the manuscript writing.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Blaschko-linear lichen planus of the face: A retrospective study of 6 cases and a literature review. Ann Dermatol Venereol. 2022;149:112-8.
- [CrossRef] [PubMed] [Google Scholar]
- Linear lichen planus pigmentosus of the face with histological findings of lichen planopilaris-an uncommon variant of lichen planus. Dermatol Online J. 2021;27:10.
- [CrossRef] [Google Scholar]
- Cutaneous mosaicisms: Concepts, patterns and classifications. An Bras Dermatol. 2013;88:507-17.
- [CrossRef] [PubMed] [Google Scholar]
- A case series on a rare clinical presentation of lichen planopilaris restricted to the face. Cureus. 2024;16:e59987.
- [CrossRef] [Google Scholar]
- A case of lichen planus pigmentosus with facial dyspigmentation responsive to combination therapy with chemical peels and topical retinoids. J Clin Aesthet Dermatol. 2016;9:44-50.
- [Google Scholar]
- Linear lichen planopilaris of the face treated with low-dose cyclosporin A. Acta Derm Venereol. 2000;80:212.
- [CrossRef] [PubMed] [Google Scholar]
- Linear lichen planopilaris of the face: Case report and review. Skin Appendage Disord. 2016;2:72-5.
- [CrossRef] [PubMed] [Google Scholar]
- Hyaluronic acid in facial rehabilitation-a narrative review. Cosmetics. 2023;10:61.
- [CrossRef] [Google Scholar]
- Two cases of linear lichen planus pigmentosus of the chin in Korean women treated by fractional lasers and polydeoxyribonucleotide injection. Ann Dermatol. 2023;35(Suppl 1):S38-42.
- [CrossRef] [PubMed] [Google Scholar]
- Linear lichen planus pigmentosus of the forehead treated by neodymium: yttrium-aluminum-garnet laser and topical tacrolimus. J Dermatol. 2012;39:189-91.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of Q-switched Nd-YAG laser on the clinical, pigmentary, and immunological markers in patients with lichen planus pigmentosus: A pilot study. Dermatol Ther. 2020;33:e13208.
- [CrossRef] [Google Scholar]
- Microneedling in the treatment of atrophic scars: A systematic review of randomised controlled trials. Int Wound J. 2021;18:577-85.
- [CrossRef] [PubMed] [Google Scholar]




