
Translate this page into:
Aspiration of lipoma: Effective use of liposuction
*Corresponding author: Nilesh N. Goyal, Department of Dermatology, Lilavati Hospital and Research Centre, Bandra West, Mumbai 400050, Maharashtra, India. getyoung@juvenis.in
-
Received: ,
Accepted: ,
How to cite this article: Dodani J, Goyal NN. Aspiration of lipoma: Effective use of liposuction. J Cutan Aesthet Surg. doi: 10.4103/JCAS.JCAS_49_23
Abstract
Lipomas tend to be surgically excised leaving big scars which often are not liked by patients. Liposuction offers an alternative solution especially for large lipomas, wherein complete resolution can occur with hardly any complications and above all minimal scar at wound site.
Keywords
Lipoma
Liposuction
Scarless

INTRODUCTION
Lipoma is a common benign tumor composed of mature fat cells enclosed in a capsule under the skin.1 They are often painless which become a cosmetic sore once they grow. Though a subcutaneous swelling which was dealt with by surgeons, these days lipomas are presenting very frequently in dermatology clinics. Surgical excision is the conventional treatment for lipomas.2 This entails a large incision followed by enucleation of the lipoma with its capsule which eventually heals with a scar. However, other techniques which are less scarring have been described. Narrow hole extrusion technique is a variant which aids in squeezing the fat cells out of a small incision made over the lipoma. This technique, however, does not ensure complete removal of the lipoma capsule.
We describe a relatively newer indication of liposuction that can help in treating lipomas. Liposuction is traditionally designed to take out fat from under the skin using tumescent local anesthesia as in Dermatologic Liposuction Surgery or under systemic anesthesia as done by the surgeons.3 Large lipomas of more than 5 cm especially on cosmetically relevant areas of body can be treated using principles of Dermatologic Liposuction Surgery.
CASE REPORT
A 24-year-old laser hair technician working at a dermatology clinic presented with a 4 cm × 8 cm painless skin colored banana shaped swelling on right side of chest under the clavicle of 5-year duration during which it had gradually grown to present day size [Figure 1]. An ultrasonogram of the growth confirmed it to be a lipoma with no intramuscular extensions or overlying adhesions. Her main concern was about scarring after surgery and hence was reluctant to get it done. She was hence offered liposuction of the growth. On the day of surgery, a dilute solution of lidocaine 2% with adrenaline 10 mL and sodium bicarbonate 0.5 mL was made in 30 mL of normal saline and injected within the lipoma with a 20G long spinal needle [Figure 2]. Some of the solution was also injected underneath the lipoma. This was then allowed to wait for 15 min. Once the lipoma was numb and pale in color, a 1.5 mm punch was used to make an entry point at its lower pole [Figure 3]. A blunt-tipped cannula of 2.4 mm diameter with serrated edges at its apertures attached to a 10 mL Luer lock syringe was inserted through this hole into the lipoma [Figures 4 and 5]. The piston of the syringe was pulled back with the cannula apertures inside the lipoma creating a suction within the syringe. To-and- fro motion of the cannula and syringe system aided with pressure from the left hand, allowed fat to enter the syringe [Supplementary Video 1]. This was continued till it was ascertained that no more fat persisted in the lipoma. Because of the small size of the lipoma, the suction would be lost every time the cannula holes got exposed to the outside. This cannula suction system had to be recreated every time. An attempt was also made to remove as much of the lipoma capsule as possible [Figures 6 and 7]. The area was then dressed after application of antiseptic ointment to the entry point. A tight compression dressing with Dynaplast® was given to maintain adequate pressure on the treated area. This was done to prevent bruising and blood collection within the lipoma. Appropriate oral antibiotics and painkillers were prescribed for a week.

- Lipoma banana shaped in a subclavicular area.
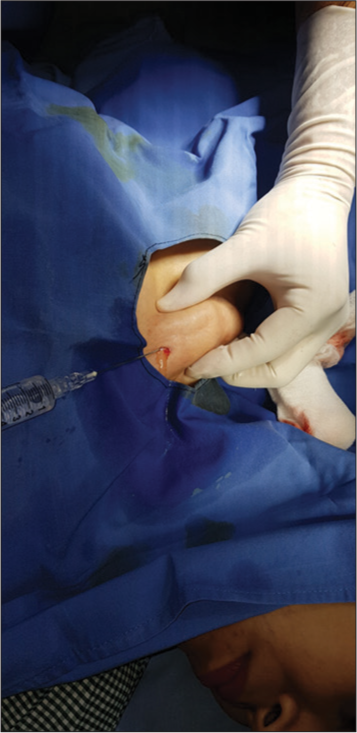
- Tumescent anesthesia infiltrated into lipoma with a 20G spinal needle.

- Lipoma tumesced post infiltration.

- Bensimon micro sculptor cannula with sharp jagged aperture openings.
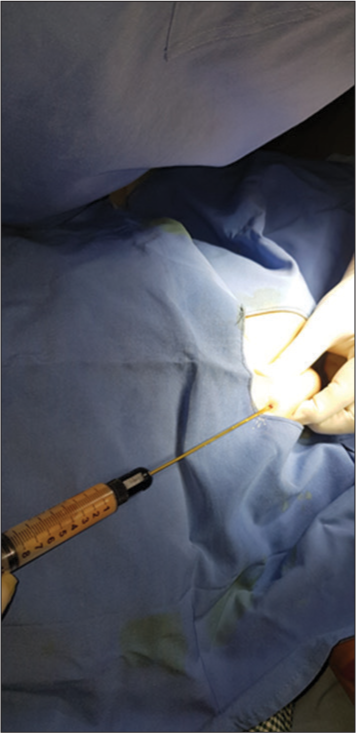
- Aspiration of fat from lipoma with a 10 Luer lock syringe.
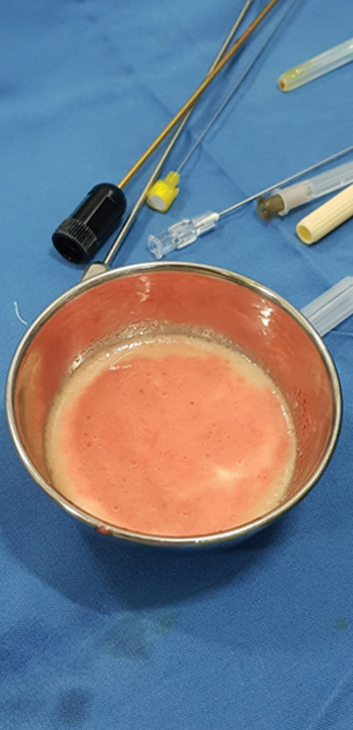
- Aspirated fat in a bowl.

- Post op view of treated lipoma.
The patient was called after 1 week for dressing review. The area had healed well with no collections and minimal bruising. Complete healing took place by 2 weeks [Figure 8].

- Complete resolution and healing of treated area after 2 weeks.
DISCUSSION
Liposuction has become an integral alternative in the management of subcutaneous lipoma. It has numerous advantages which include minimal incisions, shorter operation time, reduced blood loss, faster postoperative recovery, and reduced wound healing complications, and the most vital point is its superior cosmetic result following treatment. The one limitation of liposuction is the size of lipoma. Very small lesions would be difficult to treat with liposuction as there would be no space for the cannula tip to stay within the lipoma for creation of syringe suction. The authors feel that lipomas above 3 cm can be very well dealt with using liposuction.
Surgical excision is a widely popular technique in the treatment of lipomas. However, it involves large incisions and a multilayered closure with a greater risk of bleeding and postoperative wound complications.2 Although surgical excision is effective, this modality is associated with scarring.1
The resulting scar could become hypertrophic or keloidal, with significant disfigurement and cosmetic concerns, especially with lesions located on the exposed parts of the body. Bigger and deep infiltrating lipomas would require excisions under general anesthesia in an operating room which adds to the cost factor and possible morbidity. Hence, this raises concern which in turn makes liposuction a better option overall.
Dermatologists trained and practicing Dermatologic Liposuction Surgery can easily conduct this procedure in their day surgery centers. The use of liposuction under tumescent local anesthesia technique has made the procedure significantly safe and effective in reaching the goal of body shaping. Till date there have been no deaths across the world when principles of Dermatologic Liposuction Surgery have been adhered to.
Another modality of treatment which involves a small incision through a narrow hole is called narrow hole extrusion technique. A minor circular punch defect is created in the skin and the fat is extruded out by applying lateral pressure.4 However, large lipomas with adherent large cysts would need open dissection. Hence, this treatment is only suitable for very small lipomas.
Nevertheless, liposuction being a simpler procedure, albeit with a long learning curve, has its potential benefits for all patients presenting with lipomas, especially those with multiple lesions and tendency for poor scarring.5
CONCLUSION
Aspiration of Lipoma though not the commonly practiced treatment modality in the surgical world, it offers a different perspective. It can be indicated in areas where a scar would not be acceptable to the patient. A thoroughly done procedure can ensure complete removal of the lipoma and its sac with no chances of recurrence.
Authors’ contributions
Jessica Dodani has helped in creating the manuscript. Nilesh N Goyal has performed the procedure and managed the patient before and after the procedure.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Treatment of lipomas assisted with tumescent liposuction. J Eur Acad Dermatol Venereol. 2007;21:243-6.
- [CrossRef] [Google Scholar]
- Experience with liposuction for the treatment of subcutaneous lipoma: A case series from a tertiary health institution in Nigeria. J West Afr Coll Surg. 2022;12:117-21.
- [CrossRef] [Google Scholar]
- The use of suction-assisted surgical extraction of moderate and large lipomas: Long-term follow-up. Aesthetic Plast Surg. 2002;26:114-7.
- [CrossRef] [Google Scholar]
- Novel uses of skin biopsy punches in dermatosurgery. Indian J Dermatol. 2015;60:170-5.
- [CrossRef] [Google Scholar]
- The treatment of atypical lipoma with liposuction. J Dermatol Surg Oncol. 1991;17:332-4.
- [CrossRef] [Google Scholar]




