
Translate this page into:
Bicalutamide: A review

*Corresponding author: Dr. Venkataram Mysore, Department of Dermatology, Venkat Charmalaya - Centre for PG training and Advanced Dermatology, Affiliated to Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka, India. drvenkat@venkatcenter.com
-
Received: ,
Accepted: ,
How to cite this article: Aulakh S, Mysore V. Bicalutamide: A review. J Cutan Aesthet Surg. 2025;18:78-85. doi: 10.25259/jcas_182_23
Abstract
Bicalutamide is a non-steroidal androgen receptor antagonist that exerts anti-androgenic effects on peripheral tissues. It has been recently of interest in female pattern hair loss and has led to the off-label use of this drug for the improvement of Sinclair grading in such patients. This review aims to discuss the pharmacological properties along with indications, contraindications, and safety profile of bicalutamide for its use in dermatological research.
Keywords
Alopecia
Androgen Receptor
Anti-androgen drug
Bicalutamide
Female pattern hair loss

INTRODUCTION
Androgen receptor (AR) is a ligand-dependent transcriptional factor located on the X chromosome. It is known to be located in a diverse range of tissues including bone, muscle, prostate, adipose tissue, and the reproductive, cardiovascular, immune, neural, and hematopoietic systems.1
In the skin and subcutaneous tissues, ARs are found in the majority of keratinocytes within the epidermis, approximately 10% of fibroblasts in the dermis, as well as in the basal cells of sebaceous glands, sebocytes, and dermal papillary cells of hair follicles.2 The localization of AR in hair follicles subdues the dermal papillary cells to undergo regression, producing progressive hair follicle miniaturization and subsequently the conversion of terminal hair follicles into vellus hair follicles.3
Classic anti-androgen therapies to combat hyperandrogenism or increased peripheral sensitivity include drugs such as ketoconazole, spironolactone, cyproterone acetate, and flutamide [Figure 1].4
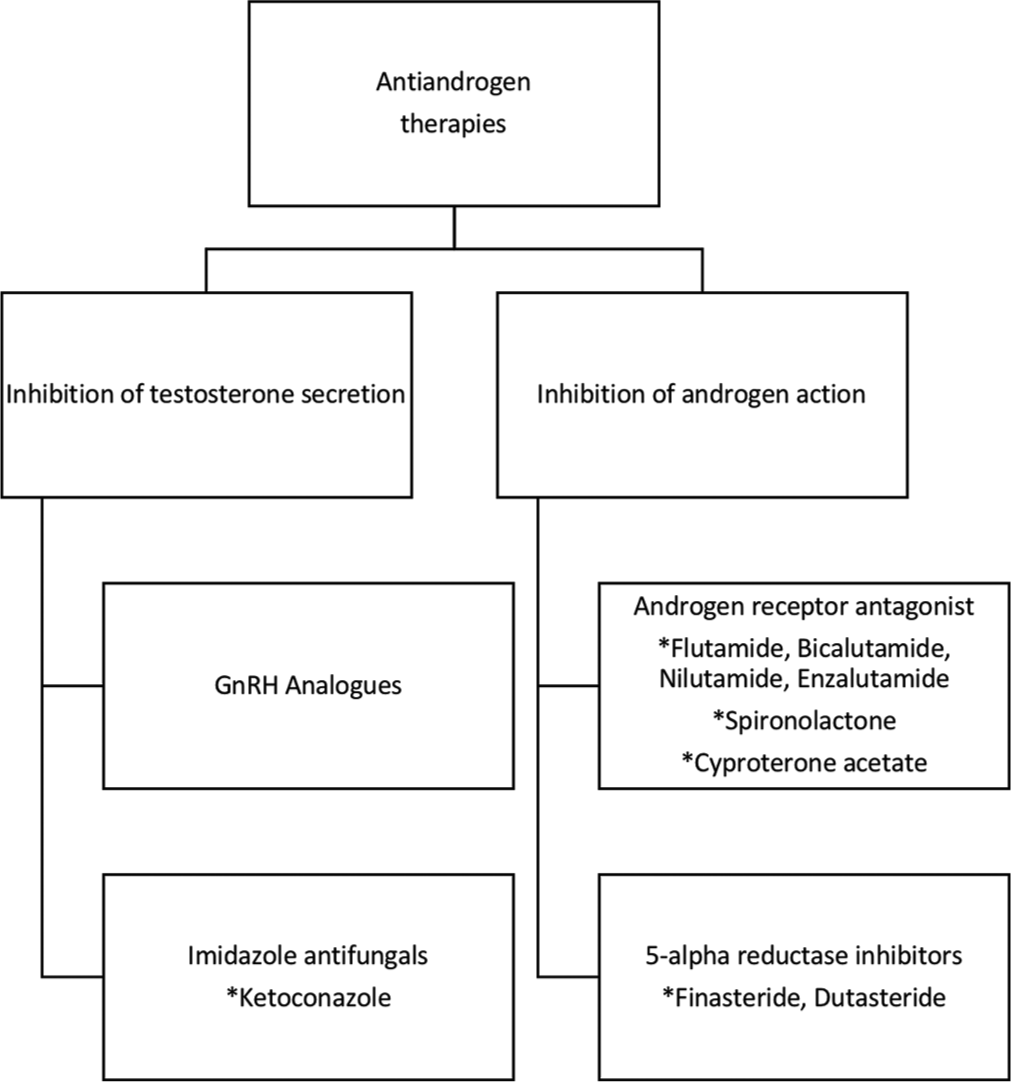
- Classification of anti-androgen therapies. GnRH: Gonadotropin-releasing hormone. *Name of compounds(drugs) under the pharmaceutical classes
Bicalutamide is a member of the non-steroidal AR antagonists group of drugs. These groups of drugs modulate the action of ARs by antagonistic action. This group of drugs includes flutamide, bicalutamide, nilutamide enzalutamide, apalutamide, and darolutamide. They were first approved for their use in prostate cancer in conjunction with gonadotropin-releasing hormone (GnRH) analogs.5
CHEMICAL STRUCTURE
Flutamide is a substituted anilide. Bicalutamide is derived synthetically after the structural modification of flutamide. The systematic name of bicalutamide is (RS)-N-[4-cyano-3-(trifluoromethyl)phenyl]-3-[(4-fluorophenyl)sulfonyl]-2-hydroxy-2-methylpropanamide. Its chemical structure is shown in Figure 2. A racemic mixture of an equal proportion of R and S enantiomers forms the final proprietary release formulation of bicalutamide.6
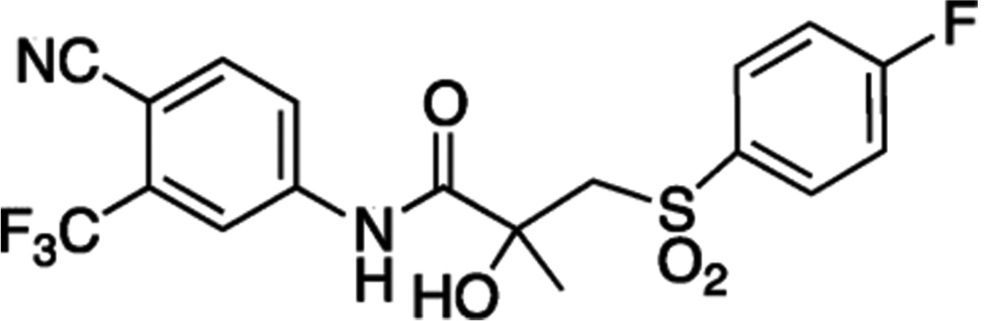
- Chemical structure of bicalutamide. NC: Cyano group, F3C: Trifluoromethyl group, SO2: Sulfonyl group, OH: Hydroxy group, NH: amide group.
PHARMACOKINETICS AND PHARMACODYNAMICS
Bicalutamide is well absorbed from gut mucosa and its absorption is not affected by food. It follows a linear absorption coefficient. The tissue distribution of bicalutamide is not well documented; however, it is known to cross the blood-brain barrier, causing central anti-androgenic effects as well. It is metabolized by the liver. Its R enantiomer is hydroxylated by the enzyme CYP3A4 into R-hydroxy bicalutamide and the S enantiomer is rapidly glucuronidated without hydroxylation.7 In severe hepatic impairment, the elimination half-life of the active (R)-enantiomer of bicalutamide is increased by about 1.75-fold (76% increase; elimination half-life of 5.9 and 10.4 days for normal and impaired patients, respectively). It is highly protein-bound and is mainly excreted through urine. However, the elimination half-life of bicalutamide remains unchanged in renal impairment.8
Indications: Bicalutamide is Food and Drug Administration (FDA)-approved for the treatment of carcinoma prostate. It is used off-label for various indications such as androgenetic alopecia in females (female pattern hair loss [FPHL]), hirsutism, frontal fibrosing alopecia (FFA), seborrhea, acne, hidradenitis suppurativa (HS), feminization of transgender women, precocious puberty in boys, chemical castration, and priapism.
MECHANISM OF ACTION
Female Pattern Hair Loss (FPHL)
The synthesis of testosterone is from glandular as well as extra-glandular sites. In males, the primary production of testosterone is from the testis, under the influence of the feedback loop of GnRH, luteinizing hormone (LH), and follicle-stimulating hormone secreted from the hypothalamic-pituitary axis.9 However, in females, the primary sources of testosterone synthesis are ovarian theca cells (regulated by LH) and the adrenal cortex. Androstenedione and dehydroepiandrosterone are likewise produced by the ovary and adrenal gland and are converted either to more potent androgens (e.g., testosterone and dihydrotestosterone [DHT]) or to estrogens in peripheral organs including skin.10
Serum testosterone concentration in women ranges from 15 to 65 ng/dL (0.5–2.3 nM). The average daily rate of testosterone production in women is approximately 0.25 mg, with about half of this daily output derived from the metabolic conversion of androstenedione to testosterone at extra-glandular sites, including the skin. Two peaks of androgen concentration parallel the peaks of plasma estrogens at the preovulatory and luteal phases of the menstrual cycle.11 Nevertheless, both forms – testosterone and DHT – bind to the peripheral AR, inducing a conformational change in the receptor. This alteration enables the movement of the receptor-ligand complex into the nucleus. The activated ARligand complex acts as a transcription factor and regulates gene expression. There is an alteration of the Wnt/b-catenin transcription pathway and secretion of transforming growth factor b, ultimately causing a shortened anagen phase and miniaturization of hair follicles. In disorders of androgen excess, such as polycystic ovarian syndrome (PCOS), or in local androgen abnormalities at cutaneous sites, due to either 5-a reductase or AR abnormalities, clinical conditions such as FPHL, hirsutism, and acne can be induced through this mechanism.12
Based on the understanding of the pathogenesis of FPHL, the AR can serve as a better target than DHT to tackle patterned hair loss, especially in females with or without other signs of virilization. The non-steroidal AR antagonists with no other hormonal activity competitively block androgen action on accessory sex organs and skin, typically reversing hair loss by inducing anagen.13 Studies done by Fernandez-Nieto et al. and Ismail et al. with an oral non-steroidal anti-androgen, bicalutamide, have shown 27.5% and 20.2% reduction in hair loss, respectively, at 6 months follow-up [Table 1].14,15 Fernandez-Nieto et al. studied a total of 44 patients with FPHL, who used doses of 25 mg/d in 15 patients and 50 mg/d in 29 patients. A total of 28 patients had coexisting comorbidities, namely, PCOS in 14 patients, seborrhea, acne, hirsutism, and alopecia (SAHA) syndrome in 6 patients, and hirsutism in eight patients. A total of 32 patients were evaluated after 6 months for response to treatment and showed a 27.5% reduction in the Sinclair scale. The side effects encountered in their study were a mild and transient increase of liver enzymes (<3 times the upper limit of normal) in five patients, hair shedding in 3, transient amenorrhea in 2, and endometrial hyperplasia, and headache in a single patient each.14
| Fernandez-Nieto et al.14 (N=44) | Ismail et al.15 (N=316) | Gomez-Zubiaur et al.16 (N=6) | |
|---|---|---|---|
| Mean age (in years) | 34.8 | 49.0 | 35.7 |
| Comorbidities | PCOS (14), SAHA (6), hirsutism (8) |
Seborrhea PCOS (2) Hirsutism (3) Abdominal obesity (4) |
|
| Mean treatment duration in months (duration range) |
10.5 (02–24) | 6.2 (02–69) | 6 |
| Bicalutamide dose mg (N) | 50 (29), 25 (15) | 10 (220), 12.5 (8), 20 (79), 25 (3), 30 (5), 50 (1) |
Mesotherapy With 1 mL of 0.5% bicalutamide solution Three Monthly sessions for 6 months |
| Concomitant treatments (N) | Oral minoxidil 0.5–1 mg (33) Topical 5% minoxidil (5) Finasteride 2.5 mg (1) Dutasteride 0.5–1 mg (7) Mesotherapy with dutasteride (6) |
Oral minoxidil (308) Spironolactone (172) |
None |
| Improvement | Sinclair stage at 6 months: 2.14 (27.5% reduction) |
Sinclair stage at 6 months: 2.21 (20.2% reduction) |
The degree of alopecia was not modified in any of the cases; however, in all cases, a subtle improvement in hair density was described after the third session, which did not persist at the 6-month visit. |
N: Sample size, PCOS: Polycystic ovarian syndrome, FPHL: Female pattern hair loss, SAHA: Seborrhea, acne, hirsutism, and alopecia
A more recent and potentially safer and more effective approach to treating this condition could involve the topical preparation of non-steroidal AR antagonists. These meso-solutions serve to target the scalp specifically, thus minimizing the risk of side effects in other parts of the body. In a study done by Gomez-Zubiaur et al., they used mesotherapy with 1 mL of 0.5% bicalutamide solution and noted a subtle improvement in hair density at 3 months [Table 1].16
Hirsutism
It is the presence of terminal coarse hairs in females in a male-pattern distribution. It is often part of PCOS along with acne, seborrhea, and patterned hair loss. Oral contraceptive pills (OCPs) are currently the primary treatment of choice in such patients. However, in a randomized control trial done by Moretti et al., they showed that OCPs combined with oral bicalutamide (50 mg/d) were more effective in treating severe hirsutism.17 Following this, Müderris et al. used low-dose oral bicalutamide (25 mg/d) as a standalone therapy for the treatment of hirsutism and found clinical improvement in the degree of hirsutism in all patients by a mean reduction in hirsutism scores of 41.2 ± 11.4% at 3 months and 61.6 ± 11.1% at 6 months.18
Notably, bicalutamide had also been shown to reverse minoxidil-induced hypertrichosis in FPHL by Moussa et al. in a case series of 35 patients. They commenced bicalutamide at a dose of 10 mg and gradually up-titrated it to a mean dose of 14.4 mg until no hypertrichosis was seen with concomitant oral minoxidil therapy.19 Therefore, oral bicalutamide may be useful for decreasing the risk of hypertrichosis as well, which is the most frequent adverse effect of oral minoxidil while improving Sinclair grading in FPHL patients.
The mechanism of bicalutamide in minoxidil-induced hypertrichosis is not entirely clear. However, there is a possibility that minoxidil might have an impact on the AR or its downstream signaling pathways, as mentioned by Moussa et al. in their paper.19 Another study reports that minoxidil suppresses AR-related functions, decreases AR transcriptional activity in reporter assays, and reduces the expression of AR targets at the protein level.20 Ironically, these noted observations bring into doubt the prior assertion that hypertrichosis induced by minoxidil is not influenced by androgens but is due to the stimulation of dermal papilla cells by various growth factors.21 This view rather prompts a reconsideration of the differentiation between hypertrichosis and hirsutism and needs a better understanding of the mechanism of the same.
Acne and seborrhea
Hormonal acne and seborrhea can be constituents of polycystic ovary syndrome or as part of SAHA syndrome. Lowering androgen concentrations or controlling their effect at the tissue level is a priority in the therapeutic strategy for such patients. Oral anti-androgen like bicalutamide can be combined with other therapies for non-responders and more effective results.22
Frontal Fibrosing Alopecia (FFA)
FFA is a patterned form of cicatricial alopecia, commonly encountered in postmenopausal females. The only report of bicalutamide use in FFA is published by Jerjen et al. They have mentioned the difficulty in determining if FFA represents androgenetic alopecia (AGA) with a lichenoid tissue reaction or patterned lichen planopilaris, hence the use of oral bicalutamide in their cohort along with low-dose oral minoxidil and other anti-androgens to clinically improve it.23
Hidradenitis Suppurativa (HS)
HS/acne inversa is a post-pubertal, chronic, inflammatory disorder of the hair follicle presenting as painful, deep-seated, and inflamed lesions in the apocrine gland-bearing areas of the body. In a systematic review by Zouboulis et al., their literature search cumulated 452 HS-associated druggable genes which they proposed as targets in HS and postulated that they can be repurposed as drugs for controlling HS, including AR ligands like bicalutamide.24
Feminization of transgender women
Anti-androgenic effects of bicalutamide can also form part of gender-affirming hormonal therapy along with a therapeutic armamentarium consisting of estrogens and progestins. This will add to the scope of practice for obstetricians and gynecologists with some modest expansion of the knowledge base required to prescribe this drug to their patients.25
Precocious puberty in boys
Familial male-limited precocious puberty is a GnRH-independent form of isosexual precocious puberty driven by androgens which promote virilization and growth. At present, there is no established treatment. Steroidal as well as non-steroidal anti-androgens can be used. However, Reiter et al. used the effective and favorable tolerability profile of bicalutamide as an anti-androgen along with anastrozole in 14 patients of precocious puberty. They showed an overall decreased growth rate, bone maturation rate, and less aggressive behavior with minimal changes in the Tanner stage in the testes, scrotum, and pubic hair in their study.26
Chemical castration
The role of testosterone in sexual offending is thought to be mediated by its effect on known risk factors for recidivism such as deviant sexual arousal and/or sexual preoccupation. Anti-androgenic effects of bicalutamide have been employed as chemical castration therapy along with psychosocial therapies in such patients.27
Priapism
Priapism is a disorder in which the penis maintains a prolonged, rigid erection in the absence of appropriate stimulation. It is a potentially devastating condition and may lead to penile fibrosis if untreated. Dahm et al. reported the use of 50 mg of bicalutamide in three patients, who not only experienced no further episodes of sustained priapism but also reported maintained libido and the ability to achieve sustained rigid erections for intercourse.28
Table 2 summarizes the comparative features of available AR blockers and their versatility of use in different indications, reported so far in the literature.29-31
| Drug | Mechanism of action | Relative potency | Side-effect profile | Selectivity and versatility of treating various condition |
|---|---|---|---|---|
| Bicalutamide | Competitive AR antagonist, with partial agonist action | 4.3 | Mild gynecomastia and breast tenderness, reversible hepatotoxicity, hyperlipidemia (favorable side effect profile with lesser gastrointestinal side effects) |
Carcinoma prostate, androgenetic alopecia in females (FPHL), hirsutism in females, frontal fibrosing alopecia, seborrhea, acne, hidradenitis suppurativa, feminization of transgender women, precocious puberty in boys, chemical castration, priapism |
| Flutamide | Competitive AR antagonist | 3.3 | Diarrhea, hepatotoxicity, photosensitivity | Carcinoma prostate, androgenetic alopecia in females (FPHL), hirsutism, acne and seborrhea, chemical castration, priapism |
| Enzalutamide | AR Full antagonist, inhibits binding | Data not available; apalutamide and enzalutamide are more efficacious agents for nmCRPC than dorlutamide | Fatigue, hypertension, Hot flushes, dizziness, nausea, seizure risk | Non-metastatic castration resistant prostate carcinoma (CRPC), metastatic CRPC |
| Apalutamide | Selective and competitive AR antagonist | Data not available; apalutamide and enzalutamide are more efficacious agents for nmCRPC than dorlutamide | Fatigue, hypertension, rash, diarrhea, nausea, weight loss, arthralgia, hot flushes and peripheral edema | Non-metastatic CRPC |
| Darolutamide | AR Full antagonist, inhibits binding | Data not available; apalutamide and enzalutamide are more efficacious agents for nmCRPC than dorlutamide | Fatigue, nausea, pain in extremities, rashes, ischemia, heart failure (most favorable safety profile out of enzalutamide, apalutamide) | Non-metastatic CRPC |
FPHL: Female pattern hair loss, CRPC: Castration-resistant prostatic carcinoma, nm: Non-metastatic, AR: Androgen receptor
DOSAGE
Bicalutamide is used in dosages of 150–200 mg/d for prostatic carcinoma followed by 50 mg/d in patients with concomitant GnRH analog use.32 It is available in 50 mg tablets in the market. In various studies so far, it has been used in FPHL in dosages varying from 12.5 mg to 50 mg 3–7 times per week. Ismail et al. have used a low-dose regimen of 10 mg daily in most of their patients.15 However, considering its relative safety profile than flutamide, much more efficacious results can be obtained at higher doses of 50 mg daily in FPHL of Sinclair grade 3 and 4.33 Similarly, the first reported dose of bicalutamide for use in hirsutism was also 50 mg/d but low doses of 25 mg/d and 15 mg/d have also been found effective.17-19
SIDE EFFECTS
Side effects reported so far with bicalutamide use are enumerated in Table 3. Anti-androgens are known to cause mild gynecomastia and breast tenderness (due to increased testicular estrogen production) along with mild reversible hepatotoxicity. Bicalutamide has fewer gastrointestinal side effects than flutamide. Symptoms such as nausea, vomiting, abdominal pain, fatigue, anorexia, flu-like symptoms, dark urine, and jaundice may indicate underlying hepatic dysfunction in patients on bicalutamide. In a study done by Fernandez-Nieto et al. (n = 44), there is a mild and transient increase of liver enzymes (3 times the upper limit of normal) in only five patients, that too not mandating its discontinuation in any of them.14 However, Ismail et al. (n = 316) have reported it in nine patients, out of which three discontinued.15 Although mentioned in the literature, libido, and potency are largely preserved with the anti-androgenic effect of the bicalutamide group, even in males, contrary to as seen with 5-alpha reductase inhibitors, that is, finasteride and dutasteride.28,34 Bicalutamide has also been found to increase serum lipid levels in women, especially those having pre-existing deranged cardiometabolic profiles and PCOS. It warrants regular monitoring of serum lipids while the patient is on oral treatment.17 Other reported side effects include myalgias and arthralgias, dyspnea, and photosensitivity.35-37
| Gynecomastia (in males) | Hepatotoxicity |
| Breast tenderness | Anemia |
| Mood changes (anxiety, depression, memory loss) | Edema feet and fluid retention |
| Weight gain | Gastrointestinal symptoms (nausea, diarrhea, constipation) |
| Potential teratogenicity (theoretical risk of feminization of the male fetus) | Abnormal uterine bleeding (endometrial hyperplasia) and amenorrhea |
| Difficulty in concentrating | Paradoxical hair shedding |
| Maculopapular rash, urticaria and angioedema | Myalgias and arthralgias |
| Decreased libido (rarely reported in males, not reported in females) | Acneiform eruption |
| Palpitations and dyspnea (Presents secondary to interstitial pneumonitis and subsequent pulmonary fibrosis) | Photosensitivity |
USE IN SPECIAL POPULATIONS
Bicalutamide is contraindicated in pregnant females (Pregnancy Category X). Hence, it should be used cautiously in females of childbearing age group and male patients with female partners of reproductive potential.38 Manufacturers advise to use an effective contraception during treatment and for 130 days after the final dose of bicalutamide.39 It is unknown if bicalutamide is secreted in breast milk; hence, it has not yet been recommended for use in lactating/breastfeeding females. Cautious use in patients of hepatic dysfunction and on drugs known to cause hepatic impairment is mandated. No dose modification is required in patients with renal impairment. No data are available for its use in the pediatric population in the case of adolescent-onset AGA, acne, and hirsutism.
WORKUP AND MONITORING
Baseline complete blood count, liver function tests, serum fasting lipid profile, and urinary pregnancy test should be ordered. The investigations should be repeated monthly during the initial 4 months and subsequently at regular intervals, particularly following any up-dosing schedule.39
DRUG INTERACTIONS
Bicalutamide is metabolized exclusively in the liver through the CYP3A4 enzyme. Hence, cautious use of CYP3A4 inducers (phenytoin, rifampicin, phenobarbital, and glucocorticoids) and inhibitors (ketoconazole, clarithromycin, diltiazem, erythromycin, itraconazole, ritonavir, and verapamil) is warranted. Food does not affect the absorption of oral bicalutamide.7 Hemorrhage with concomitant use of coumarin anticoagulant has been reported. Therefore, close monitoring of prothrombin time and international normalized ratio, and subsequent dose adjustment of the anticoagulant is required.40
FORMULATION
Bicalutamide is available in 50 mg tablet form for oral administration. No oral suspension or injectable preparations are available so far. Bicalutamide is potentially water-insoluble, it is hence physically micronized to smaller particle sizes to ensure better bioavailability through tablet form.41
CONCLUSION
AR antagonism theoretically serves as a better target than DHT to tackle patterned hair loss, especially in females. The encouraging results observed in studies suggest the potential for bicalutamide in FPHL patients. However, experience with the drug is limited, and hence, there is a need for further studies before its routine use. The drug’s reported safety and mechanism of action, however, offer promise for further investigation and application in the management of hair loss.
Authors’ contributions
Both the authors, Shayna Aulakh and Venkataram Mysore, discussed the analysis of the data, reviewed and edited the manuscript, and contributed to the concepts, design and preparation of the manuscript. Both the authors have diligently contributed to the literature search, incorporating intellectual content and in carrying out clinical studies. Venkataram Mysore being the reviewer and guarantor of the Manuscript.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Androgen receptor structure, function and biology: From bench to bedside. Clin Biochem Rev. 2016;37:3-15.
- [Google Scholar]
- Androgens and androgen receptor action in skin and hair follicles. Mol Cell Endocrinol. 2018;465:122-33.
- [CrossRef] [PubMed] [Google Scholar]
- Androgen receptor accelerates premature senescence of human dermal papilla cells in association with DNA damage. PLoS One. 2013;8:e79434.
- [CrossRef] [PubMed] [Google Scholar]
- Structure-activity relationship analysis of a series of nonsteroidal analogues as androgen receptor antagonists. New J Chem. 2021;45:1176-86.
- [CrossRef] [Google Scholar]
- Structural basis for antagonism and resistance of bicalutamide in prostate cancer. Proc Natl Acad Sci U S A. 2005;102:6201-6.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide: Clinical pharmacokinetics and metabolism. Clin Pharmacokinet. 2004;43:855-78.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide 150mg: A review of its use in the treatment of locally advanced prostate cancer. Drugs. 2006;66:837-50.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of estrogens in males and androgens in females. J Clin Invest. 2019;129:1818-26.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in serum testosterone during the menstrual cycle-an integrative systematic review of published literature. Gynecol Reprod Endocrinol Metab. 2022;3:9-20.
- [Google Scholar]
- Androgens in women: Androgen-mediated skin disease and patient evaluation. J Am Acad Dermatol. 2019;80:1497-506.
- [CrossRef] [PubMed] [Google Scholar]
- Female pattern hair loss and androgen excess: A report from the multidisciplinary androgen excess and PCOS committee. J Clin Endocrinol Metab. 2019;104:2875-91.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide: A potential new oral antiandrogenic drug for female pattern hair loss. J Am Acad Dermatol. 2020;83:e355-6.
- [CrossRef] [PubMed] [Google Scholar]
- Safety of oral bicalutamide in female pattern hair loss: A retrospective review of 316 patients. J Am Acad Dermatol. 2020;83:1478-9.
- [CrossRef] [PubMed] [Google Scholar]
- Mesotherapy with bicalutamide: A new treatment for androgenetic alopecia. Int J Trichology. 2023;15:39-40.
- [CrossRef] [PubMed] [Google Scholar]
- Combined oral contraception and bicalutamide in polycystic ovary syndrome and severe hirsutism: A double-blind randomized controlled trial. J Clin Endocrinol Metab. 2018;103:824-38.
- [CrossRef] [PubMed] [Google Scholar]
- New alternative treatment in hirsutism: Bicalutamide 25 mg/day. Gynecol Endocrinol. 2002;16:63-6.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide improves minoxidil-induced hypertrichosis in female pattern hair loss: A retrospective review of 35 patients. J Am Acad Dermatol. 2022;87:488-90.
- [CrossRef] [PubMed] [Google Scholar]
- Minoxidil may suppress androgen receptor-related functions. Oncotarget. 2014;5:2187-97.
- [CrossRef] [PubMed] [Google Scholar]
- Minoxidil promotes hair growth through stimulation of growth factor release from adipose-derived stem cells. Int J Mol Sci. 2018;19:691.
- [CrossRef] [PubMed] [Google Scholar]
- Etiopathogenesis and therapeutic approach to adult onset acne. Indian J Dermatol. 2016;61:403-7.
- [CrossRef] [PubMed] [Google Scholar]
- Clinicopathological characteristics and treatment outcomes of fibrosing alopecia in a pattern distribution: A retrospective cohort study. J Eur Acad Dermatol Venereol. 2021;35:2440-7.
- [CrossRef] [PubMed] [Google Scholar]
- Hidradenitis suppurativa and comorbid disorder biomarkers, druggable genes, new drugs and drug repurposing-a molecular meta-analysis. Pharmaceutics. 2021;14:44.
- [CrossRef] [PubMed] [Google Scholar]
- Gender-affirming hormone therapy for transgender female. Clin Obstet Gynecol. 2018;61:705-21.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide plus anastrozole for the treatment of gonadotropin-independent precocious puberty in boys with testotoxicosis: A phase II, open-label pilot study (BATT) J Pediatr Endocrinol Metab. 2010;23:999-1009.
- [CrossRef] [PubMed] [Google Scholar]
- The efficacy, safety and ethics of the use of testosterone-suppressing agents in the management of sex offending. Curr Opin Endocrinol Diabetes Obes. 2016;23:271-8.
- [CrossRef] [PubMed] [Google Scholar]
- Antiandrogens in the treatment of priapism. Urology. 2002;59:138.
- [CrossRef] [PubMed] [Google Scholar]
- Second-generation antiandrogens: from discovery to standard of care in castration resistant prostate cancer. Front Oncol. 2019;9:801.
- [CrossRef] [PubMed] [Google Scholar]
- Receptor affinity and potency of non-steroidal antiandrogens: Translation of preclinical findings into clinical activity. Prostate Cancer Prostatic Dis. 1998;1:307-14.
- [CrossRef] [PubMed] [Google Scholar]
- Apalutamide, enzalutamide, and darolutamide for non-metastatic castration-resistant prostate cancer: A systematic review and network meta-analysis. Int J Clin Oncol. 2020;25:1892-900.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide dosages used in the treatment of prostate cancer. Prostate. 1999;39:47-53.
- [CrossRef] [Google Scholar]
- Bicalutamide and the new perspectives for female pattern hair loss treatment: What dermatologists should know. J Cosmet Dermatol. 2022;21:4171-5.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide (Casodex®) in the treatment of prostate cancer: History of clinical development. Prostate. 1998;34:61-72.
- [CrossRef] [Google Scholar]
- Bicalutamide associated acute liver injury and migratory arthralgia: A rare but clinically important adverse effect. Case Rep Gastroenterol. 2018;12:266-70.
- [CrossRef] [Google Scholar]
- Interstitial pneumonitis induced by bicalutamide given for prostate cancer. Int J Clin Oncol. 2018;16:763-5.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-induced photosensitivity to bicalutamide-case report and review of the literature. Photodermatol Photoimmunol Photomed. 2016;32:161-4.
- [CrossRef] [PubMed] [Google Scholar]
- An overview of animal toxicology studies with bicalutamide (ICI 176,334) J Toxicol Sci. 1997;22:75-88.
- [CrossRef] [PubMed] [Google Scholar]
- Bicalutamide in advanced prostate cancer: A review. Drugs Aging. 1998;12:401-22.
- [CrossRef] [PubMed] [Google Scholar]
- Enhancement of solubility of bicalutamide drug using solid dispersion technique. Pharma Sci Monit. 2012;3:2739-48.
- [Google Scholar]




